History
An 83-year-old man had undergone implantation of a dual-chamber pacemaker 12 years previously for intermittent high-grade atrioventricular block. He did well for several years, but at age 79 experienced symptoms of congestive heart failure. During the initial hospitalization he was found to have significantly reduced left ventricular systolic function, with a left ventricular ejection fraction (LVEF) of 34%. On echocardiography he had global hypokinesis of the left ventricle. An initial pharmacologic stress study revealed equivocal changes in the inferior wall. Because of the equivocal changes a coronary angiogram was performed. No significant coronary artery disease was found, and the patient was classified as having idiopathic dilated cardiomyopathy. The patient was started on an angiotensin-converting enzyme inhibitor, a beta blocker, a diuretic, and low-dose aspirin. He was already taking a lipid-lowering agent. He had resolution of his heart failure symptoms and was discharged after a 5-day hospital stay. Medications were titrated by his local physician over the following 3 months. The patient did well and returned to an active lifestyle and frequent international travel.
At 81 years of age he again began to experience symptoms, with mild dyspnea on exertion and rare episodes of orthopnea. Medications were altered, and the patient improved and managed as an outpatient. His LVEF was minimally changed, at 32%.
The patient returned 11 months later, at age 82, with profound heart failure symptoms. He was hospitalized again, and his LVEF by echocardiography was 26%. An ambulatory monitor reading was obtained, and the patient was noted to have frequent ventricular extrasystoles, representing 25% of ventricular beats during the 24-hour monitoring period.
The physician managing his care thought the opportunity for further optimization of his medical regimen was minimal. The patient was then referred for consideration of upgrade of his dual-chamber pacemaker to a cardiac resynchronization therapy defibrillator (CRT-D).
At the time of the initial referral evaluation, the patient’s medical regimen appeared optimal. The recent echocardiogram was reviewed and original measurements and observations confirmed. Pacemaker assessment demonstrated pacemaker dependency. He had frequent ventricular extrasystoles on 12-lead electrocardiogram, and frequent extrasystoles were also noted during auscultation. It was explained to the patient that the frequent ventricular extrasystoles could theoretically improve after a device upgrade, especially if improvement in left ventricular function was realized. If the extrasystoles did not improve, he was told that they might require treatment by pharmacologic suppression and/or an ablation procedure if the foci could be identified.
After a thorough discussion of the potential benefits and risks of CRT-D upgrade, the patient was upgraded to a CRT-D device. The chronic ventricular pacing lead was abandoned and capped. The chronic atrial lead was connected to the new CRT-D pulse generator, and a new right ventricular ICD lead and coronary sinus were placed. The defibrillation threshold was 14 J.
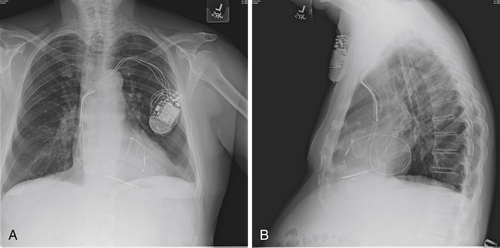
The postimplant chest radiograph is shown in Figure 40-1. Pacing and sensing thresholds checked at the time of discharge were excellent. For the period that the patient was monitored after implant, he continued to have significant ventricular ectopy. He occasionally had pairs and triplets but no longer salvos. The “PVC trigger response” was programmed “on” in an effort to maintain biventricular stimulation. The patient was discharged the day after the CRT-D upgrade and returned a few days later to his home for care to be continued by his cardiologist.
In the months immediately after the procedure the patient thought his peripheral edema was somewhat less noticeable but overall did not feel much improvement. He proceeded with an extended international trip that was intended to last for 5 months at a destination at a considerably higher altitude. Shortly after arrival he developed marked dyspnea on exertion to the point that he returned to his home. On return to the lower altitude his symptoms improved minimally.
