Procedure 3 Anterior Odontoid Resection
The Transoral Approach

Indications





Examination/Imaging
 Neurologic and musculoskeletal examination
Neurologic and musculoskeletal examination
 Preoperative imaging should include multiplanar radiographs of the cervical spine, computed tomography (CT) with sagittal and coronal reformatting, and magnetic resonance imaging (MRI) to clearly define any soft tissue pathology and the degree of neural compression (Figure 3-1).
Preoperative imaging should include multiplanar radiographs of the cervical spine, computed tomography (CT) with sagittal and coronal reformatting, and magnetic resonance imaging (MRI) to clearly define any soft tissue pathology and the degree of neural compression (Figure 3-1).





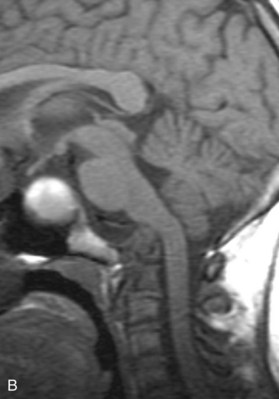
Treatment Options
• Anterior odontoid resection through the transoral approach (transoral-transpharyngeal, with or without palatotomy)
• Combined anterior odontoid resection through the transoral approach, followed by posterior stabilization with possible decompression
• Standalone posterior stabilization with possible decompression
• Adjunctive traction reduction (in setting of reducible basilar invagination or atlantoaxial subluxation), followed by posterior stabilization
Surgical Anatomy
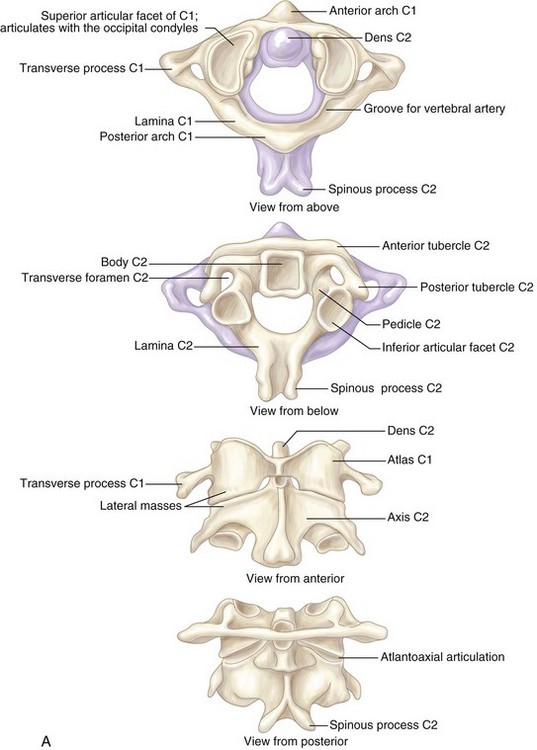
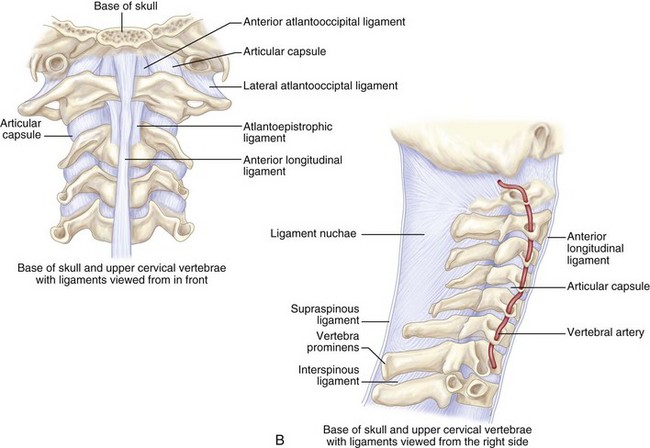
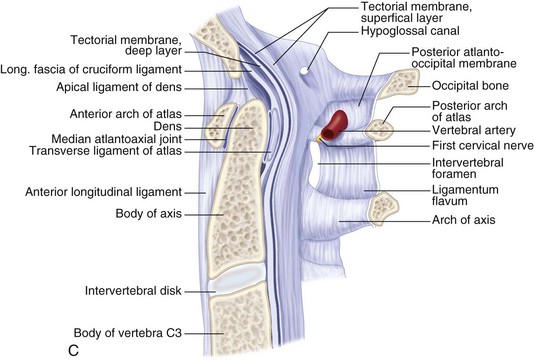
 Understanding the ligaments of the craniovertebral junction is vital when operating in this region.
Understanding the ligaments of the craniovertebral junction is vital when operating in this region.
 The atlas is united to the occipital bone by the anterior and posterior atlanto-occipital membranes.
The atlas is united to the occipital bone by the anterior and posterior atlanto-occipital membranes.



