[level-membership-for-critical-care-medicine-category]PROCEDURE 43
 Emergent Open Sternotomy (Perform)
Emergent Open Sternotomy (Perform)
PREREQUISITE NURSING KNOWLEDGE
• Knowledge of anatomy and physiology of the cardiovascular system is necessary.
• Advanced cardiac life support knowledge and skills are needed
• Understanding of the signs and symptoms of cardiac tamponade is necessary.
• Emergency open sternotomy is performed for patients who have undergone a median sternotomy, usually within the first 2 weeks of cardiac surgery.
• Emergent open sternotomy is indicated for exsanguinating hemorrhage or cardiac tamponade with imminent cardiac arrest.6,7
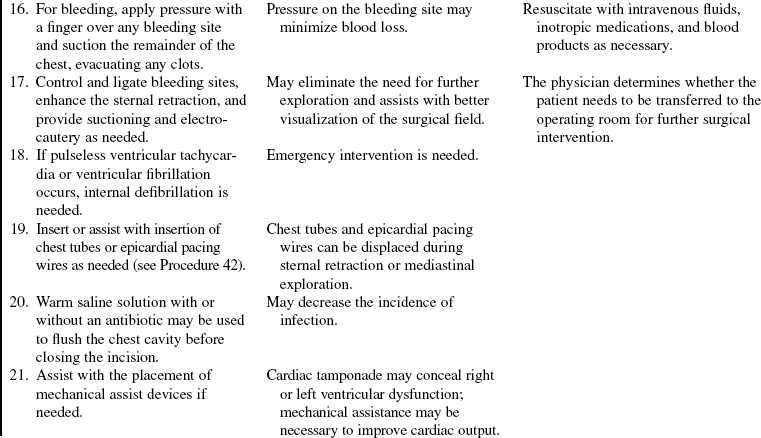
 The goal of mediastinal exploration for persistent hemorrhage is to stop the bleeding and retain circulating blood volume. The requirement for homologous blood transfusion and incidence of wound infection associated with an undrained mediastinal hematoma may be decreased.3
The goal of mediastinal exploration for persistent hemorrhage is to stop the bleeding and retain circulating blood volume. The requirement for homologous blood transfusion and incidence of wound infection associated with an undrained mediastinal hematoma may be decreased.3

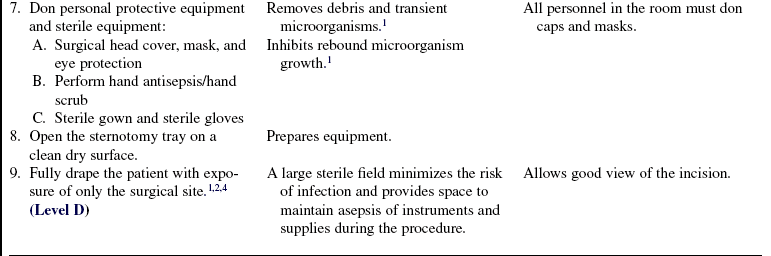
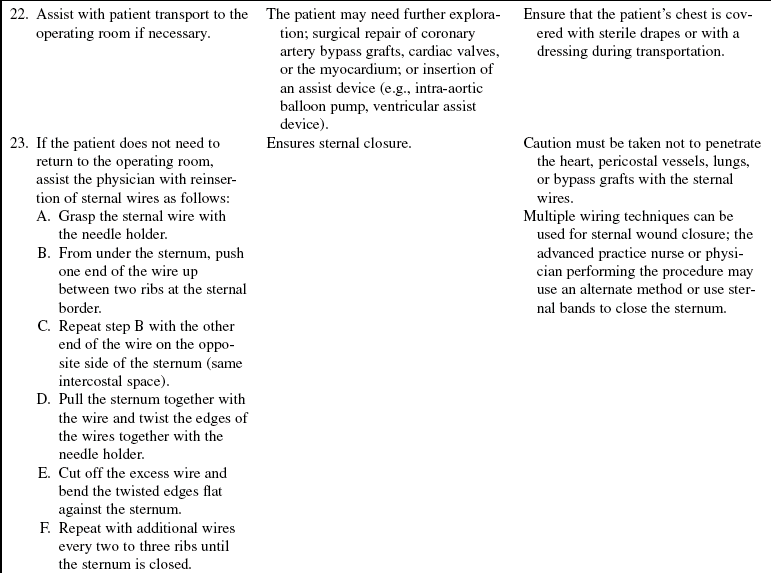
• Knowledge and skills related to aseptic and sterile technique, surgical instrumentation, sternal opening, sternal exploration, sternal closure, and suturing are needed.1,4–6
• Paralytic agents may be a necessary adjunct to sedation to improve oxygenation, diminish muscle activity, and enhance visualization.
