Procedure 15 Posterior Cervical Laminoplasty
Indications
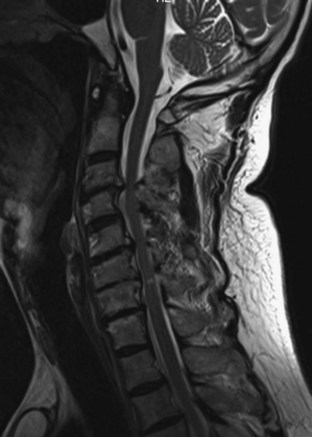
 Multilevel cervical spondylotic myelopathy in three or more motion segments (Figure 15-1)
Multilevel cervical spondylotic myelopathy in three or more motion segments (Figure 15-1)
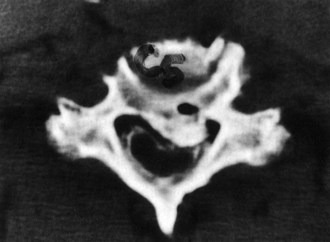
 Ossification of the posterior longitudinal ligament (OPLL) (Figure 15-2)
Ossification of the posterior longitudinal ligament (OPLL) (Figure 15-2)


Examination/Imaging
 Upper motor neuron signs (Hoffmann, clonus, up-going Babinski reflex, and finger escape sign)
Upper motor neuron signs (Hoffmann, clonus, up-going Babinski reflex, and finger escape sign)

 Difficulties with any activities requiring fine motor movements (buttoning shirt, writing)
Difficulties with any activities requiring fine motor movements (buttoning shirt, writing)
 Wasting of hand intrinsic musculature
Wasting of hand intrinsic musculature


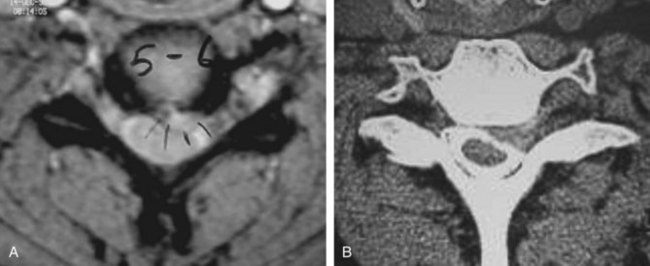
 Figure 15-5 shows axial MRI (A) and CT (B) myelogram demonstrating left-sided compression. The choice of opening side depends on the side of neurologic compression. In this example, the opening side would be the left side.
Figure 15-5 shows axial MRI (A) and CT (B) myelogram demonstrating left-sided compression. The choice of opening side depends on the side of neurologic compression. In this example, the opening side would be the left side.
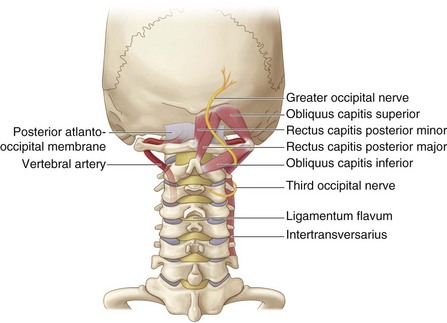
Surgical Anatomy


Positioning
 The patient’s hair is shaved up to the inferior margin of the occiput.
The patient’s hair is shaved up to the inferior margin of the occiput.

 The head is positioned with the “chin-tucked and slightly forward-flexed” to facilitate exposure.
The head is positioned with the “chin-tucked and slightly forward-flexed” to facilitate exposure.
 Operating room bed positioning
Operating room bed positioning
 After the patient is positioned, the shoulders are taped down.
After the patient is positioned, the shoulders are taped down.


Portals/Exposures
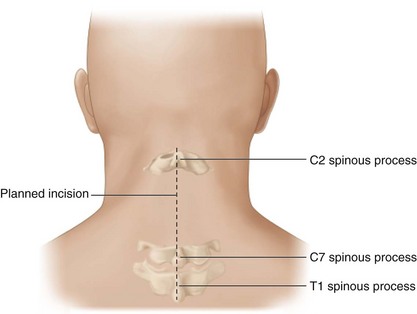
 The spinous processes of C2 and C7serve as superficial landmarks for the surgical incision.
The spinous processes of C2 and C7serve as superficial landmarks for the surgical incision.
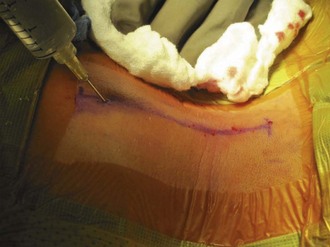
 Injection of local anesthetic with epinephrine into the paraspinal musculature minimizes bleeding (Figure 15-9).
Injection of local anesthetic with epinephrine into the paraspinal musculature minimizes bleeding (Figure 15-9).
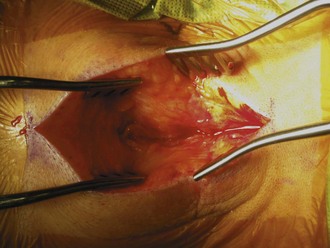
 Follow the nuchal line to the spinous processes (Figure 15-10). A careful midline dissection through the nuchal ligament minimizes muscular bleeding.
Follow the nuchal line to the spinous processes (Figure 15-10). A careful midline dissection through the nuchal ligament minimizes muscular bleeding.
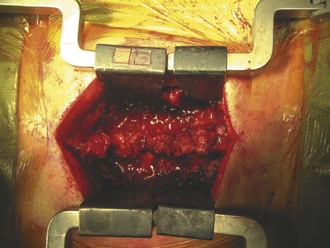
 Use standard exposure to the cervical spine from C2 to T1 (Figure 15-11).
Use standard exposure to the cervical spine from C2 to T1 (Figure 15-11).


