Hemodialysis
PREREQUISITE NURSING KNOWLEDGE
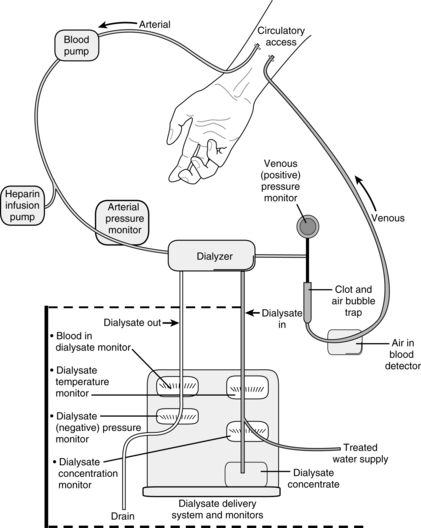
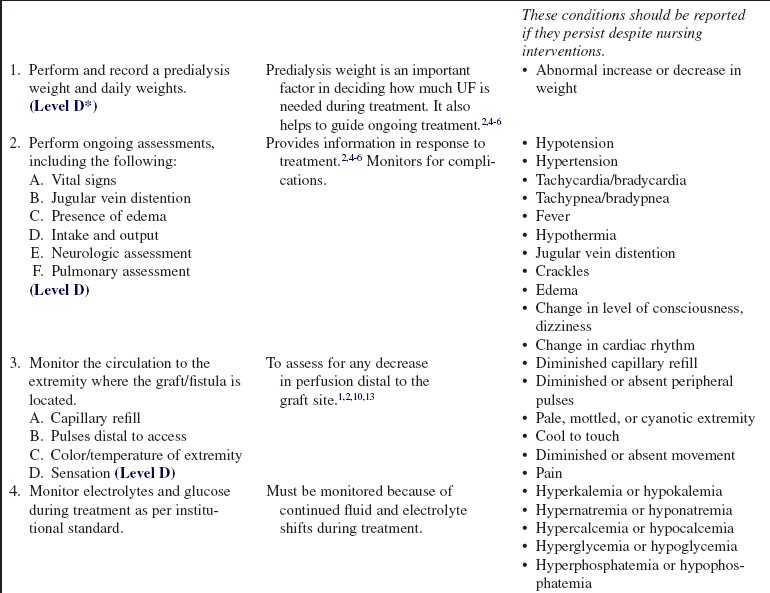
• Hemodialysis (Fig. 113-1) may be needed for the onset of acute renal failure, for maintenance therapy for patients with chronic renal failure, or for patients with acute drug intoxication.9
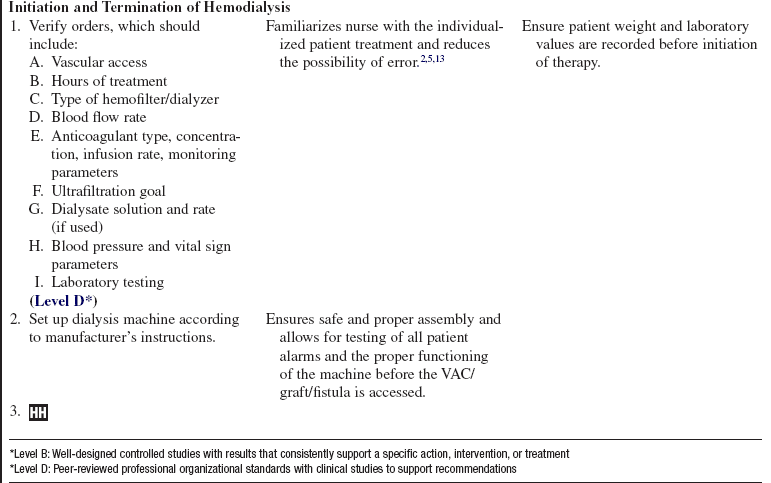
• Requirements for ensuring adequate therapy include: 1, an appropriate prescription; 2, a high level of nursing expertise; 3, an efficiently operating hemodialysis machine; 4, satisfactory access; 5, an informed patient; and 6, ongoing data review.11
• Knowledge of the principles of diffusion, ultrafiltration (UF), osmosis, oncotic pressure, and hydrostatic pressure as they pertain to fluid and solute management during dialysis is neccessary.2,4,5
 Diffusion is the passive movement of solutes through a semipermeable membrane from an area of higher to lower concentration until equilibrium is reached.