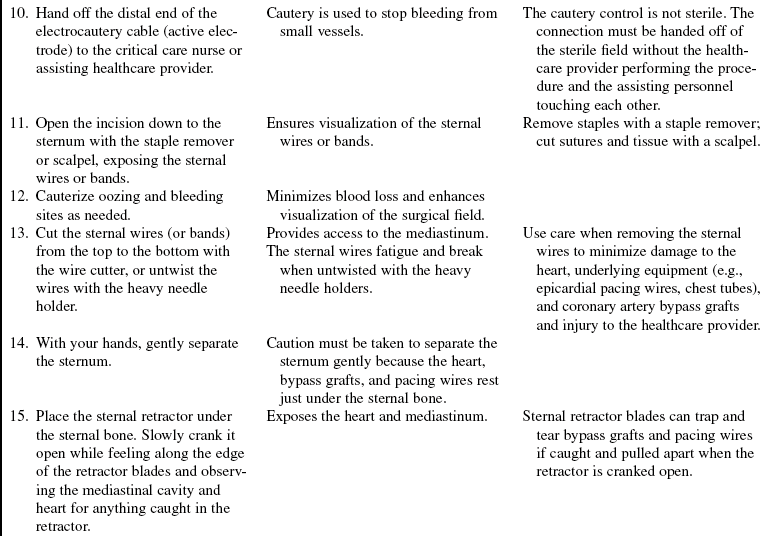
• Internal defibrillation may be necessary if life-threatening dysrhythmias occur (see Procedure 42).
EQUIPMENT
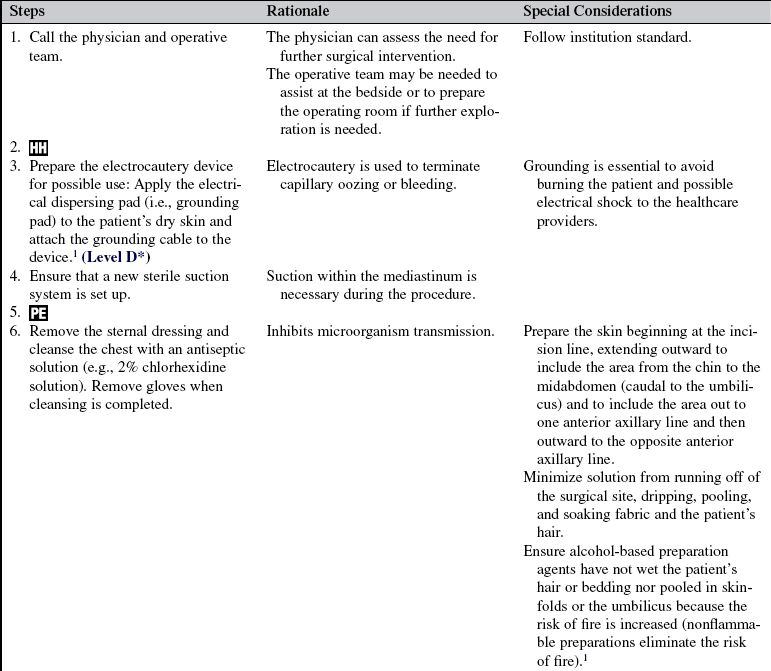
• Antiseptic solution (e.g., 2% chlorhexidine-based preparation)
• Head cover, masks, eye protection, sterile gown, sterile gloves, sterile drapes
• Sterile open-chest set and sternotomy tray





• Electrocautery equipment: Generator, cautery, electrical dispersing pad (e.g., grounding pad)
• Large sterile suction catheter (e.g., Yankauer)
• Suction containers, tubing, regulator, and suction source
• Radiopaque gauze or other surgical sponge materials
• Polypropylene (Prolene) suture (cutting needle) and other suture material according to preference
• Syringes: 3 ml, 5 ml, 10 ml, and 20 ml
• Knife blades: Nos. 10, 11, 15
• Emergency medication and resuscitation equipment, including internal defibrillation paddles and external defibrillation pads or paddles
Additional equipment as needed includes the following:
• Prescribed analgesia or sedation
• Prescribed blood products and intravenous solutions
• Defibrillator and compatible internal defibrillation paddles
• Warm saline solution with or without an antibiotic, as prescribed
• Chest tubes and chest tube drainage system
• Intra-aortic balloon pump or other mechanical assist device
• Peripheral nerve stimulator (used if paralytic agents are administered)
PATIENT AND FAMILY EDUCATION
• Teaching may not be provided until after the procedure.  Rationale: When an emergent sternotomy is performed for rapid hemodynamic collapse, education of the patient and family may not be possible prior to the procedure.