Procedure
 The authors will describe a modified “open-door laminoplasty” technique originally described by Hirabayashi and colleagues. The technique entails variations on laminoplasty types: They can be generally described as unilateral hinge (“open-door”) and bilateral hinge (“French door”) with supplemental procedures. Various supplemental methods are used to keep the laminoplasty door open (laminoplasty plates, suture use, and bone graft).
The authors will describe a modified “open-door laminoplasty” technique originally described by Hirabayashi and colleagues. The technique entails variations on laminoplasty types: They can be generally described as unilateral hinge (“open-door”) and bilateral hinge (“French door”) with supplemental procedures. Various supplemental methods are used to keep the laminoplasty door open (laminoplasty plates, suture use, and bone graft).
Step 1
 C3-7 spinous processes are removed to facilitate exposure and if spinous process sutures are not used.
C3-7 spinous processes are removed to facilitate exposure and if spinous process sutures are not used.
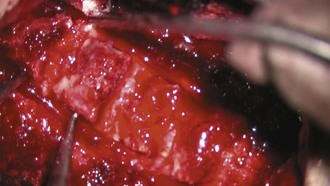
 A high-speed AM-8 burr (Midas Rex Pneumatic Tools, Fort Worth, Texas) is used to make two bony troughs at the medial aspect of the lateral mass or the lamina–facet junction (Figure 15-12).
A high-speed AM-8 burr (Midas Rex Pneumatic Tools, Fort Worth, Texas) is used to make two bony troughs at the medial aspect of the lateral mass or the lamina–facet junction (Figure 15-12).
 The lamina is thicker at the superior margin and thinner inferiorly.
The lamina is thicker at the superior margin and thinner inferiorly.

 The opening side is removed with a burr bicortically (cortical-cancellous-cortical bone layer).
The opening side is removed with a burr bicortically (cortical-cancellous-cortical bone layer).
Step 2
 Ligamentum flavum from the C2-3 interspace and C7-T1 interspace is excised with a Kerrison rongeur (Figure 15-13, A and B). Ligamentum flavum is excised at both interlaminar spaces at the cephalad and caudad levels of the laminoplasty.
Ligamentum flavum from the C2-3 interspace and C7-T1 interspace is excised with a Kerrison rongeur (Figure 15-13, A and B). Ligamentum flavum is excised at both interlaminar spaces at the cephalad and caudad levels of the laminoplasty.
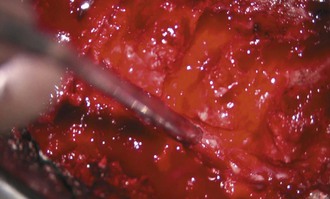
 Any dural adhesions on the opening side are freed with curettes and 2-mm Kerrison rongeurs (Figure 15-14).
Any dural adhesions on the opening side are freed with curettes and 2-mm Kerrison rongeurs (Figure 15-14).


Step 3
 The hinge side is carefully opened by the operative assistant, using small forward-angled curettes or skin hooks.
The hinge side is carefully opened by the operative assistant, using small forward-angled curettes or skin hooks.

Step 3 Pearls
• Be careful not to be overly aggressive. A 6- to 8-mm opening achieves good decompression with less risk of posterior migration of spinal cord and root tension.
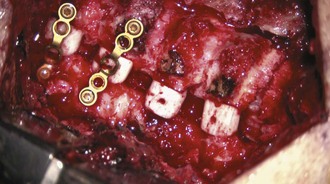
• Allograft trial spacers (Figure 15-15) are used to estimate graft size.
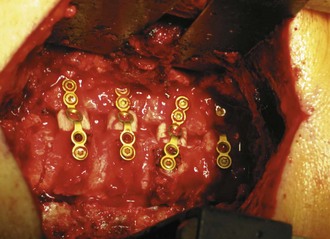
• Allograft spacers are applied on the opening side (Figure 15-16).






Postoperative Care and Expected Outcomes



Herkowitz HN. A comparison of anterior cervical fusion, cervical laminectomy, and cervical laminoplasty for the surgical management of multiple level spondylotic radiculopathy. Spine. 1988;13:774-780.
Hirabayashi K, Watanabe K, Wakano K, et al. Expansive open-door laminoplasty for cervical spinal stenotic myelopathy. Spine. 1983;8:693-699.
Park AE, Heller JG. Cervical laminoplasty: use of a novel titanium plate to maintain canal expansion–surgical technique. J Spinal Disord Tech. 2004;17:265-271.
Satomi K, Ogawa J, Ishii Y, Hirabayashi K. Short-term complications and long-term results of expansive open-door laminoplasty for cervical stenotic myelopathy. Spine J. 2001;1:26-30.

