History
Current Medications
Current Symptoms
Physical Examination
Laboratory Data
Focused Clinical Questions and Discussion Points
Question
Discussion
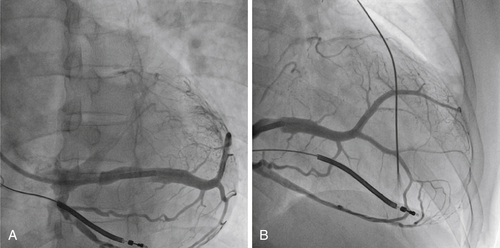
FIGURE 13-1 Subselective coronary sinus venogram in left anterior oblique (A) and right anterior oblique (B). Note that the size of the distal coronary sinus branch is bigger than the size of the guiding catheter.
Question
Discussion
Question
Discussion
Question
Discussion
Plan of Action
Intervention
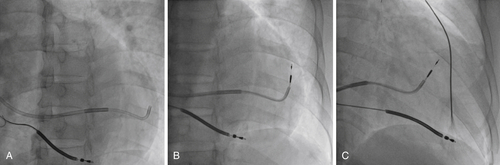
FIGURE 13-2 A 90-degree subselection catheter was used in telescoping fashion to guide the direction of the 3830 lead (A). Once the 3830 lead was in position, the lead was fixated by rotating the lead clockwise for two to three turns. The position of the lead was then checked in the left anterior oblique (B) and right anterior oblique views (C).
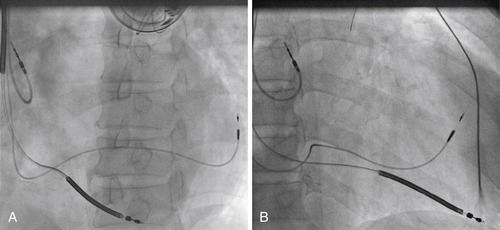
FIGURE 13-3 Final position of the leads in left anterior oblique (A) and right anterior oblique (B) views. Despite the size of the coronary sinus branch being bigger than the size of the lead, the lead retained its position at its fixed location.
Outcome
Selected References
1. Aziz A.F.A., Hussin A., Khelae S.K. et al. Active fixation in the coronary sinus for left ventricular stimulation: an alternative method in improving left sided lead stability and overcoming phrenic nerve stimulation. Heart Rhythm. 2012;5(Suppl):S490.
2. Baranowski B., Yerkey M., Dresing T. et al. Fibrotic tissue growth into the extendable lobes of an active fixation coronary sinus lead can complicate extraction. Pacing Clin Electrophysiol. 2011;34:e64–e65.
3. Luedorff G., Kranig W., Grove R. et al. Improved success rate of cardiac resynchronization therapy implant by employing an active fixation coronary sinus lead. Europace. 2010;12:825–829.
4. Maytin M., Carrillo R.G., Baltodano P. et al. Multicenter experience with transvenous lead extraction of active fixation coronary sinus leads. Pacing Clin Electrophysiol. 2012;35:641–647.