Rationale: When an emergent sternotomy is performed for rapid hemodynamic collapse, education of the patient and family may not be possible prior to the procedure.
• Explain the reason that the open sternotomy procedure was performed and its outcome or anticipated outcome.  Rationale: This explanation provides information and encourages the patient and family to ask questions and clarify details about the patient and procedure.
Rationale: This explanation provides information and encourages the patient and family to ask questions and clarify details about the patient and procedure.
PATIENT ASSESSMENT AND PREPARATION
Patient Assessment
• Assess hemodynamic and neurologic status.  Rationale: This assessment identifies baseline data that may indicate the need for emergent open sternotomy and provides comparison data.
Rationale: This assessment identifies baseline data that may indicate the need for emergent open sternotomy and provides comparison data.
• Assess the patient’s medical history, specifically for coagulation disorders, renal disease with coexistent uremia, and functional status of the right and left ventricle.  Rationale: Baseline data are obtained.
Rationale: Baseline data are obtained.
• Assess current laboratory data, specifically complete blood cell count, platelet count, international normalized ratio, activated partial thromboplastin time, and fibrinogen.  Rationale: Near-normal baseline coagulation study results decrease the likelihood of coagulopathy as a possible cause for ongoing hemorrhage.
Rationale: Near-normal baseline coagulation study results decrease the likelihood of coagulopathy as a possible cause for ongoing hemorrhage.
• Assess for signs and symptoms of cardiac tamponade:
 Sudden decrease or cessation in chest tube drainage
Sudden decrease or cessation in chest tube drainage
 Hypotension (mean arterial blood pressure, <60 mm Hg)
Hypotension (mean arterial blood pressure, <60 mm Hg)

 Apical heart rate greater than 110 beats/min
Apical heart rate greater than 110 beats/min




 Decreased cardiac output and cardiac index
Decreased cardiac output and cardiac index

 Rationale: The presence of some or all of these signs and symptoms assists the healthcare provider to decide whether an emergent open sternotomy is necessary.
Rationale: The presence of some or all of these signs and symptoms assists the healthcare provider to decide whether an emergent open sternotomy is necessary.
• Assess for excessive chest tube drainage.  Rationale: Presence of bleeding assists with the determination of the need for mediastinal exploration. Follow institution guidelines regarding determination of the timing of mediastinal exploration. One recommendation is when chest tube drainage continues at equal to or greater than 3 mL/kg/hr for at least 3 hours.2
Rationale: Presence of bleeding assists with the determination of the need for mediastinal exploration. Follow institution guidelines regarding determination of the timing of mediastinal exploration. One recommendation is when chest tube drainage continues at equal to or greater than 3 mL/kg/hr for at least 3 hours.2
Patient Preparation
• Verify correct patient with two identifiers.  Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
• Ensure that the patient and family understand procedural teaching (if time is available). Answer questions as they arise and reinforce information as needed.  Rationale: Understanding of the information provided is evaluated and reinforced.
Rationale: Understanding of the information provided is evaluated and reinforced.
• Obtain informed consent (may not be possible if the procedure is an emergency).  Rationale: Informed consent protects the rights of the patient and ensures a competent decision for the patient and the family.
Rationale: Informed consent protects the rights of the patient and ensures a competent decision for the patient and the family.
• Perform a pre-procedure verification and time out, if non-emergent.  Rationale: Ensures patient safety.
Rationale: Ensures patient safety.
• If time allows, obtain a transthoracic echocardiogram in an attempt to identify mediastinal fluid or clot and ventricular filling and wall motion.  Rationale: An echocardiogram aids in the diagnosis of effusion or tamponade and confirms the necessity for an open sternotomy.
Rationale: An echocardiogram aids in the diagnosis of effusion or tamponade and confirms the necessity for an open sternotomy.
• Ensure the patient’s airway is protected and that supplemental oxygen is delivered.  Rationale: The probability that the patient’s ventilatory needs will be met is enhanced.
Rationale: The probability that the patient’s ventilatory needs will be met is enhanced.
• Position the patient in the supine position with the head of the bed flat.  Rationale: This position ensures visualization of the chest and enhances hemodynamic stability.