Diffusion is the passive movement of solutes through a semipermeable membrane from an area of higher to lower concentration until equilibrium is reached.







• Vascular access is needed to perform hemodialysis and can be provided with a double-lumen vascular access catheter (VAC), an external arteriovenous (AV) shunt, or a surgically created AV anastomosis (e.g., fistula or graft). Common sites for the VAC include the internal jugular or subclavian vein. Common sites for the external shunt include the forearm (radial artery to cephalic vein) or the leg (posterior tibial artery to long saphenous vein). The AV fistula or graft is used for long-term dialysis management.
• The subclavian vein is not recommended for temporary access because of the increased incidence of vascular stenosis, which makes the vein of the ipsilateral arm unsuitable for chronic dialysis if needed. The internal jugular or leg veins are more commonly used.
• Hemodialysis uses an artificial kidney (hemofilter, dialyzer) with a semipermeable membrane to create two separate compartments: the blood compartment and the dialysis solution (dialysate) compartment. The semipermeable membrane allows the movement of small molecules (e.g., electrolytes, urea, drugs) and middle-weight molecules (creatinine) from the patient’s blood into the dialysate but is impermeable to larger molecules (blood cells, plasma proteins).
• Each dialyzer has four ports: two end ports for blood (in one end and out the other) and two side ports for dialysis solution (also in one end and out the other). In most cases, the blood and dialysate are run through the dialyzer in opposite or countercurrent directions.
• The hollow-fiber dialyzer is the most commonly used dialyzer. With this dialyzer, the blood flows through the center of hollow fibers and the dialysate flows around the outside of the hollow fibers. The advantages of hollow-fiber filters include a low priming volume, low resistance to flow, and high amount of surface area. The major disadvantage is the potential for clotting because of the small fiber size.
• Parallel-plate dialyzers are designed as sheets of membrane over supporting structures. Blood and dialysate pass through alternate spaces of the dialyzer. The major disadvantages of this type of filter are the increase in allergic dialyzer reactions and lower filter surface area.
• All dialyzers have UF coefficients; thus, the dialyzer selected varies in different clinical situations. The higher the UF coefficient, the more rapid the fluid removal. UF coefficients are determined with in vivo measurements done by each dialyzer manufacturer.
• Clearance refers to the ability of the dialyzer to remove metabolic waste products from the patient’s blood. The blood flow rate, the dialysate flow rate, and the solute concentration affect clearance. Clearance occurs by the processes of diffusion, convection, and UF.2–4,8–10
• The blood circuit consists of blood lines, a blood pump, and various monitoring devices. The blood lines carry the blood to and from the patient. The blood pump controls the speed of the blood through the circuit. The monitoring devices include arterial and venous pressure monitors and an air detection monitor to prevent air entering the circuit from being returned to the patient.
• The dialysate is composed of water, a buffer (e.g., acetate or bicarbonate), and various electrolytes. Most solutions also contain glucose. The buffer helps neutralize acids that are generated as a result of normal cellular metabolism and usually are excreted by the kidney. The concentration of electrolytes is usual normal plasma concentrations, which help to create a concentration gradient for removal of excess electrolytes. The glucose, available in various concentrations, promotes the removal of plasma water.