 Below the foramen magnum, the oropharynx is separated from the prevertebral fascia by a well-defined areolar plane (Figure 3-2). The oropharyngeal mucosa heals remarkably well after surgical incision and repair.
Below the foramen magnum, the oropharynx is separated from the prevertebral fascia by a well-defined areolar plane (Figure 3-2). The oropharyngeal mucosa heals remarkably well after surgical incision and repair.

 The anterior longitudinal ligament extends caudally in the midline.
The anterior longitudinal ligament extends caudally in the midline.
Positioning
 Neurophysiologic monitoring electrodes for somatosensory-evoked potential and transcranial motor-evoked potential monitoring are placed first.
Neurophysiologic monitoring electrodes for somatosensory-evoked potential and transcranial motor-evoked potential monitoring are placed first.




Positioning Pearls
• Because many patients have inherent spinal instability, perisurgical neck immobilization may be required. Halo immobilization, however, will limit neck extension and surgical exposure.
• The placement of topical 1% hydrocortisone on the oral mucosa, before and after surgery, may reduce the incidence of lip and tongue swelling.
Positioning Pitfalls
• Inability to widely open the mouth is a relative contraindication to this procedure. As a general rule, in the adult population, if you cannot place three fingers into the mouth of a patient with his or her mouth fully opened, the transoral approach should be avoided. Otherwise, splitting the mandible and tongue may be needed for adequate exposure.
• Alternatively, patients may be positioned laterally in a Mayfield clamp (Figure 3-3). The advantages of this position are that blood and washings drain out of the operative field. The head is placed in slight extension, which improves exposure. The table may be tilted laterally, allowing optimal positioning for the patient and surgeon. After the initial procedure, a posterior stabilization can be performed after reversing the lateral tilt.
• A fluoroscopy unit is then brought in following positioning to confirm adequate positioning and spinal alignment.

Portals/Exposures
 Oral swabs can be obtained for culture to identify bacterial colonization before preparation of the mouth and oropharynx with 1% Betadine or cetrimide.
Oral swabs can be obtained for culture to identify bacterial colonization before preparation of the mouth and oropharynx with 1% Betadine or cetrimide.

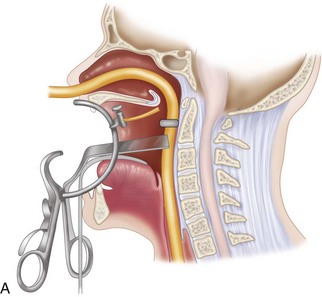
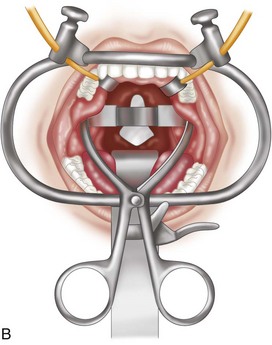
 The midlines of the oropharyngeal mucosa and soft palate are infiltrated with 1% lidocaine with epinephrine (1:100,000). A Crockard transoral retractor system (Codman, Raynham, Mass.) is used to maintain adequate exposure of the posterior oral cavity and to keep the nasotracheal and nasogastric tubes to one side, out of the surgeon’s way (Figures 3-4 and 3-5).
The midlines of the oropharyngeal mucosa and soft palate are infiltrated with 1% lidocaine with epinephrine (1:100,000). A Crockard transoral retractor system (Codman, Raynham, Mass.) is used to maintain adequate exposure of the posterior oral cavity and to keep the nasotracheal and nasogastric tubes to one side, out of the surgeon’s way (Figures 3-4 and 3-5).
 A tongue blade and soft palate retractors maximize the exposure.
A tongue blade and soft palate retractors maximize the exposure.





