PROCEDURE 6 Open Reduction and Internal Fixation of Intra-Articular Fractures of the Distal Humerus

Examination/Imaging



Surgical Anatomy
 Muscular anatomy (Fig. 1A): medial head, lateral head, and long head of the triceps; triceps tendon, intermuscular septum, flexor carpi ulnaris, anconeus, and extensor carpi ulnaris
Muscular anatomy (Fig. 1A): medial head, lateral head, and long head of the triceps; triceps tendon, intermuscular septum, flexor carpi ulnaris, anconeus, and extensor carpi ulnaris Neurologic anatomy (see Fig. 1A): radial nerve, ulnar nerve, and posterior antebrachial cutaneous nerve
Neurologic anatomy (see Fig. 1A): radial nerve, ulnar nerve, and posterior antebrachial cutaneous nerve Bony anatomy (Fig. 1B): medial and lateral epicondyles, trochlea, capitellum, olecranon fossa, and olecranon
Bony anatomy (Fig. 1B): medial and lateral epicondyles, trochlea, capitellum, olecranon fossa, and olecranon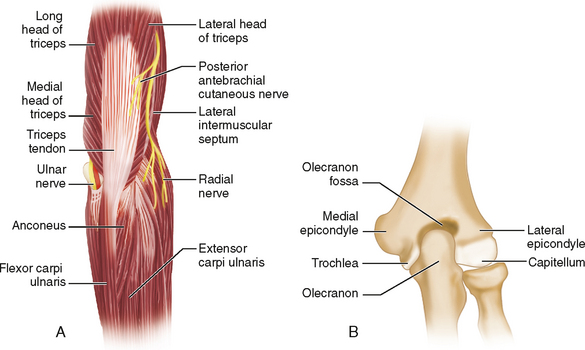
Positioning
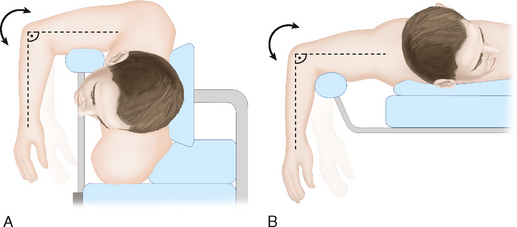
 The patient may be placed in the lateral decubitus position with the operative side facing upward (Fig. 2A) or, alternatively, the patient may be placed in the prone position (Fig. 2B).
The patient may be placed in the lateral decubitus position with the operative side facing upward (Fig. 2A) or, alternatively, the patient may be placed in the prone position (Fig. 2B).
Portals/Exposures
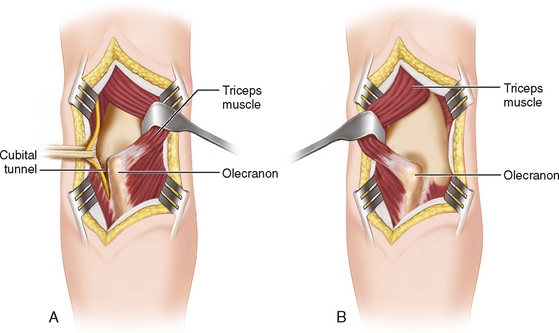
 Triceps-splitting approach
Triceps-splitting approach
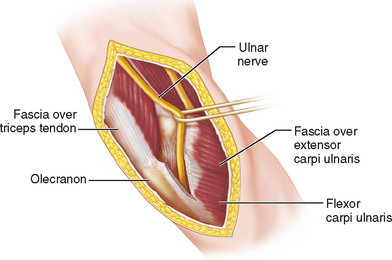
 Triceps-sparing approach
Triceps-sparing approach
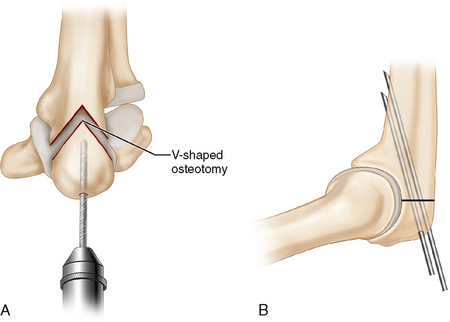
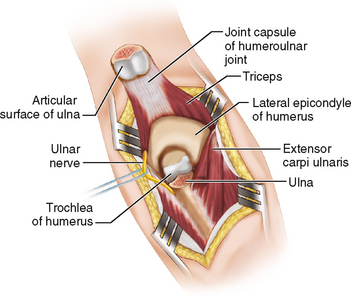
 Olecranon osteotomy approach
Olecranon osteotomy approach
Procedure
STEP 1
 Once the distal humerus has been appropriately exposed, the elbow should be flexed greater than 140° to provide greater access to the distal humerus.
Once the distal humerus has been appropriately exposed, the elbow should be flexed greater than 140° to provide greater access to the distal humerus.