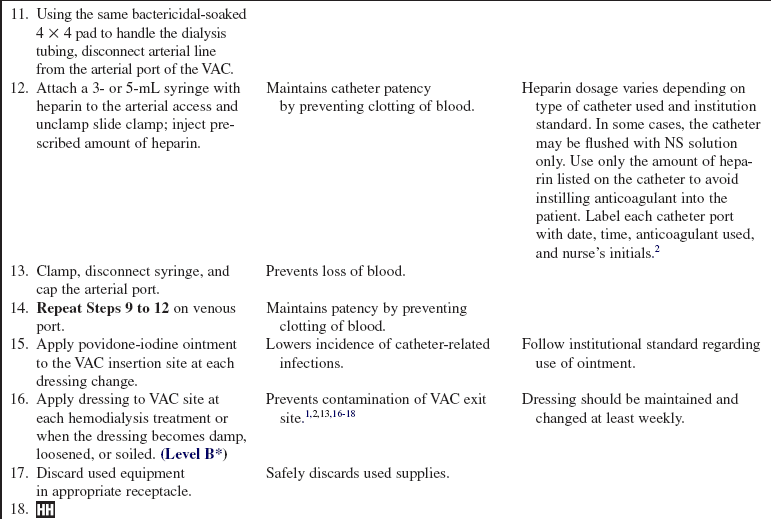
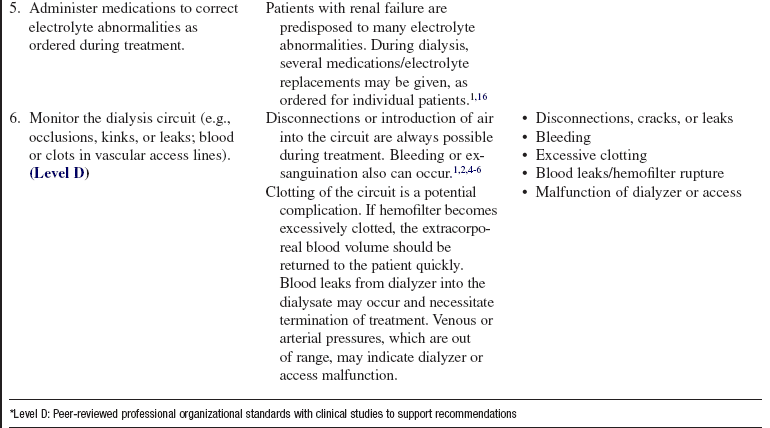
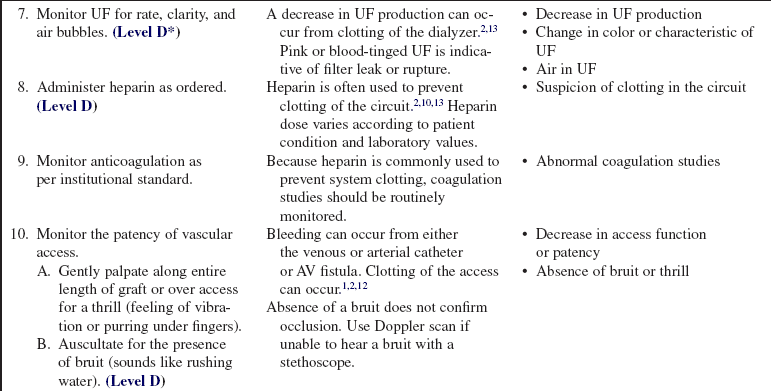
• Heparin is usually used during dialysis to prevent clotting of the circuit. In patients with coagulopathies, normal saline solution flushes can be used to keep the blood circuit patent.5 Heparin should be avoided in patients with a history of heparin-induced thrombocytopenia (HIT).2,10
• Because large volumes of water are used during treatments to generate the dialysate, the water must be purified before patient use to prevent patient exposure to potentially harmful substances present in the water supply (e.g., calcium carbonate, sodium chloride, and iron).
• Other extended renal replacement therapy techniques or “hybrid” techniques (sustained low-efficiency dialysis [SLED], extended daily dialysis [EDD]) generally use standard hemodialysis equipment and techniques with reduced blood flow and dialysate rates to gradually remove plasma water and solutes in the critically ill patient. They are used from 4 to 12 hours a day.8
• The adequacy of dialysis and assessment of the patient’s residual renal function should be evaluated on a periodic basis. Adequacy of dialysis can be measured with urea kinetic modeling (Kt/V) or urea clearance.2,4,14,15 Residual renal functioning can be monitored with urine creatinine clearance.14,15 Collaboration with the nephrology team is necessary to monitor these parameters.2,4,5
EQUIPMENT
• Fluid shield face masks or goggles
• Sterile and nonsterile gloves
• Sterile normal saline (NS) solution, 3 L
• Two 10-mL syringes with blunt-tip cannulas
• Dressing supplies (sterile barrier, 4 × 4 gauze pads, transparent dressing, tape)
• Povidone-iodine, hypochlorite, or chlorhexidine bactericidal solution (follow institution standard)
• Heparin (1000 units/mL; for both priming and infusion, as ordered)
• Sterile bowl for soaking of 4 × 4 pads with bactericidal solution
Additional equipment for graft cannulation includes the following:
• Two 10-mL syringes with blunt-tip cannulas
• 1% lidocaine and two tuberculin syringes with 25-gauge needles
Additional equipment for initiation of hemodialysis includes the following:
Additional equipment, to have available depending on patient need, includes the following:






PATIENT AND FAMILY EDUCATION
• Explain the procedure and review any questions the patient may have.  Rationale: Explanation provides information and may decrease patient anxiety.
Rationale: Explanation provides information and may decrease patient anxiety.