Procedure
Step 1
 The anterior ridge or tubercle of the atlas is palpated. At this point, a confirmatory lateral localizing image may be taken. An operating microscope can then be used, or a surgeon may choose loupe magnification with directed illumination.
The anterior ridge or tubercle of the atlas is palpated. At this point, a confirmatory lateral localizing image may be taken. An operating microscope can then be used, or a surgeon may choose loupe magnification with directed illumination.
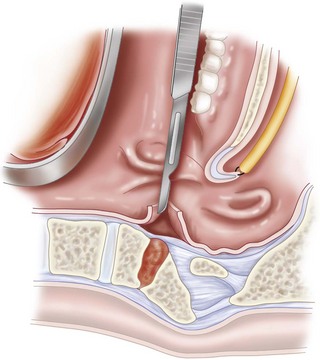
 A vertical incision is made extending approximately 2.5 cm superiorly and 2.5 to 3.0 cm inferiorly along the midline of the posterior oropharynx (Figure 3-6).
A vertical incision is made extending approximately 2.5 cm superiorly and 2.5 to 3.0 cm inferiorly along the midline of the posterior oropharynx (Figure 3-6).






Step 1 Pitfalls
• Great care should be taken to avoid cerebrospinal fluid (CSF) leakage in order to minimize the risk of postoperative meningitis. A preoperative lumbar drain should be placed when an intradural approach is anticipated. In such procedures, fat, muscle, fascia lata, or a dermal fat graft should be used in the repair of any dural opening, followed by the application of fibrin glue.
• With an incision from the inferior clivus to the superior border of C3, an operating field of 15 to 20 mm bilaterally can be exposed. Beyond that, there is an increased risk of trauma to the eustachian tube, hypoglossal nerve, vidian nerve, and vertebral artery at the C1-2 interspace.
• Given the large vascular channels and venous sinusoids in this region, postoperative hematoma formation may be a problem. This can be minimized by meticulous hemostasis, using Avitene, Surgicel, Gelfoam, or fibrin glue, and postoperative nursing in the head-up position. Bleeding from the rheumatoid pannus or small arterial feeders can be controlled with bipolar electrocautery. If an intradural procedure is performed, watertight dural closure is very important to minimize the risk of infection. Suturing or clipping the dura will rarely close the defect completely. A free dermal fat graft, pharyngeal mucosal rotation flaps, or nasal septal mucosal flaps help provide a watertight closure, and a lumbar drain may also be used.
Step 2
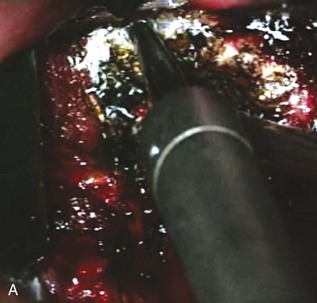
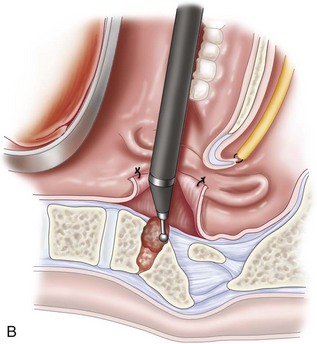
 A match-head burr is used to remove the anterior arch of the atlas out laterally approximately 1 cm to each side of the midline (about two thirds of the arch, exposing the shoulder of the dens bilaterally) (Figure 3-7). The odontoid mass and pannus (if present) are then resected in a rostrocaudal direction (starting at the top of the odontoid process) using a combination of drilling and curetting.
A match-head burr is used to remove the anterior arch of the atlas out laterally approximately 1 cm to each side of the midline (about two thirds of the arch, exposing the shoulder of the dens bilaterally) (Figure 3-7). The odontoid mass and pannus (if present) are then resected in a rostrocaudal direction (starting at the top of the odontoid process) using a combination of drilling and curetting.