 The reduction of the articular surface should be held provisionally with pointed reduction forceps and K-wires (Fig. 8B). Several 4.0-mm cancellous screws may then be used to rigidly stabilize the articular surface. The surgeon must take care to ensure that these screws do not enter the olecranon fossa or protrude through the articular surface and into the joint.
The reduction of the articular surface should be held provisionally with pointed reduction forceps and K-wires (Fig. 8B). Several 4.0-mm cancellous screws may then be used to rigidly stabilize the articular surface. The surgeon must take care to ensure that these screws do not enter the olecranon fossa or protrude through the articular surface and into the joint.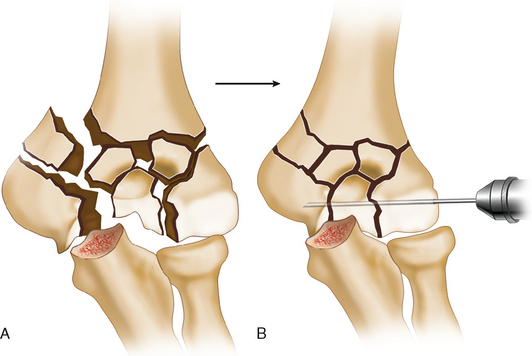
STEP 2
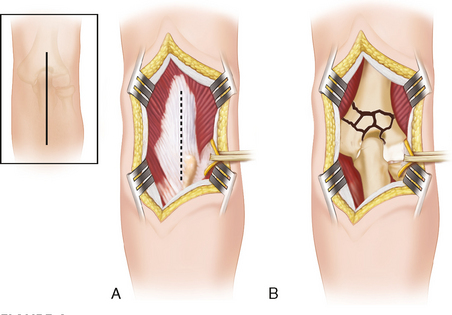
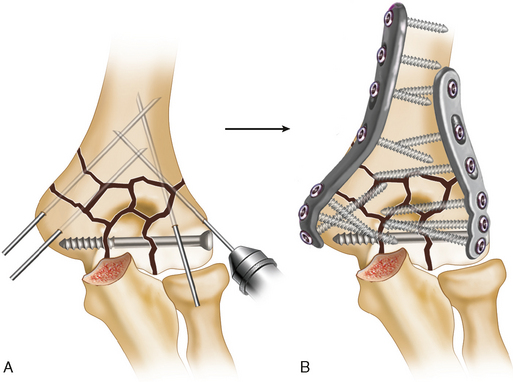
 After reduction of the articular surface, the nonarticular supracondylar component of the fracture is reduced and the articular surface is provisionally fixed to the humeral shaft using K-wires (Fig. 9A).
After reduction of the articular surface, the nonarticular supracondylar component of the fracture is reduced and the articular surface is provisionally fixed to the humeral shaft using K-wires (Fig. 9A). Rigid fixation of the fracture using two plates (one on each column) is mandatory (Fig. 9B). Either precontoured 3.5-mm periarticular distal humerus plates or 3.5-mm reconstruction plates may be used to provide rigid fixation.
Rigid fixation of the fracture using two plates (one on each column) is mandatory (Fig. 9B). Either precontoured 3.5-mm periarticular distal humerus plates or 3.5-mm reconstruction plates may be used to provide rigid fixation.
STEP 3
 Prior to closure, the elbow should be taken through a range of motion (flexion, extension, pronation, and supination) to ensure the elbow is stable and that there are no blocks to motion. The reduction and the position of the hardware should be checked using fluoroscopy.
Prior to closure, the elbow should be taken through a range of motion (flexion, extension, pronation, and supination) to ensure the elbow is stable and that there are no blocks to motion. The reduction and the position of the hardware should be checked using fluoroscopy. If a triceps-splitting approach was used, care must be taken to ensure the triceps tendon is appropriately repaired.
If a triceps-splitting approach was used, care must be taken to ensure the triceps tendon is appropriately repaired.


Postoperative Care and Expected Outcomes

Coles CP, Barei DP, Nork SE, Taitsman LA, Hanel DP, Bradford Henley M. The olecranon osteotomy: a six-year experience in the treatment of intraarticular fractures of the distal humerus. J Orthop Trauma. 2006;20:164-171.
Dakouré PW, Ndiaye A, Ndoye JM, Sané AD, Niane MM, Séye SI, Dia A. Posterior surgical approaches to the elbow: a simple method of comparison of the articular exposure. Surg Radiol Anat. 2007;29:671-674.
Doornberg JN, van Duijn PJ, Linzel D, Ring DC, Zurakowski D, Marti RK, Kloen P. Surgical treatment of intra-articular fractures of the distal part of the humerus: functional outcome after twelve to thirty years. J Bone Joint Surg [Am]. 2007;89:1524-1532.
Hewins EA, Gofton WT, Dubberly J, MacDermid JC, Faber KJ, King GJ. Plate fixation of olecranon osteotomies. J Orthop Trauma. 2007;21:58-62.
McKee MD, Kim J, Kebaish K, Stephen DJ, Kreder HJ, Schemitsch EH. Functional outcome after open supracondylar fractures of the humerus: the effect of the surgical approach. J Bone Joint Surg [Br]. 2000;82:646-651.
McKee MD, Veillette CJ, Hall JA, Schemitsch EH, Wild LM, McCormack R, Perey B, Goetz T, Zomar M, Moon K, Mandel S, Petit S, Guy P, Leung I. A multicenter, prospective, randomized, controlled trial of open reduction—internal fixation versus total elbow arthroplasty for displaced intra-articular distal humeral fractures in elderly patients. J Shoulder Elbow Surg. 2009;18:3-12.
McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR. Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg [Am]. 2000;82:1701-1707.
Figures 1, 5, 6, and 7 modified from Hoppenfeld S, deBoer P. Surgical Exposures in Orthopaedics: The Anatomic Approach. 3rd ed. Philadelphia: Lippincott Williams and Wilkins, 2003. Figures 2, 4, and 11B modified from AO Surgery Reference Online (www.aofoundation.org). Figures 3 and 10 modified from McKee MD, Kim J, Kebaish K, Stephen DJ, Kreder HJ, Schemitsch EH. Functional outcome after open supracondylar fractures of the humerus: the effect of the surgical approach. J Bone Joint Surg [Br]. 2000;82:646–51. Figures 8 and 9 modified from Jupiter JB, Neff U, Holzach P, Allgöwer M. Intercondylar fractures of the humerus. An operative approach. J Bone Joint Surg [Am]. 1985;67:226–39.