• Explain the need for sterile technique for the duration of treatment.  Rationale: Explanation decreases the chance of systemic infection because pathogens can be transported throughout the entire body via the circulation.
Rationale: Explanation decreases the chance of systemic infection because pathogens can be transported throughout the entire body via the circulation.
• Explain the purpose of hemodialysis.  Rationale: Hemodialysis is necessary to perform the physiologic functions of the kidneys when renal failure is present.
Rationale: Hemodialysis is necessary to perform the physiologic functions of the kidneys when renal failure is present.
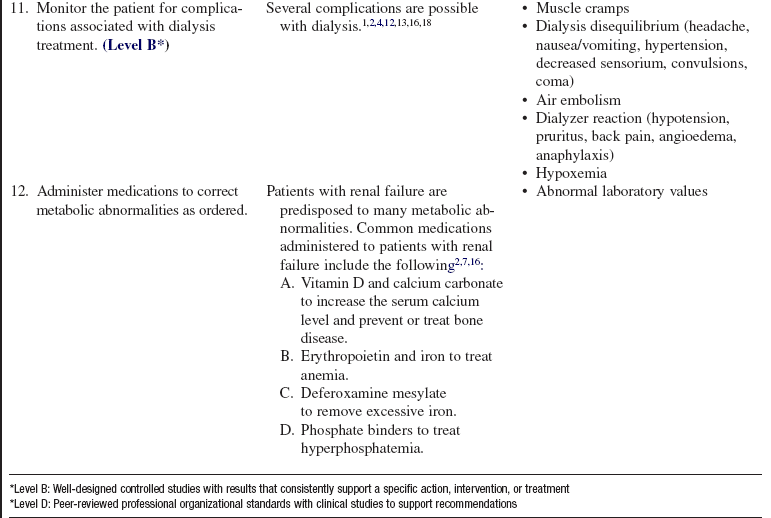
• Explain the need for careful monitoring of the patient during the treatment for fluid and electrolyte imbalance.  Rationale: Dialysis treatment puts the patient at risk for imbalance because of the rapid movement of fluid and electrolytes from the patient during treatment.
Rationale: Dialysis treatment puts the patient at risk for imbalance because of the rapid movement of fluid and electrolytes from the patient during treatment.
• Explain the importance of input from the patient on how he or she is feeling during the treatment.  Rationale: Hypotension is a common occurrence during treatment; the patient may experience light-headedness or dizziness if hypotension is present. Patient knowledge of this possibility should help decrease anxiety.
Rationale: Hypotension is a common occurrence during treatment; the patient may experience light-headedness or dizziness if hypotension is present. Patient knowledge of this possibility should help decrease anxiety.
• Explain the hemodialysis circuit setup to the patient.  Rationale: The patient and family must be aware that blood will be removed from the patient’s body and will be visible during the hemodialysis treatment.
Rationale: The patient and family must be aware that blood will be removed from the patient’s body and will be visible during the hemodialysis treatment.
PATIENT ASSESSMENT AND PREPARATION
Patient Assessment
• Assess baseline vital signs, weight, neurologic status, physical assessment of all body systems, and fluid and electrolyte status.  Rationale: Patients in renal failure often have altered baseline assessments, both in physical assessment and in the laboratory values. Having this information before treatments are started is helpful so that interventions, including the dialysate, can be individualized. Alterations during treatment are common because of the rapid removal of fluid and solutes.
Rationale: Patients in renal failure often have altered baseline assessments, both in physical assessment and in the laboratory values. Having this information before treatments are started is helpful so that interventions, including the dialysate, can be individualized. Alterations during treatment are common because of the rapid removal of fluid and solutes.
• Assess graft, fistula, or VAC site for signs or symptoms of infection.  Rationale: Because dialysis access sites are used frequently, infection is always a potential risk. Dialysis access sites should only be used for dialysis, and not for other intravenous access needs, except in an emergency situation. Insertion sites provide a portal of entry for infection, which may result in septicemia if unrecognized or untreated. If the insertion site appears to be infected, further interventions (e.g., site change, culture, and antibiotic treatment) may be necessary.
Rationale: Because dialysis access sites are used frequently, infection is always a potential risk. Dialysis access sites should only be used for dialysis, and not for other intravenous access needs, except in an emergency situation. Insertion sites provide a portal of entry for infection, which may result in septicemia if unrecognized or untreated. If the insertion site appears to be infected, further interventions (e.g., site change, culture, and antibiotic treatment) may be necessary.
