[level-membership-for-cardiovascular-category]
History
Comments
Current Medications
Comments
Current Symptoms
Comments
Physical Examination
Comments
Laboratory Data
Electrocardiogram
Findings
Comments
Echocardiogram
Findings
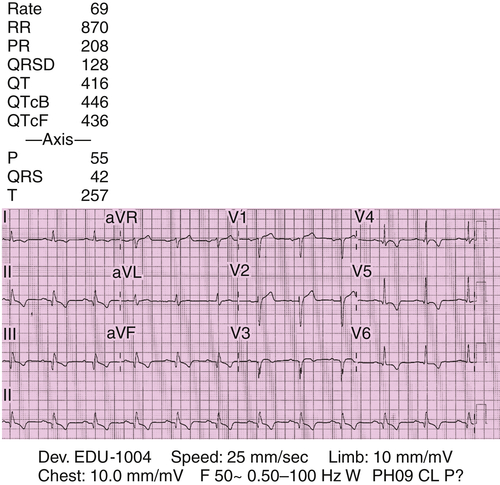
FIGURE 22-1
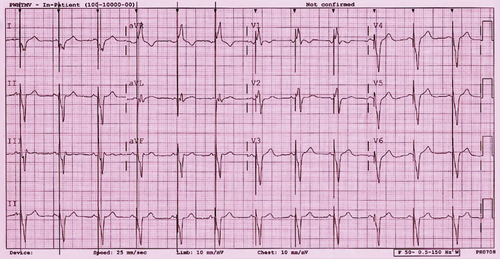
FIGURE 22-2
Comments
Findings
Comments
Findings
Comments
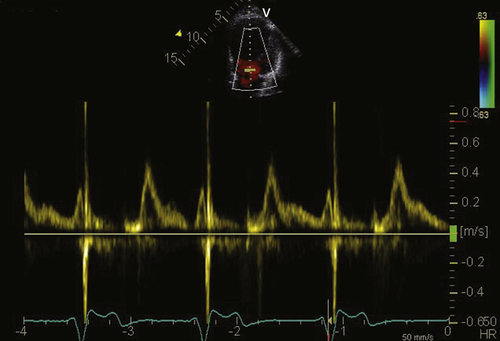
FIGURE 22-3
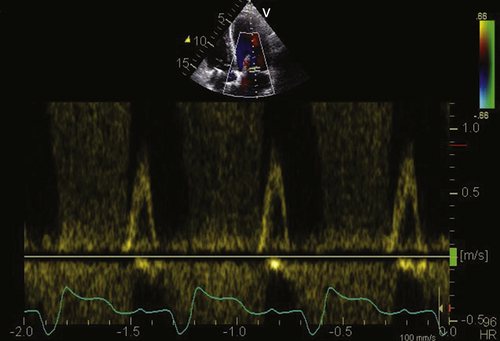
FIGURE 22-4
Findings
Comments
Focused Clinical Questions and Discussion Points
Question
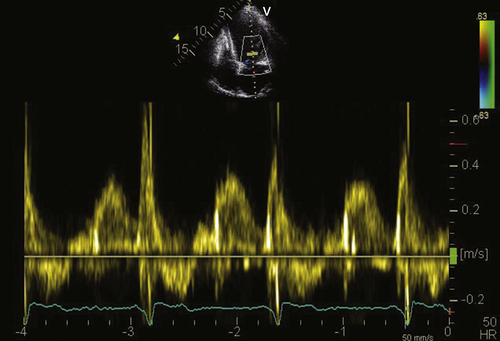
FIGURE 22-5
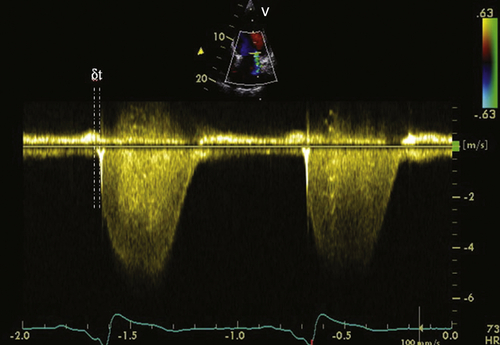
FIGURE 22-6
Discussion
Question
Discussion
Ritter Method
Mitral Regurgitation Method
The Iterative Method
Discussion
Final Diagnosis
Plan of Action
Intervention
Selected References
1. Cleland J.G., Daubert J.C., Erdmann E. et al. The CARE-HF study (CArdiac REsynchronisation in Heart Failure study): rationale, design and end-points. Eur J Heart Fail.. 2001;3:481–489.
2. Heydari B., Jerosch-Herold M., Kwong R.Y. et al. Imaging for planning of cardiac resynchronization therapy. JACC Cardiovasc Imaging. 2012;5:93–110.
3. Gorcsan 3rd. J., Abraham T., Agler D.A. et al. Echocardiography for cardiac resynchronization therapy: recommendations for performance and reporting. Report from the American Society of Echocardiography Dyssynchrony Writing Group endorsed by the Heart Rhythm Society. J Am Soc Echocardiogr. 2008;21:191–213.
4. Ritter P., Dib J.C., Lelievre T. et al. Quick determination of the optimal AV delay at rest in patients paced in DDD mode for complete AV block. (abstract). Eur J CPE. 1994;4:A163.
5. Meluzín J., Spinarová L., Bakala J. et al. Pulsed Doppler tissue imaging of the velocity of tricuspid annular systolic motion: a new, rapid, and non-invasive method of evaluating right ventricular systolic function. Eur Heart J. 2001;22:340–348.
6. Zhang Q., Fung J.W., Chan Y.S. et al. The role of repeating optimization of atrioventricular interval during interim and long-term follow-up after cardiac resynchronization therapy. Int J Cardiol. 2008;124:211–217.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
History
Comments
Current Medications
Comments
Current Symptoms
Comments
Physical Examination
Comments
Laboratory Data
Electrocardiogram
Findings
Comments
Echocardiogram
Findings
FIGURE 22-1
FIGURE 22-2
[/not-level-membership-for-cardiovascular-category]