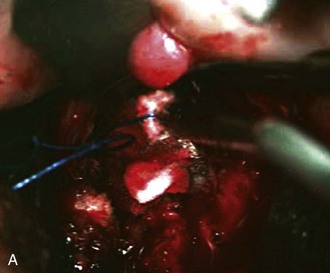
 Any venous bleeding can be controlled with Surgicel and fibrin glue (Figure 3-8, A).
Any venous bleeding can be controlled with Surgicel and fibrin glue (Figure 3-8, A).






Postoperative Care and Expected Outcomes
 Postoperatively, the nasotracheal tube is left in place for 24 to 48 hours. It should only be removed if there is no evidence of significant labial or lingual swelling.
Postoperatively, the nasotracheal tube is left in place for 24 to 48 hours. It should only be removed if there is no evidence of significant labial or lingual swelling.



 Hydrocortisone ointment should be applied to the tongue and mucosa for the first 48 hours.
Hydrocortisone ointment should be applied to the tongue and mucosa for the first 48 hours.
 In the event of a durotomy, lumbar drainage should be maintained for 5 to 10 days. Prophylactic antibiotic therapy directed against gram-positive, gram-negative, and anaerobic oral flora may be administered by some surgeons. For example, Menezes (1991) recommended CSF cultures for the initial 5 days, at which point, if the cultures remain negative, antibiotics may be stopped. Occasionally, a lumbar-peritoneal shunt may be required for persistent CSF leakage.
In the event of a durotomy, lumbar drainage should be maintained for 5 to 10 days. Prophylactic antibiotic therapy directed against gram-positive, gram-negative, and anaerobic oral flora may be administered by some surgeons. For example, Menezes (1991) recommended CSF cultures for the initial 5 days, at which point, if the cultures remain negative, antibiotics may be stopped. Occasionally, a lumbar-peritoneal shunt may be required for persistent CSF leakage.