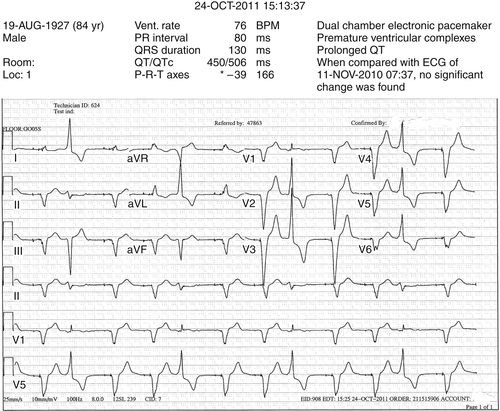
FIGURE 40-1
His local cardiologist added spironolactone to his medical regimen, questioned possible dislodgement of the coronary sinus lead, and referred him for reevaluation of the CRT-D system.
He was reevaluated with chest radiography and echocardiography. On comparison of the postimplant and current radiographs, no significant change in lead positions was appreciated. Pacing and sensing thresholds were excellent. “True” biventricular pacing was noted to be 51%. A 12-lead ambulatory monitor was obtained. Forty percent of his ventricular beats were classified as fusion beats or ventricular extrasystoles. Of the beats classified as premature ventricular contractions, 80% were of the same morphology.
Given the high percentage of ventricular extrasystoles, low percentage of effective biventricular pacing, and, not surprisingly, lack of response to CRT, what options should be considered?
Current Medications
The patient was taking carvedilol 25 mg twice daily, furosemide 20 mg twice daily, lisinopril 20 mg daily, naproxen (Aleve) two tablets (250 mg) as needed, and enteric-coated aspirin 81 mg daily.
Current Symptoms
The patient was easily fatigued. He experienced significant dyspnea on exertion at higher altitudes and mild-to-moderate exertional dyspnea at lower altitudes.
Physical Examination
Laboratory Data
Electrocardiogram
Findings
The electrocardiogram revealed a dual-chamber electronic pacemaker, premature ventricular complexes, and prolonged QT, with no change in contrast to the previous tracing (see Figure 40-1).
Chest Radiograph
Findings
The chest radiograph did not reveal significant changes from the previous radiograph. The implantable cardioverter-defibrillator with right atrial, right ventricular, and coronary sinus leads was visualized (Figure 40-2). The heart size was within normal limits. Pulmonary vascularity was at the upper limits of normal. A tiny amount of scarring was noted in the bases. The chest radiograph was otherwise negative.
Echocardiogram
Findings
The echocardiogram revealed mild-to-moderate left ventricular enlargement, moderate-to-severe decrease in left ventricular systolic function, calculated LVEF of 32%, and generalized left ventricular hypokinesis. Some segmental abnormalities (not depicted graphically) were due to the paced rhythm. Also noted were moderate-to-severe mitral valve regurgitation; moderate tricuspid valve regurgitation resulting, in part, from the device electrode; and moderate-to-severe biatrial enlargement. The findings were consistent with those in moderate pulmonary hypertension. In contrast to the report from November 2010, the rhythm on this echocardiogram was regular, so the quantification of the cardiac magnetic resonance imaging (MRI) is more accurate (see comments in previous report). Visually, however, no significant change was seen in the MRI findings. Tricuspid regurgitation no longer occurred. Side-by-side comparison of images was performed. The right systolic pressure was higher.
Focused Clinical Questions and Discussion Points
Question
Does the premature ventricular contraction morphology matter in terms of CRT nonresponse?
Discussion
The premature ventricular contraction morphology reflects the site of origin for the arrhythmia. For example, in this patient, the left bundle branch block morphology, inferior axis, and positive concordance suggest origin in the basal right ventricular free wall.
