History
Current Medications
Current Symptoms
Physical Examination
Laboratory Data
Comments
Electrocardiogram
Findings
Chest Radiograph
Findings

FIGURE 15-1 Posterior-anterior fluoroscopic view showing the guide wire in serted via left axillary vein puncture, tracking into the persistent left superior vena cava. Contrast injection did not show an innominate vein or posterior lateral tributaries suitable for coronary sinus lead implantation.
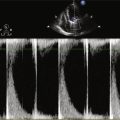
Echocardiogram
Findings
Final Diagnosis
Intervention

FIGURE 15-2 Levophase of the left coronary angiogram in the right anterior oblique 30-degree projection showing a dilated coronary sinus (the persistent left superior vena cava is also visible) and a posterior lateral vein.
Outcome
Comments
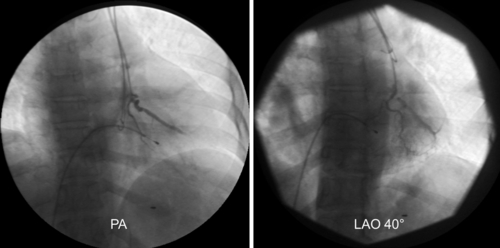
FIGURE 15-3 Subselection of the lateral vein with a Judkins right 4 diagnostic catheter in the posterior-anterior (left) and left anterior oblique 40-degree (right) views.
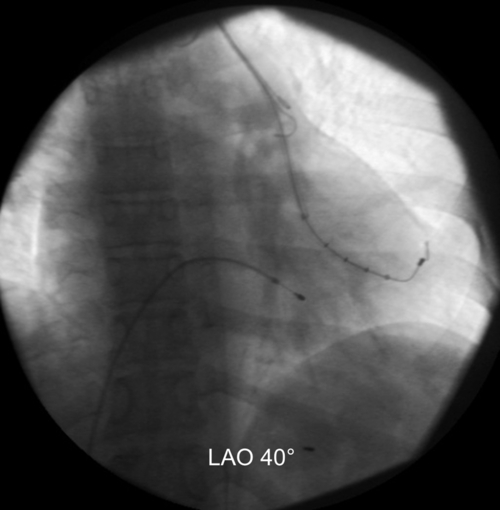
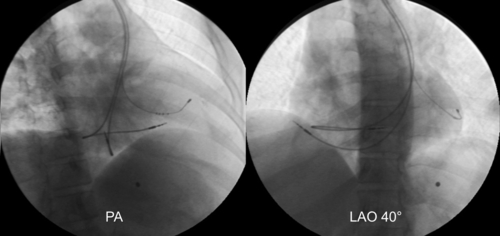
FIGURE 15-4 Positioning of the left ventricular lead in the lateral branch.
Selected References
1. Ratliff H.L., Yousufuddin M., Lieving W.R. et al. Persistent left superior vena cava: case reports and clinical implications. Int J Cardiol. 2006;113:242–246.
2. Gasparini M., Mantica M., Galimberti P. et al. Biventricular pacing via a persistent left superior vena cava: report of four cases. Pacing Clin Electrophysiol. 2003;26:192–196.