 Arterial Catheter Insertion (Perform)
Arterial Catheter Insertion (Perform)
PREREQUISITE NURSING KNOWLEDGE
• Knowledge of anatomy and physiology of the vasculature and adjacent structures is needed.
• Nurses must be adequately prepared to insert arterial catheters. This preparation should include specific educational content about arterial catheter insertion and opportunities to demonstrate clinical competency.
• Understanding of the principles of hemodynamic monitoring is necessary.
• Clinical competence in suturing is needed.
• Conditions that warrant the use of arterial pressure monitoring include patients with the following:
 Acute hypotension or hypertension (hypertensive crisis)
Acute hypotension or hypertension (hypertensive crisis)
 Hemodynamic instability or circulatory collapse
Hemodynamic instability or circulatory collapse



 Continuous infusion of vasoactive medications
Continuous infusion of vasoactive medications
 Frequent arterial blood gas measurements
Frequent arterial blood gas measurements

 Intraaortic balloon pump therapy
Intraaortic balloon pump therapy







• Noninvasive indirect blood pressure measurements determined with auscultation of Korotkoff sounds distal to an occluding cuff consistently average 10 to 20 mm Hg lower than simultaneous direct measurement.13
• Arterial waveform inspection can help with rapid diagnosis of the presence of valvular disorders, and determine the effects of dysrhythmias on perfusion, the effects of the respiratory cycle on blood pressure, and the effects of intraaortic balloon pump therapy or ventricular assist device therapy on blood pressure.
• The preferred artery for arterial catheter insertion is the radial artery (see Fig. 80-1). Although this artery is smaller than the ulnar artery, it is more superficial and can be more easily stabilized during the procedure.9 The brachial artery is a safe and reliable alternative site for arterial puncture and line placement.18
• At times, the femoral artery may be used for arterial catheter insertion. The use of this artery can be technically difficult because of the proximity of the femoral artery to the femoral vein (see Fig. 80-2).
• The most common complications associated with arterial puncture include pain, vasospasm, hematoma formation, infection, hemorrhage, and neurovascular compromise.3,8,19
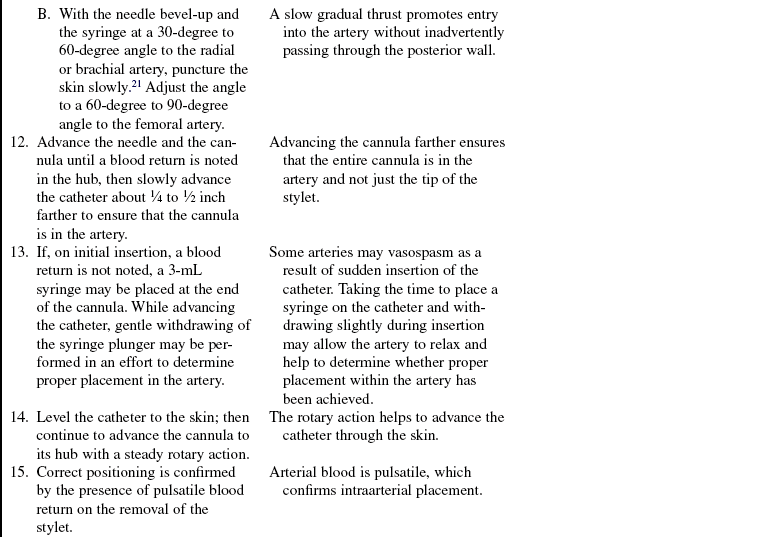
• Causes of failure to cannulate the artery include a tangential approach to the artery, tortuosity of the artery or arterial spasm, or impingement of the needle tip on the posterior wall.20