• Assess VAC patency and the ability to easily aspirate blood from both ports.  Rationale: Adequate blood flow is necessary during a treatment to facilitate optimal fluid and solute removal. Patent VAC ports are necessary for adequate blood flow.
Rationale: Adequate blood flow is necessary during a treatment to facilitate optimal fluid and solute removal. Patent VAC ports are necessary for adequate blood flow.
• With AV fistula use, assess the site for presence of bruit, erythema, swelling, and quality of blood flow.  Rationale: Physical assessment of the fistula can indicate patency of the graft and the possible presence of infection.
Rationale: Physical assessment of the fistula can indicate patency of the graft and the possible presence of infection.
• Assess the circulation to the distal parts of the access limb.  Rationale: The placement of a vascular access may compromise circulation.
Rationale: The placement of a vascular access may compromise circulation.
Patient Preparation
• Verify correct patient with two identifiers.  Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
• Ensure the patient understands preprocedural teachings. Answer questions as they arise, and reinforce information as needed.  Rationale: Understanding of previously taught information is evaluated and reinforced.
Rationale: Understanding of previously taught information is evaluated and reinforced.
• Position the patient in a comfortable position (that also facilitates optimal blood flow through the access site and allows for the setup of a sterile field).  Rationale: Facilitation of patient comfort helps to minimize the amount of patient movement during treatment, which can change the amount of blood flow through the access site. Different access sites may require different patient positions to facilitate optimal blood flow.
Rationale: Facilitation of patient comfort helps to minimize the amount of patient movement during treatment, which can change the amount of blood flow through the access site. Different access sites may require different patient positions to facilitate optimal blood flow.
• With AV fistula use, ask the patient whether he or she wants lidocaine used on the access site before the fistula is accessed.  Rationale: Patient comfort is promoted, and anxiety may be reduced.
Rationale: Patient comfort is promoted, and anxiety may be reduced.
References
![]() 1. Allon, M, Dialysis catheter-related bacteremia. treatment and prophylaxis. Am J Kidney Dis 2004; 44:779–791.
1. Allon, M, Dialysis catheter-related bacteremia. treatment and prophylaxis. Am J Kidney Dis 2004; 44:779–791.
2. Amato, RL. Hemodialysis. In: Counts CS, et al, eds. Core curriculum for nephrology nursing. ed 5. Pitman, -NJ: American Nephrology Nurses Association; 2008,:-657–681.
3. Bouman, CS, High-volume hemofiltration as adjunctive therapy for sepsis and systemic inflammatory response -syndrome. background, definition and a descriptive analysis of animal and human studies. Adv Sepsis 2007; 6:74–77.
![]() 4. Burrows-Hudson S, Prowant, B. Nephrology nursing standards of practice and guidelines for care,. Pitman, NJ: American Nephrology Nurses Association; 2005,.
4. Burrows-Hudson S, Prowant, B. Nephrology nursing standards of practice and guidelines for care,. Pitman, NJ: American Nephrology Nurses Association; 2005,.
5. Challinor, P. Hemodialysis. In: Thomas N, ed. Renal nursing. ed 3. Edinburg: Ballierre Tindall; 2008:181–222.
![]() 6. Dinwiddie, LC, Managing catheter dysfunction for better patient outcomes. a team approach. Nephrol Nurs J 2004; 31:653–660.
6. Dinwiddie, LC, Managing catheter dysfunction for better patient outcomes. a team approach. Nephrol Nurs J 2004; 31:653–660.
7. Goldstein-Fuchs, J, Contemporary nephrology nursing. principles and practice. Molzahn, A. Butera, E. Nutrition and chronic kidney disease. ed 2. American Nephrology Nurses’ Association, Pitman, NJ, 2006:371–391.
![]() 8. Golper, T, Hybrid renal replacement therapies in critically ill patients. sepses, kidney and multiple organ dysfunction. Contrib Nephrol 2004; 114:278–283.
8. Golper, T, Hybrid renal replacement therapies in critically ill patients. sepses, kidney and multiple organ dysfunction. Contrib Nephrol 2004; 114:278–283.
![]() 9. Kellum, JA, et al. The 3rd International Consensus -Conference of the Acute Dialysis Quality Initiative (ADQI). Int J Artif Organs. 2005; 28:441–444.
9. Kellum, JA, et al. The 3rd International Consensus -Conference of the Acute Dialysis Quality Initiative (ADQI). Int J Artif Organs. 2005; 28:441–444.
