[level-membership-for-cardiovascular-category]
History
In 2010 the patient reported dyspnea with New York Heart Association (NYHA) class II, then class III. A nonischemic dilated cardiomyopathy was diagnosed. The surface electrocardiogram (ECG) showed a complete left bundle branch block (LBBB) and the echocardiography a left ventricular ejection fraction (LVEF) of 25% and a left ventricular end-diastolic diameter of 63 mm. A medical treatment including angiotensin-converting enzyme inhibitors, beta blockers, and diuretics was prescribed with a significant improvement in symptoms and echocardiographic parameters over 1 year. A NYHA class II to III dyspnea occurred in 2012, as well as a deterioration in LVEF (25%). The implantation of a cardiac resynchronization therapy defibrillator (CRT-D) was attempted in another center, but the left ventricular lead could not be implanted because of a coronary sinus dissection. A CRT-D device was implanted, with a plug into the left ventricular port. The patient was referred to our center 2 months later for a new attempt of left ventricular lead implantation. Computed tomography (CT) was performed to assess the patency of the coronary sinus. A Medtronic 4194 (Minneapolis, Minn.) left ventricular lead was implanted into a lateral vein. The lead must be positioned at the proximal part of the lateral vein because of a permanent phrenic nerve simulation at the distal and medial part of the vein despite the electrical repositioning. The following day the chest radiograph showed the dislodgement of the left ventricle lead into the body of the coronary sinus.
Current Medications
The patient was taking bisoprolol 10 mg daily, ramipril 10 mg daily, eplerenone 50 mg daily, and furosemide 40 mg daily.
Comments
The patient was on optimal drug treatment according to the new European Society of Cardiology 2012 guidelines.
Current Symptoms
The patient was experiencing dyspnea with NYHA class III and no signs of right heart failure.
Physical Examination
Comments
The patient had symptoms of left heart failure but no signs of heart failure decompensation.
Laboratory Data
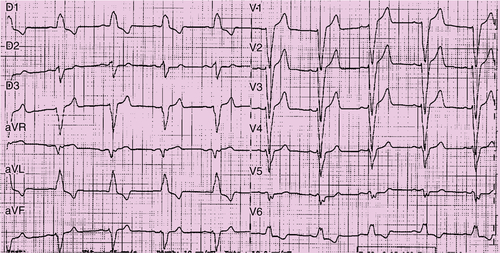
FIGURE 23-1 Baseline electrocardiogram with sinus rhythm and left bundle branch block.
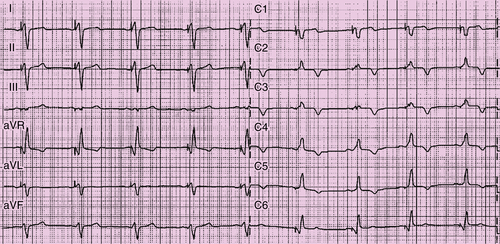
FIGURE 23-2 Surface electrocardiogram with biventricular pacing, with the bipolar lead positioned at the proximal portion of the lateral vein (see Figure 23-1).
Comments
The N-terminal pro-brain natriuretic peptide was 450 pg/mL.
Electrocardiogram
Findings
The electrocardiogram revealed sinus rhythm and complete LBBB (
Figure 23-1), biventricular pacing with the bipolar lead (Figure 23-2), and biventricular pacing with final quadripolar lead (Figure 23-3).
Chest Radiograph
Findings
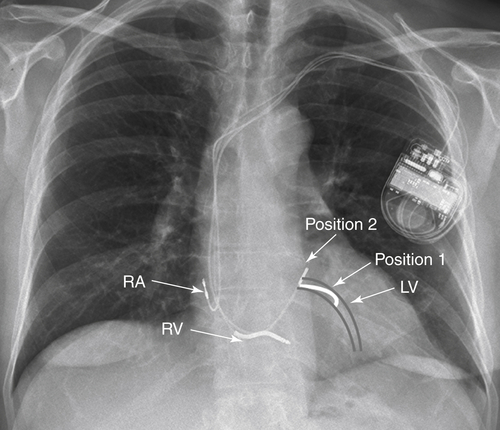
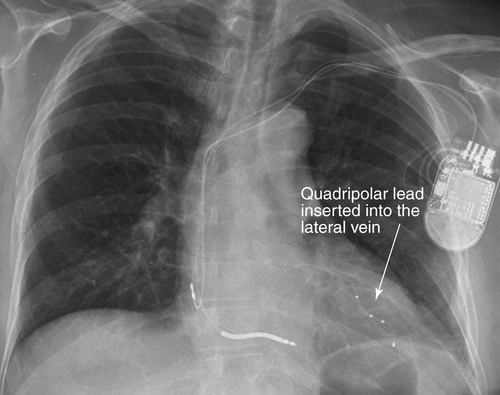
Figure 23-4 shows dislodgement of the Attain 4194 left ventricular lead (Medtronic) into the body of the cornonary sinus (arrow 2). Arrow 1 shows the initial location of the tip of the left ventricular lead in the operating room. Figure 23-5 shows the left ventricular lead with four poles positioned into the lateral vein.