• Site selection is as follows:
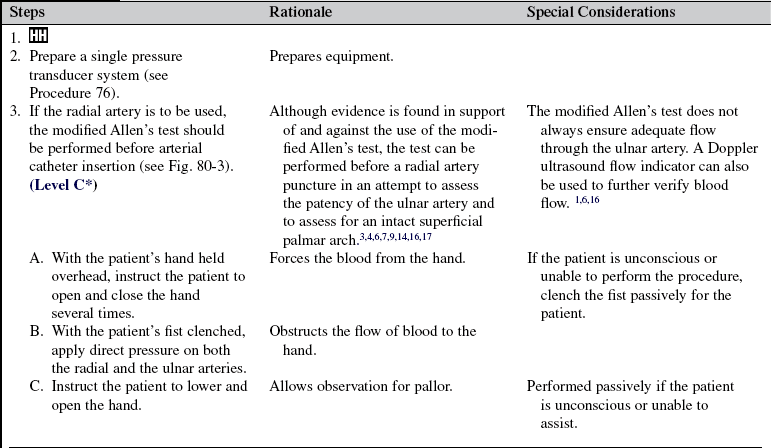
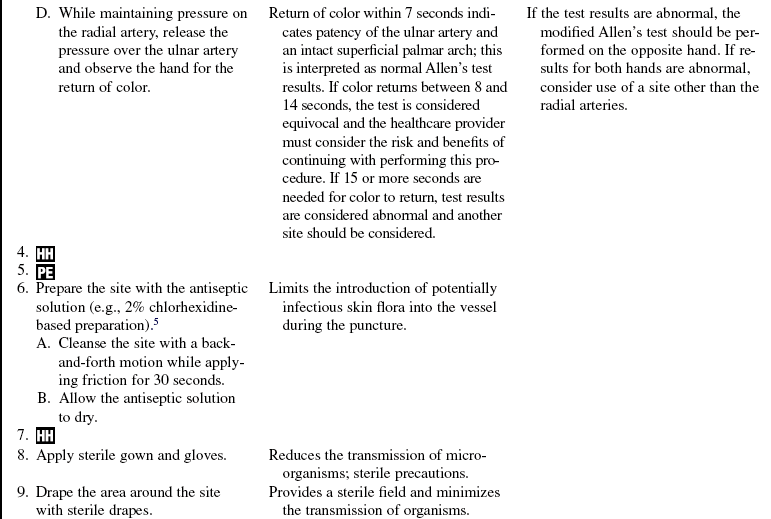
 Use the radial artery as the first choice. Conduct a modified Allen’s test before performing an arterial puncture on the radial artery (see Fig. 80-3). Normal palmar blushing is complete before 7 seconds, indicating a positive result; 8 to 14 seconds is considered equivocal; and 15 or more seconds indicates a negative test result. Doppler flow studies or plethysmography can also be performed to ensure the presence of collateral flow. Research shows these studies to be more reliable than the modified Allen’s test.1,20 Thrombosis of the arterial cannula is a common complication. Ensuring collateral flow distal to the puncture site is important for prevention of ischemia. Puncture of both the radial and ulnar arteries on the same hand is never recommended, to prevent compromising blood supply to the hand.4,10,14,16
Use the radial artery as the first choice. Conduct a modified Allen’s test before performing an arterial puncture on the radial artery (see Fig. 80-3). Normal palmar blushing is complete before 7 seconds, indicating a positive result; 8 to 14 seconds is considered equivocal; and 15 or more seconds indicates a negative test result. Doppler flow studies or plethysmography can also be performed to ensure the presence of collateral flow. Research shows these studies to be more reliable than the modified Allen’s test.1,20 Thrombosis of the arterial cannula is a common complication. Ensuring collateral flow distal to the puncture site is important for prevention of ischemia. Puncture of both the radial and ulnar arteries on the same hand is never recommended, to prevent compromising blood supply to the hand.4,10,14,16


EQUIPMENT
• 2-inch, 20-gauge, nontapered Teflon cannula-over-needle; or prepackaged kit that includes a 6-inch, 18-gauge, Teflon catheter with appropriate introducer and guidewire
• Single-pressure transducer system (see Procedure 76)
• Monitoring equipment consisting of a connecting cable, monitor, oscilloscope display screen, and recorder
• Nonsterile gloves, head covering, goggles
• Antiseptic solution (e.g., 2% chlorhexidine-based preparation)
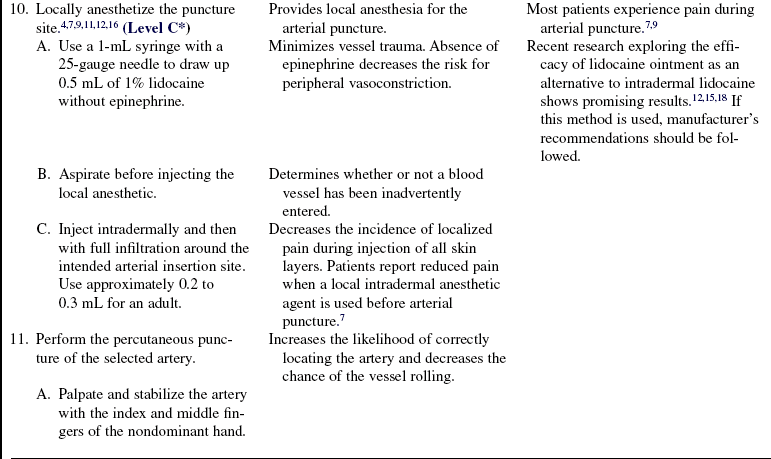
• 1% lidocaine without epinephrine, 1 to 2 mL
Additional supplies to have available as needed include the following:
PATIENT AND FAMILY EDUCATION
• Explain the procedure and the purpose of the arterial catheter.  Rationale: This explanation decreases patient and family anxiety.
