History
Intervention
Outcome
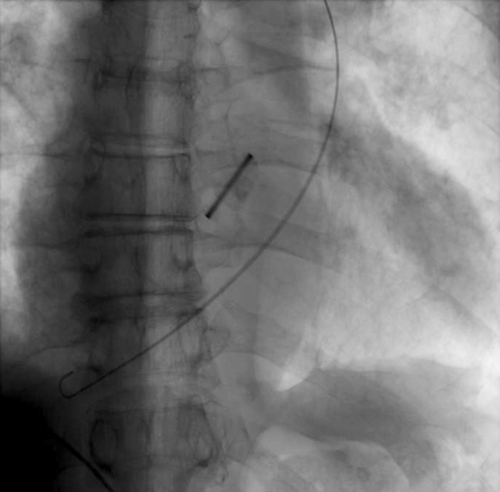
FIGURE 14-1 Posteroanterior view of a left-sided venous access with the J-wire tracking down the PLSVC into the coronary sinus and right atrium.
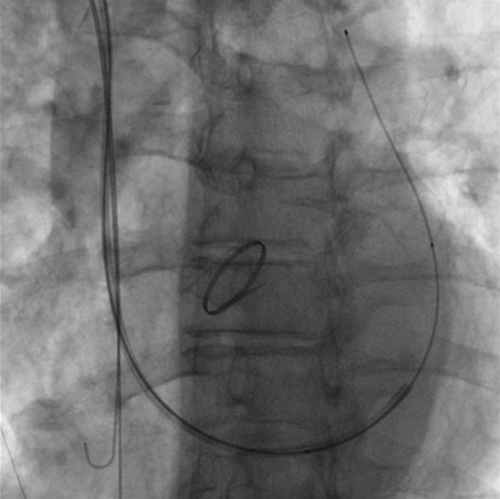
FIGURE 14-2 Posteroanterior fluoroscopic view after right-sided venous access and retrograde cannulation of the coronary sinus with a guiding catheter and 0.035-inch guide wire. Note that the guide wire may be mistaken to be in the pulmonary artery in this view (the cranial excursion of the guide wire and a left anterior oblique view showing a posterior course of the guide wire allow the operator to make the correct diagnosis).
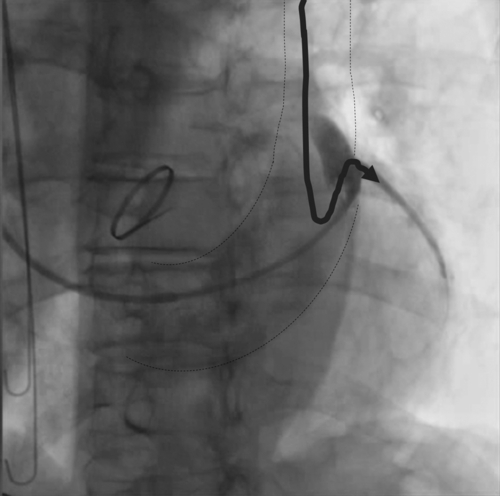
FIGURE 14-3 Left anterior oblique 40-degree view showing a balloon catheter subselecting a lateral branch. Note that access to this branch would be impossible via the left-sided persistent superior vena cava (PLSVC) (curved arrow). The dotted lines outline the contours of the coronary sinus and PLSVC.
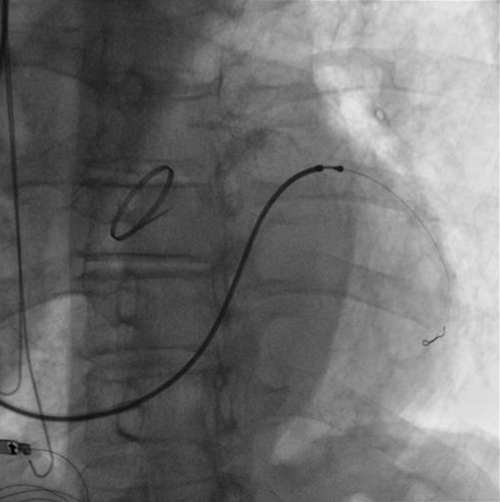
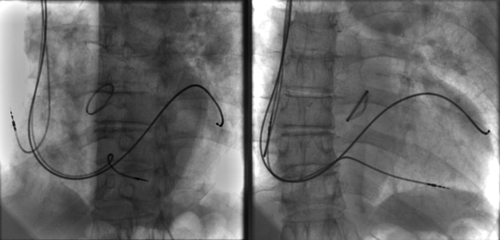
Figure 14-5 Final position of the leads in the 40-degree left anterior oblique (left) and posteroanterior (right) views.
Selected References
1. Biffi M., Bertini M., Ziacchi M. et al. Clinical implications of left superior vena cava persistence in candidates for pacemaker or cardioverter-defibrillator implantation. Heart Vessels. 2009;24:142–146.
2. Ratliff H.L., Yousufuddin M., Lieving W.R. et al. Persistent left superior vena cava: case reports and clinical implications. Int J Cardiol. 2006;113:242–246.


