[level-membership-for-cardiovascular-category]
History
Current Medications
Current Symptoms
Physical Examination
Laboratory Data
Electrocardiogram
Findings
Catheterization
Findings
Focused Clinical Questions and Discussion Points
Question

FIGURE 12-1
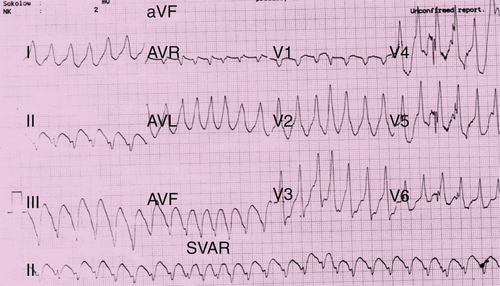
FIGURE 12-2
Discussion
Question
Discussion
Question
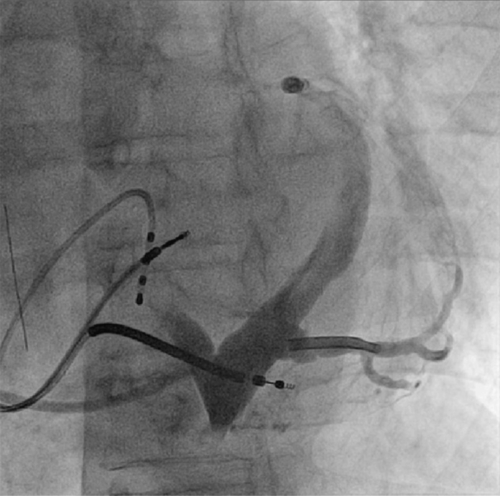
FIGURE 12-3
Discussion
Question
Discussion
Intervention
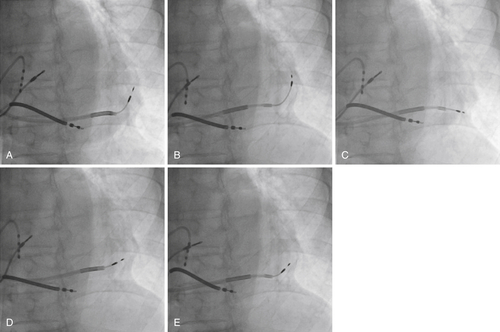
FIGURE 12-4
Outcome
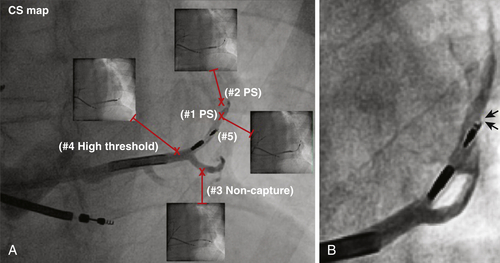
FIGURE 12-5
Selected References
1. Anderson S.E., Hill A.J., Iaizzo P.A. Microanatomy of human left ventricular coronary veins. Anat Rec (Hoboken). 2009;292:23–28.
2. Hansky B., Vogt J., Gueldner H. et al. Implantation of active fixation lead in coronary veins for left ventricular stimulation: report of five cases. Pacing Clin Electrophysiol. 2007;30:44–49.
3. Sanchez-Quintana D., Cabrera J.A., Climent V. et al. How close are the phrenic nerves to cardiac structures? Implications for the cardiac interventionalists. J Cardiovasc Electrophysiol. 2005;16:309–313.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
History
Current Medications
Current Symptoms
Physical Examination
Laboratory Data
Electrocardiogram
Findings
Catheterization
Findings
Focused Clinical Questions and Discussion Points
Question
[/not-level-membership-for-cardiovascular-category]
