Procedure 18 Operative Management of Scheuermann Kyphosis

Indications
 Rigid curves greater than 75 degrees
Rigid curves greater than 75 degrees
 Curves that have progressed despite brace treatment
Curves that have progressed despite brace treatment
 Painful kyphotic curves that progress despite nonoperative treatment
Painful kyphotic curves that progress despite nonoperative treatment

 Respiratory difficulty resulting from curves greater than 100 degrees
Respiratory difficulty resulting from curves greater than 100 degrees
Examination/Imaging



Surgical Anatomy





Positioning



Procedure
Step 1: Anterior Release and Fusion
 Perform an open or video-assisted thoracoscopic approach.
Perform an open or video-assisted thoracoscopic approach.
 Disks that do not become lordotic on hyperextension radiographs should be resected.
Disks that do not become lordotic on hyperextension radiographs should be resected.
 A strut graft can be placed to enhance fusion and prevent loss of correction.
A strut graft can be placed to enhance fusion and prevent loss of correction.

Step 1 Pearls
• Resecting the anterior portion of the rib head allows more exposure of the posterior disk.
• A laminar spreader can be used to view the remaining disk after the initial diskectomy.
• It is critical to release the anterior longitudinal ligament, because this is part of the deforming force.
• Chest tubes are discontinued when drain output is less than 80 mL per 8-hour shift.
Step 1 Controversies
• A thoracic surgeon may be required for anterior approaches.
• A vertebral column resection (VCR) or pedicle subtraction osteotomy (PSO) in posterior-only fusion may lead to correction equal to that of anterior release and posterior fusion.
• Performing a VCR or PSO at cord level potentially carries a higher risk of neurologic complications, especially in older patients.
• Combined procedures have a higher incidence of general complications than posterior-only surgery.
• VATS has been found to result in less morbidity than conventional thoracotomy, but it is approximately 30% more expensive.
Postoperative Care and Expected Outcomes
 Bracing is typically not necessary.
Bracing is typically not necessary.
 Patients are maintained in the intensive care unit or a monitored bed overnight.
Patients are maintained in the intensive care unit or a monitored bed overnight.

Step 2
 Perform a wide release, including a radical facetectomy at the apex and at the three adjacent cranial and caudal levels.
Perform a wide release, including a radical facetectomy at the apex and at the three adjacent cranial and caudal levels.

 A rod should be contoured to normal sagittal alignment.
A rod should be contoured to normal sagittal alignment.
 The rod is inserted into the proximal screws (Figure 18-2, A) and cantilevered into the remaining screws (Figure 18-2, B).
The rod is inserted into the proximal screws (Figure 18-2, A) and cantilevered into the remaining screws (Figure 18-2, B).

 If a PSO or VCR is performed, a temporary fixation rod is required for any correction maneuvers.
If a PSO or VCR is performed, a temporary fixation rod is required for any correction maneuvers.

Step 2 Pearls
• The distal end of the instrumentation should be the sagittal stable vertebra, which is the most proximal thoracolumbar or lumbar vertebra intersected (not bisected) by the posterior sacral vertical line.
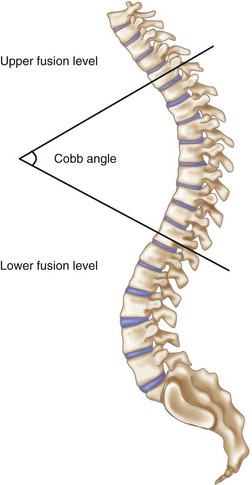
• The proximal end of the instrumentation should be the proximal vertebra measured in the Cobb angle (Figure 18-1).
Step 2 Pitfalls
• If an apical disk herniation is seen on the MRI, an anterior diskectomy or VCR should be performed before curve correction.
• A thoracic VCR requires resection of the rib head and often sacrifices the nerve root.
• The mean arterial pressure should be increased to at least 75 mm Hg before correction.
 -inch stainless steel) will prevent loss of correction.
-inch stainless steel) will prevent loss of correction.Arlet V, Schlenzka D. Scheuermann’s kyphosis: surgical management. Eur Spine J. 2005;14:817-827.
Boachie-Adjei O, Sarwahi V. Scheuermann’s kyphosis. In: DeWald RL, editor. Spinal Deformities: The Comprehensive Text. New York: Thieme Medical Publishers; 2003:777-786.
Lee SS, Lenke LG, Kuklo TR, et al. Comparison of Scheuermann kyphosis correction by posterior-only thoracic pedicle screw fixation versus combined anterior/posterior fixation. Spine. 2006;31:2316-2321.
Murray PM, Weinstein SL, Spratt KF. The natural history and long-term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am. 1993;75:236-248.