Theoretically, premature ventricular contractions that originate in the free wall may be associated with a greater degree of dyssynchrony and thus promote ventricular dysfunction. However, studies suggest that this effect, if present, is minor in contrast to the importance of the overall frequency of the premature ventricular contractions.2
If the device senses an event on the right ventricular lead and if premature ventricular contractions occur from the left ventricular free wall, premature ventricular contraction–triggered pacing possibly could occur after ventricular refractoriness has ended and may be proarrhythmic. It appears, however, that this phenomenon is very rare.
Question
At what number of premature ventricular contractions per day should this arrhythmia be considered a cause for CRT nonresponse?
Discussion
Any premature ventricular contraction will result in inhibition of biventricular pacing. In general, if CRT is not being delivered for more than 95% of the beats, consideration to optimize therapy is recommended. Premature ventricular contractions may contribute to or primarily cause cardiomyopathy and heart failure. Typically more than 20,000 beats per day are from the premature ventricular contractions, and treatment with ablation or medication for the premature ventricular contractions may improve ventricular function.1
A premature ventricular contraction also may produce continued inhibition of pacing beyond a single beat. For example, if the postventricular atrial refractory period has been extended after a premature ventricular contraction, an ensuing sinus beat will not be tracked. Furthermore, if intrinsic conduction is present through the atrioventricular node, native wide QRS conduction would occur. Now this conducted beat acts as another premature ventricular contraction, in turn resulting in the next sinus beat being in the postventricular atrial refractory period (especially if intrinsic conduction through the atrioventricular node is long), and the phenomenon can be repetitive, significantly decreasing effective CRT.3
The device interrogated percentage of biventricular pacing also may be misleading when frequent PVCs occur. Some of the beats may represent the fusion or pseudofusion and be counted as paced beats, but the ventricle is depolarized through the abnormal PVC.
Question
Is it possible to know whether the premature ventricular contractures result from the cardiomyopathy or are causing or contributing to the heart failure process?
Discussion
When cardiomyopathy gives rise to premature ventricular contractions, multiple morphologies could be expected. Monomorphic premature ventricular contractions responsible for the majority of these beats suggest a primary electrical problem that may be giving rise to the cardiomyopathy, and strong consideration should be given to targeting these beats.
At times, considerable doubt may exist as to whether treatment for premature ventricular contraction will improve CRT delivery and the cardiomyopathy itself. Here, when appropriate, a short course of an antiarrhythmic agent, such as amiodarone, can be administered. If the premature ventricular contractions are suppressed and the patient improves significantly, more definitive management such as with radiofrequency ablation for the premature ventricular contraction focus could be considered.
Final Diagnosis
The final diagnosis in this patient was nonresponse to CRT because of inadequate biventricular pacing as a result of frequent ventricular ectopy.
Plan of Action
Options discussed with the patient included an attempt to pharmacologically suppress the ectopy and to attempt ablation of the ectopic foci. The patient wished to avoid another invasive procedure and opted for pharmacologic suppression of the ectopy.
Intervention
The patient was started on amiodarone 200 mg daily and advised to have a repeat ambulatory monitoring examination in 3 to 4 months.
Outcome
An ambulatory monitoring examination was completed by the patient’s local cardiologist approximately 4 months later. The Holter monitor report noted the heart rate to range from 72 to 116 bpm. Ventricular ectopic beats were said to make up 9% of the total heart beats. This is in contrast to the previous ambulatory monitoring, in which 40% of his total heart beats were ventricular ectopic beats. The biventricular pacing had increased to 90%, and the patient had mild-to-moderate subjective improvement in exercise capability and lessening fatigue.
Selected References
1. Bhushan M., Asirvatham S.J. The conundrum of ventricular arrhythmia and cardiomyopathy: which abnormality came first? Curr Heart Fail Rep. 2009;6:7–13.
2. Del Carpio Munoz F., Syed F.F., Noheria A. et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J Cardiovasc Electrophysiol. 2011;22:791–798.
3. Mullens W., Grimm R.A., Verga T. et al. Insights from a cardiac resynchronization optimization clinic as part of a heart failure disease management program. JACC. 2009;53:765–773.