Complications
• Airway complications are always a concern with the transoral approach. It is the practice of the senior author to leave the endotracheal tube in place for a minimum of 24 hours following surgery. If after this time there is evidence of swelling of the tongue or oral cavity, the endotracheal tube is left in situ until the swelling subsides. The occurrence of lingual swelling may be minimized by intermittent intraoperative release of the retractor, and ensuring the tongue is not trapped between the retractor blade and the lower teeth.
• Delayed complications may include tongue swelling, meningitis, palatal/pharyngeal dehiscence, neurologic deterioration, retropharyngeal abscess, late pharyngeal bleeding, and velopalatine incompetence. Pharyngeal dehiscence may occur either early or late. Early dehiscence (during the first 7 days after surgery) is typically due to inadequate closure or starting oral feeding too early. This can be minimized by encouraging the patient to sit up and walk as soon as possible to prevent pooling of saliva at the apex or weakest point of the pharyngeal incision. If early dehiscence occurs, closure should be attempted (with the assistance of head and neck specialists if required), followed by hyperalimentation and intravenous antibiotics. In cases of late dehiscence, infection needs to be ruled out. The differential diagnosis of late dehiscence includes osteomyelitis, retropharyngeal abscess, and poor nutrition. Management of retropharyngeal abscess includes lateral drainage (rather than transoral), followed by appropriate intravenous antibiotics, hyperalimentation through a nasogastric feeding tube, and neck immobilization.
• Neurologic deterioration after transoral odontoid resection is most likely to be due to craniocervical instability. The vast majority of patients who undergo this procedure require a posterior stabilization procedure.
• In patients with altered mental status following the transoral approach, meningitis must be kept at the forefront of the differential diagnosis. This is particularly true in the elderly population with rheumatoid arthritis, in whom this diagnosis may be overlooked because confusion in this age group can be common in the critical care setting.
• Late retropharyngeal bleeding may indicate an underlying infection. Osteomyelitis and pseudoaneurysm of the vertebral artery must also be ruled out. MRI/MRA evaluation of the craniovertebral junction should be performed in addition to angiography to rule out vascular involvement. This diagnostic process also allows for potential therapeutic endovascular treatment in cases of vertebral artery compromise.
• Velopalatine incompetence (incorrect closure of the soft palate muscle during speech resulting in a nasal voice) occurs more commonly in children than in adults. It typically occurs 4 to 6 months after the transoral procedure and probably occurs secondary to contracture of the soft palate and nasopharynx. This requires otorhinolaryngologic evaluation. Usually it is treated with pharyngeal retraining, but a palatal prosthesis or a pharyngeal flap may also be used.
Apuzzo ML, Weiss MH, Heiden JS. Transoral exposure of the atlantoaxial region. Neurosurgery. 1978;3:201-207.
Crockard HA. Transoral surgery: some lessons learned. Br J Neurosurg. 1995;9:283-293.
Crockard HA, Calder I, Ransford AO. One-stage transoral decompression and posterior fixation in rheumatoid atlanto-axial subluxation. J Bone Joint Surg Br. 1990;72:682-685.
Crockard HA, Sen CN. The transoral approach for the management of intradural lesions at the craniovertebral junction: review of 7 cases. Neurosurgery. 1991;28:88-97. discussion 97-8
Fang HSY, Ong GB. Direct anterior approach to the upper cervical spine. J Bone Joint Surg Am. 1962;44:1588-1604.
Frempong-Boadu AK, Faunce WA, Fessler RG. Endoscopically assisted transoral-transpharyngeal approach to the craniovertebral junction. Neurosurgery. 2002;51(5 Suppl):S60-S66.
A review of the endoscopic transoral approach (Level IV evidence [case series of 7 patients]).
Hadley MN, Martin NA, Spetzler RF, Sonntag VK, Johnson PC. Comparative transoral dural closure techniques: a canine model. Neurosurgery. 1988;22:392-397.
Hsu W, Wolinsky J, Gokaslan Z, Sciubba DM. Transoral approaches to the cervical spine. Neurosurgery. 2010;66(Suppl. 3):119-125.
Kaibara T, Hurlbert RJ, Sutherland GR. Transoral resection of axial lesions augmented by intraoperative magnetic resonance imaging: report of three cases. J Neurosurg Spine. 2001;95:239-242.
Krauss WE, Bledsoe JM, Clarke MJ, Nottmeier EW, Pichelmann MA. Rheumatoid arthritis of the craniovertebral junction. Neurosurgery. 2010;66(Suppl. 3):83-95.
Menezes AH. Complications of surgery at the craniovertebral junction—avoidance and management. Pediatr Neurosurg. 1991;17:254-266.
Pollack IF, Welch W, Jacobs GB, Janecka IP. Frameless stereotactic guidance: an intraoperative adjunct in the transoral approach for ventral cervicomedullary junction decompression. Spine. 1995;20:216-220.
Singh H, Harrop J, Schiffmacher P, Rosen M, Evans J. Ventral surgical approaches to craniovertebral junction chordomas. Neurosurgery. 2010;66(Suppl. 3):96-103.
Youssef AS, Sloan AE. Extended transoral approaches: surgical technique and analysis. Neurosurgery. 2010;66(Suppl. 3)):126-134.