Rationale: This explanation decreases patient and family anxiety.
• Explain to the patient that the procedure may be uncomfortable but that a local anesthetic will be used first to alleviate most of the discomfort.  Rationale: Patient cooperation is elicited, and insertion is facilitated.
Rationale: Patient cooperation is elicited, and insertion is facilitated.
• Explain the patient’s role in assisting with catheter insertion.  Rationale: This explanation elicits patient cooperation and facilitates insertion.
Rationale: This explanation elicits patient cooperation and facilitates insertion.
PATIENT ASSESSMENT AND PREPARATION
Patient Assessment
• Obtain the patient’s medical history, including history of diabetes, hypertension, peripheral vascular disease, vascular grafts, arterial vasospasm, thrombosis, or embolism. Obtain the patient’s history of coronary artery bypass graft surgery in which radial arteries were removed for use as conduits or presence of arteriovenous (AV) fistulas or shunts.  Rationale: Extremities with any of these problems should be avoided as sites for cannulation because of the potential for complications. Patients with diabetes mellitus or hypertension are at higher risk for arterial or venous insufficiency. Previously removed radial arteries are a contraindication for ulnar artery cannulation.
Rationale: Extremities with any of these problems should be avoided as sites for cannulation because of the potential for complications. Patients with diabetes mellitus or hypertension are at higher risk for arterial or venous insufficiency. Previously removed radial arteries are a contraindication for ulnar artery cannulation.
• Assess the patient’s medical history of coagulopathies, use of anticoagulant therapy, vascular abnormalities, or peripheral neuropathies.  Rationale: This assessment assists in determining safety of the procedure and aids in site selection.
Rationale: This assessment assists in determining safety of the procedure and aids in site selection.
• Assess the patient’s allergy history (e.g., allergy to lidocaine, topical anesthetic cream, antiseptic solutions, or tape).  Rationale: This assessment decreases the risk for allergic reactions.
Rationale: This assessment decreases the risk for allergic reactions.
• Assess the patient’s current anticoagulation therapy, known blood dyscrasias, and pertinent laboratory values (e.g., platelet levels, partial thromboplastin time [PTT], prothrombin time [PT], and International normalized ratio [INR]) before the procedure.  Rationale: Anticoagulation therapy, blood dyscrasias, or alterations in coagulation studies could increase the risk for hematoma formation or hemorrhage.
Rationale: Anticoagulation therapy, blood dyscrasias, or alterations in coagulation studies could increase the risk for hematoma formation or hemorrhage.
• Assess the intended insertion site for the presence of a strong pulse.  Rationale: Identification and localization of the pulse increases the chance of a successful arterial cannulation.
Rationale: Identification and localization of the pulse increases the chance of a successful arterial cannulation.
• Presence of collateral flow to the area distal to the arterial catheter should be evaluated before the artery is cannulated. For radial arterial lines, a modified Allen’s test should be performed.  Rationale: This assessment determines the presence of collateral flow to the hand to reduce vascular complications.
Rationale: This assessment determines the presence of collateral flow to the hand to reduce vascular complications.