Comments
Dislodgement lead can be seen in
Figure 23-4. A quartet lead (St. Jude Medical) can be seen in the lateral vein in
Figure 23-5.
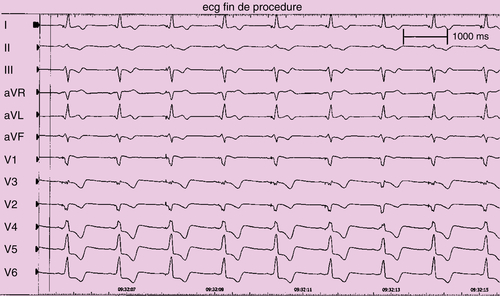
FIGURE 23-3 Final surface electrocardiogram with biventricular pacing with left ventricular pacing configuration M4 (proximal pole) to right ventricular coil.
FIGURE 23-4 Left ventricular (LV) projection of the lateral vein. Position 1: Position of the LV lead at the end of the implantation. Position 2: Position of the LV lead the day after into the body of the coronary sinus. RA, Right atrial; RV, right ventricular.
Focused Clinical Questions and Discussion Points
Question
What should be done if a complete coronary sinus dissection occurred during the implantation of a left ventricular lead into the coronary sinus?
Discussion
The recommendation is to stop the left ventricular lead implantation and monitor the patient in the intensive care unit with repeated echocardiographic examinations to diagnose a potential pericardial effusion or tamponade.
Question
Is the coronary sinus dissection definitive?
Discussion
In clinical follow-up, after 1 month, the coronary sinus was patent without dissection.
Question
How should one deal with phrenic nerve stimulation?
Final Diagnosis
In this patient the final diagnosis was left ventricular lead dislodgement related to the need for positioning the bipolar left ventricular lead at the entry of the coronary sinus lateral vein.
Plan of Action
A repeat operation was peformed. The bipolar left ventricular lead was removed and a new quadripolar left ventricular lead (Quartet, St. Jude Medical) implanted.
Intervention
The quadripolar left ventricular lead was inserted more distally in the same vein. Pacing at the distal pole and pole 2 enhanced PNS in all of the pacing configurations. Only pacing with pole 3 and 4 in pseudo-bipolar mode with the right ventricular lead provided an acceptable pacing threshold without PNS.
Outcome
After 4 months of follow-up the left ventricular pacing theshold is stable at approximately 1.3 V without PNS (see
Figures 23-3 and
23-6), with permanent biventricular capture and improvement in symptoms and exercise capacity.
Selected References
1. Forleo G.B., Della Rocca D.G., Papavasileiou L.P. et al. Left ventricular pacing with a new quadripolar transvenous lead for CRT: early results of a prospective comparison with conventional implant outcomes. Heart Rhythm. 2011;8:31–37.
2. Landolina M., Gasparini M., Lunati M. et al. Long-term complications related to biventricular defibrillator implantation: rate of surgical revisions and impact on survival: insights from the Italian Clinical Service Database. Circulation. 2011;123:2526–2535.
3. Thibault B. et al. Posters PO 04-117 to 04-183. Heart Rhythm. 2011;8 S291.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
History
In 2010 the patient reported dyspnea with New York Heart Association (NYHA) class II, then class III. A nonischemic dilated cardiomyopathy was diagnosed. The surface electrocardiogram (ECG) showed a complete left bundle branch block (LBBB) and the echocardiography a left ventricular ejection fraction (LVEF) of 25% and a left ventricular end-diastolic diameter of 63 mm. A medical treatment including angiotensin-converting enzyme inhibitors, beta blockers, and diuretics was prescribed with a significant improvement in symptoms and echocardiographic parameters over 1 year. A NYHA class II to III dyspnea occurred in 2012, as well as a deterioration in LVEF (25%). The implantation of a cardiac resynchronization therapy defibrillator (CRT-D) was attempted in another center, but the left ventricular lead could not be implanted because of a coronary sinus dissection. A CRT-D device was implanted, with a plug into the left ventricular port. The patient was referred to our center 2 months later for a new attempt of left ventricular lead implantation. Computed tomography (CT) was performed to assess the patency of the coronary sinus. A Medtronic 4194 (Minneapolis, Minn.) left ventricular lead was implanted into a lateral vein. The lead must be positioned at the proximal part of the lateral vein because of a permanent phrenic nerve simulation at the distal and medial part of the vein despite the electrical repositioning. The following day the chest radiograph showed the dislodgement of the left ventricle lead into the body of the coronary sinus.
Current Medications
The patient was taking bisoprolol 10 mg daily, ramipril 10 mg daily, eplerenone 50 mg daily, and furosemide 40 mg daily.
Comments
The patient was on optimal drug treatment according to the new European Society of Cardiology 2012 guidelines.
Current Symptoms
The patient was experiencing dyspnea with NYHA class III and no signs of right heart failure.
Physical Examination
Comments
The patient had symptoms of left heart failure but no signs of heart failure decompensation.
Laboratory Data
Buy Membership for Cardiovascular Category to continue reading.
Learn more here
[/not-level-membership-for-cardiovascular-category]
Cases in Cardiac Resynchronization Therapy Expert Consult