Procedure 38 Hemivertebrae Resection
Indications
 The primary objective in surgical treatment of hemivertebrae is to prevent the progression to severe spinal deformity.
The primary objective in surgical treatment of hemivertebrae is to prevent the progression to severe spinal deformity.


 Hemivertebrae may lead to a rapidly progressing torsional deformity.
Hemivertebrae may lead to a rapidly progressing torsional deformity.
Examination/Imaging
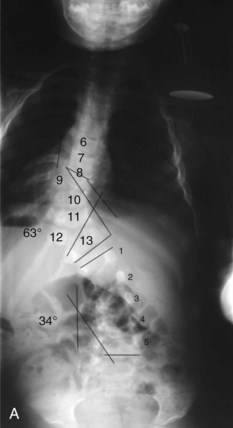
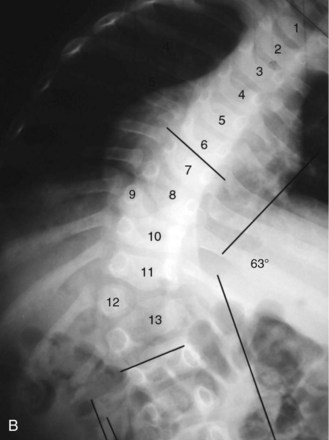
 History and physical (Figure 38-1)
History and physical (Figure 38-1)
 Routine history and physical with special attention to progression of deformity
Routine history and physical with special attention to progression of deformity




Treatment Options
• Combined anterior and posterior fusion



Portals/Exposures
 In thoracic or thoracolumbar approaches, the rib that is one or two levels above the hemivertebrae is removed.
In thoracic or thoracolumbar approaches, the rib that is one or two levels above the hemivertebrae is removed.
 Subperiosteal dissection of posterior elements is performed at the level of the hemivertebrae.
Subperiosteal dissection of posterior elements is performed at the level of the hemivertebrae.
Procedure A: Lateral-Posterior Lumbar Hemivertebra Resection and Correction with Segmental Anterior Instrumentation
Step 1
 The patient is placed in the lateral decubitus position on the concave side.
The patient is placed in the lateral decubitus position on the concave side.
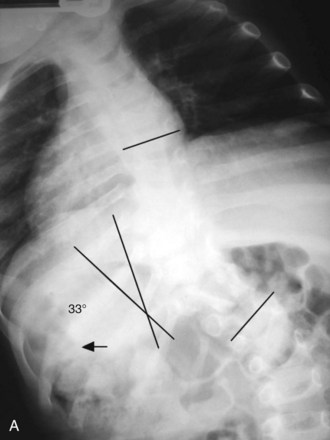
 Make an L-shaped lateral/longitudinal incision 3.5 cm lateral from the spinous processes, above and below the hemivertebrae (Figure 38-4, A).
Make an L-shaped lateral/longitudinal incision 3.5 cm lateral from the spinous processes, above and below the hemivertebrae (Figure 38-4, A).
 The posterior elements of the convexity are exposed subperiosteally.
The posterior elements of the convexity are exposed subperiosteally.

Step 1 Pearls
• Directly excising the hemivertebrae and appended structures will provide immediate correction of the existing deformity.
• Perform intraoperative monitoring of evoked potentials.
• Dissect hemivertebrae from the convex aspect toward the concave.
• Place thrombin-soaked gelatin over the dura if it is exposed.
• The dissected hemivertebrae is cut into morsels and is later used as a graft in filling the cavity created from the resection.



Procedure B: Hemivertebra Resection and Fusion: Anterior and Posterior Approach
Step 1


Step 1 Pearls
• Place thrombin-soaked gelatin over dura if it is exposed.
• A hinge consisting of a small portion of the annulus is preserved on the concave side to avoid lateral translation of the adjacent structures.
• The dissected hemivertebrae is cut into morsels and is later used as a graft in filling the cavity created from the resection.