Rationale: This position ensures visualization of the chest and enhances hemodynamic stability.
• Prescribe and ensure that an analgesic or sedative is administered.  Rationale: Promotes patient comfort.
Rationale: Promotes patient comfort.
References
1. AORN, Association of periOperative Registered NursesPerioperative standards and recommended practices. -Denver: AORN, 2008.
2. Chikwe, J, Beddow, E, Glenville, B. Cardiothoracic -surgery. New York: Oxford University Press Inc; 2006.
![]() 3. Mason, RJ, Broaddus, VC, Murray, JF, et al. Murray & Nadel’s textbook of respiratory medicine, ed 4. St Louis: Saunders; 2005.
3. Mason, RJ, Broaddus, VC, Murray, JF, et al. Murray & Nadel’s textbook of respiratory medicine, ed 4. St Louis: Saunders; 2005.
4. Phillips, N. Berry & Kohn’s operating room technique, ed 11. St Louis: Mosby; 2007.
5. Rothrock, JC. Alexander’s care of the patient in surgery, ed 13. St Louis: Mosby; 2007.
6. Sethares, K, Seifert, PC, Smith, H, Care of patients undergoing cardiac surgery. In Moser DK, Riegel B, editorsCardiac nursing: a companion to Braunwald’s heart -disease. St Louis: Saunders, 2008.
![]() 7. Soar, J, et al, European Resuscitation Council guidelines for resuscitation 2005 section 7. cardiac arrest in special circumstances. Resuscitation. 2005; 67(Suppl 1):S135–S170.
7. Soar, J, et al, European Resuscitation Council guidelines for resuscitation 2005 section 7. cardiac arrest in special circumstances. Resuscitation. 2005; 67(Suppl 1):S135–S170.
![]() This procedure should be performed only by physicians, advanced practice nurses, and other healthcare professionals (including critical care nurses) with additional knowledge, skills, and demonstrated competence per professional licensure or institutional standard.
This procedure should be performed only by physicians, advanced practice nurses, and other healthcare professionals (including critical care nurses) with additional knowledge, skills, and demonstrated competence per professional licensure or institutional standard.
[/level-membership-for-critical-care-medicine-category][not-level-membership-for-critical-care-medicine-category]PROCEDURE 43
Emergent Open Sternotomy (Perform)
PREREQUISITE NURSING KNOWLEDGE
• Knowledge of anatomy and physiology of the cardiovascular system is necessary.
• Advanced cardiac life support knowledge and skills are needed
• Understanding of the signs and symptoms of cardiac tamponade is necessary.
• Emergency open sternotomy is performed for patients who have undergone a median sternotomy, usually within the first 2 weeks of cardiac surgery.
• Emergent open sternotomy is indicated for exsanguinating hemorrhage or cardiac tamponade with imminent cardiac arrest.6,7
The goal of mediastinal exploration for persistent hemorrhage is to stop the bleeding and retain circulating blood volume. The requirement for homologous blood transfusion and incidence of wound infection associated with an undrained mediastinal hematoma may be decreased.3
• Knowledge and skills related to aseptic and sterile technique, surgical instrumentation, sternal opening, sternal exploration, sternal closure, and suturing are needed.1,4–6
• Paralytic agents may be a necessary adjunct to sedation to improve oxygenation, diminish muscle activity, and enhance visualization.
• Internal defibrillation may be necessary if life-threatening dysrhythmias occur (see Procedure 42).
EQUIPMENT
• Antiseptic solution (e.g., 2% chlorhexidine-based preparation)
• Head cover, masks, eye protection, sterile gown, sterile gloves, sterile drapes
• Sterile open-chest set and sternotomy tray
• Electrocautery equipment: Generator, cautery, electrical dispersing pad (e.g., grounding pad)
• Large sterile suction catheter (e.g., Yankauer)
• Suction containers, tubing, regulator, and suction source
• Radiopaque gauze or other surgical sponge materials
• Polypropylene (Prolene) suture (cutting needle) and other suture material according to preference
• Syringes: 3 ml, 5 ml, 10 ml, and 20 ml
• Knife blades: Nos. 10, 11, 15
• Emergency medication and resuscitation equipment, including internal defibrillation paddles and external defibrillation pads or paddles
Additional equipment as needed includes the following:
• Prescribed analgesia or sedation
• Prescribed blood products and intravenous solutions
• Defibrillator and compatible internal defibrillation paddles
[/not-level-membership-for-critical-care-medicine-category]