![]() 10. Kraus, MA, Renal replacement therapy, part 1. indications and modalitiesMolitoris BA, ed.. Critical care -nephrology. Remedica: London, 2005,:151–156.
10. Kraus, MA, Renal replacement therapy, part 1. indications and modalitiesMolitoris BA, ed.. Critical care -nephrology. Remedica: London, 2005,:151–156.
11. Latham, CE. Hemodialysis technology. In: Molzahn A, Butera E, eds. Contemporary nephrology nursing: principles and practice. ed 2. Pitman, NJ: American Nephrology Nurses’ Association; 2006:548.
12. MacRae, JM, et al, The cardiovascular effects of -arteriovenous fistulas in chronic kidney disease. a cause for concern. Semin Dialysis 2006; 19:349–352.
13. National Kidney Foundation (NKF), KDOQI clinical practice guidelines for vascular access. update 2006. Am J Kidney Dis 2006; 48:S176–S307.
![]() 14. Palevsky, PM, et al, Design of the VA/NIH Acute Renal Failure Trial Network (AN) Study. intensive versus conventional renal support in acute renal failure. Clin Trials 2005; 2:423–435.
14. Palevsky, PM, et al, Design of the VA/NIH Acute Renal Failure Trial Network (AN) Study. intensive versus conventional renal support in acute renal failure. Clin Trials 2005; 2:423–435.
15. Palevsky, PM, et al. Intensity of renal support in critically ill patients with acute kidney injury. N Engl J Med. 2008; 359:7–20.
16. Robins, DC, Hemodialysis. prevention and management of treatment complicationsMolzahn A, Butera E, eds.. Contemporary nephrology nursing: principles and practice. ed 2. American -Nephrology Nurses’ Association, Pitman, NJ, 2006:581–623.
17. White, RB. Vascular access for hemodialysis. In: Molzahn A, Butera E, eds. Contemporary nephrology nursing: principles and practice. ed 2. Pitman, NJ: American Nephrology Nurses’ Association; 2006:559–578.
![]() 18. Young, EJ, et al. Incidence and influencing factors associated with exit site infections in temporary catheters for hemodialysis and apheresis. Nephrol Nurs J. 2005; 32:41–50.
18. Young, EJ, et al. Incidence and influencing factors associated with exit site infections in temporary catheters for hemodialysis and apheresis. Nephrol Nurs J. 2005; 32:41–50.
Ball, L. The buttonhole technique for arteriovenous fistula cannulation. Nephrol Nurs J. 2006; 33:299–304.
Bellomo, R, et al, Acute renal failure. definition, outcome measures, animal models, fluid therapy and information technology needsthe Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care 2004; 8:R204–R212.
Burrowes, JD, Van Houten, G. Herbs and dietary supplement use in patients with stage 5 chronic kidney disease. Nephrol Nurs J. 2006; 33:85–88.
Fry, AC, Farrington, K. Management of acute renal failure. Postgrad Med J. 2006; 82:106–116.
Desai, AA, et al, Identifying best practices in dialysis care. results of cognitive interviews and a national survey of dialysis providers. Clin J Am Soc Nephrol 2008; 3:1066–1076.
Denhaerynck, K, et al. Prevalence and consequences of nonadherence to hemodialysis regimens. Am J Crit Care. 2007; 16:222–235.
Gomez, N, Practice issues in nephrology nursing. focus on -issues from ANNA’s special interest groupsNational Symposium Special Interest Group presentations. Nephrol Nurs J/J Am Nephrol Nurs Assoc 2003; 30:333–341.
Liangos, O, Epidemiology and outcomes of acute renal failure in hospitalized patients. a national survey. Clin J Am Soc Nephrol 2006; 1:43–51.
Metta, R, et al, Spectrum of acute renal failure in the intensive care unit. the PICARD experience. Kidney Int 2004; 66:-1613–1621.
Ostermann, M, et al. Acute kidney injury in the intensive care unit according to RIFLE. Crit Care Med. 2007; 35:1837–1843.
Overberger, P, et al, Management of renal replacement therapy in acute kidney injury. a survey of practitioner prescribing practices. Clin J Am Soc Nephrol 2007; 2:623–630.
Pupim, LB, et al. Nutrition and metabolism in kidney disease. Semin Nephrol. 2006; 26:134–157.
Rauf, AA, et al. J Intensive Care Med. 2008; 23:195–203.
Uchino, S, et al, Acute renal failure in critically ill patients . a multinational, multicenter study. JAMA 2005; 294:813–818.