Procedure C: Posterior Hemivertebra Resection and Correction
Step 1
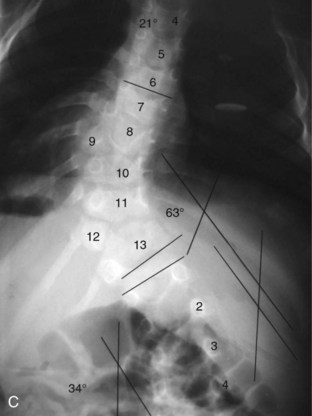
 Make a longitudinal incision along the entire scoliotic curvature (see Figure 38-2, C).
Make a longitudinal incision along the entire scoliotic curvature (see Figure 38-2, C).
 Expose the lateral tip of the transverse processes subperiosteally.
Expose the lateral tip of the transverse processes subperiosteally.
 Resect the spinous process, lamina, and facet of the hemivertebrae.
Resect the spinous process, lamina, and facet of the hemivertebrae.


Step 1 Pearls




Postoperative Care and Expected Outcomes
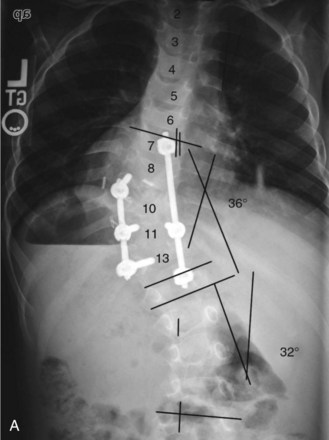
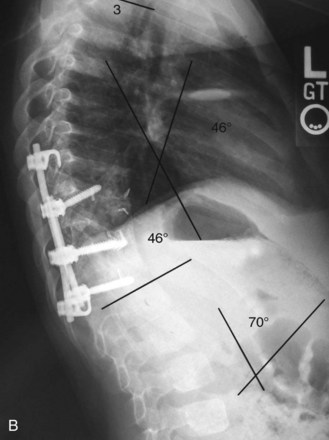
 Standing AP and lateral views of the full spine should be attained postoperatively before hospital discharge, with the patient wearing the brace.
Standing AP and lateral views of the full spine should be attained postoperatively before hospital discharge, with the patient wearing the brace.
Bollini G, Docquier PL, Viehweger E, Launay F, Jouve JL. Lumbar hemivertebra resection. J Bone Joint Surg Am. 2006;88:1043-1052.
Bollini G, Docquier PL, Viehweger E, Launay F, Jouve JL. Thoracolumbar hemivertebrae resection by double approach in a single procedure: long-term follow-up. Spine. 2006;31:1745-1757.
Hedequist DJ, Emans JB. Congenital scoliosis. J Am Acad Orthop Surg. 2004;12:266-275.
Hedequist DJ, Emans JB. The correlation of preoperative three-dimensional computed tomography reconstructions with operative findings in congenital scoliosis. Spine. 2003;28:2531-2534.
Hedequist DJ, Hall JE, Emans JB. Hemivertebra excision in children via simultaneous anterior and posterior exposures. J Pediatr Orthop. 2005;25:60-63.
Lazar RD, Hall JE. Simultaneous anterior and posterior hemivertebra excision. Clin Orthop Relat Res. 1999;364:76-84.
McMaster MJ, Ohtsuka K. The natural history of congenital scoliosis: a study of two hundred and fifty-one patients. J Bone Joint Surg Am. 1982;64:1128-1147.
This study described the natural history of congenital scoliosis in 251 patients.
Nasca RJ, Stilling FHIII, Stell HH. Progression of congenital scoliosis due to hemivertebrae and hemivertebrae with bars. J Bone Joint Surg Am. 1975;57:456-466.
Ruf M, Harms J. Posterior hemivertebra resection with transpedicular instrumentation: early correction in children aged 1 to 6 years. Spine. 2003;28:2132-2138.
Shono Y, Abumi K, Kaneda K. One-stage posterior hemivertebra resection and correction using segmental posterior instrumentation. Spine. 2001;26:752-757.
Solomon BD. VACTERL/VATER Association. Drphanet J Rare Dis. 2011;6:56.