• If available, assess the intended artery with a Doppler ultrasound scan.  Rationale: This assessment aids in determination of the patency of the artery and blood flow.1,2,16 Identification and localization of the artery to be cannulated increases the chance of a successful cannulization and reduces the complication rate and need for multiple attempts at placement.19
Rationale: This assessment aids in determination of the patency of the artery and blood flow.1,2,16 Identification and localization of the artery to be cannulated increases the chance of a successful cannulization and reduces the complication rate and need for multiple attempts at placement.19
Patient Preparation
• Verify correct patient with two identifiers.  Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
• Perform a pre-procedure verification and time out, if non-emergent.  Rationale: Ensures patient safety.
Rationale: Ensures patient safety.
• Ensure that the patient and family understand preprocedural teaching. Answer questions as they arise and reinforce information as needed.  Rationale: Understanding of previously taught information is evaluated and reinforced.
Rationale: Understanding of previously taught information is evaluated and reinforced.
• Obtain informed consent.  Rationale: Informed consent protects the rights of the patient and makes a competent decision possible for the patient; however, in emergency circumstances, time may not allow the form to be signed.
Rationale: Informed consent protects the rights of the patient and makes a competent decision possible for the patient; however, in emergency circumstances, time may not allow the form to be signed.
• Place the patient supine with the head of the bed at a comfortable position. The limb into which the arterial catheter will be inserted should be resting comfortably on the bed.  Rationale: This placement provides patient comfort and facilitates insertion.
Rationale: This placement provides patient comfort and facilitates insertion.
• Place a towel under the back of the wrist to hyperextend the wrist and tape it in place or have someone hold it (if the radial artery is being used).  Rationale: This placement positions the arm and brings the artery closer to the surface.
Rationale: This placement positions the arm and brings the artery closer to the surface.
• Elevate and hyperextend the patient’s arm. Support the arm with a pillow (when using the brachial artery).  Rationale: This action increases accessibility of the artery.
Rationale: This action increases accessibility of the artery.
• When the femoral artery is used, position the patient supine with the head of the bed at a comfortable angle. The patient’s leg should be straight with the femoral area easily accessible.  Rationale: This position is the best for localizing the femoral artery pulse.
Rationale: This position is the best for localizing the femoral artery pulse.
References
![]() 1. Abu-Omar Y, et al. Duplex ultrasonography predicts safety of radial artery harvest in the presence of an abnormal -Allen test. Ann Thorac Surg. 2004; 77:116–119.
1. Abu-Omar Y, et al. Duplex ultrasonography predicts safety of radial artery harvest in the presence of an abnormal -Allen test. Ann Thorac Surg. 2004; 77:116–119.
2. Barone, JE, Madlinger, RV. Should an Allen test be performed before artery cannulation. J Trauma. 2006; 61:468–470.
![]() 3. Buffington, S. Specimen collection and testing. In: Nattina, Sandra M, eds. Lippincott’s nursing procedures. ed 2. Springhouse, PA: Springhouse Corp; 1996:145–147.
3. Buffington, S. Specimen collection and testing. In: Nattina, Sandra M, eds. Lippincott’s nursing procedures. ed 2. Springhouse, PA: Springhouse Corp; 1996:145–147.
4. Celenski, SA, Seneff, MG, et al. Arterial line placement and care. In: Irwin RS, ed. Procedures and techniques in intensive care medicine. ed 6. Philadelphia: Lippincott Williams & Wilkins; 2008:38–46.
![]() 5. Centers for Disease Control and Prevention. Guidelines for the prevention of intravascular catheter-related infections. MMWR. 2002; 51(RR-10):1–31.
5. Centers for Disease Control and Prevention. Guidelines for the prevention of intravascular catheter-related infections. MMWR. 2002; 51(RR-10):1–31.
6. Chernecky CC, Berger BJ, eds. Laboratory tests and diagnostic procedures, ed 5, St Louis: Saunders Elsevier, 2008.
![]() 7. Clarke, S, Arterial lines. an analysis of good practice. J Child Healthcare 1999; 3:22–27.
7. Clarke, S, Arterial lines. an analysis of good practice. J Child Healthcare 1999; 3:22–27.
![]() 8. Cummins RO, ed.. Advanced cardiac life support. 1997. American Heart Association: Dallas:13. 9–13. 10.
8. Cummins RO, ed.. Advanced cardiac life support. 1997. American Heart Association: Dallas:13. 9–13. 10.
![]() 9. Giner, J, et al. Pain during arterial puncture. Chest. 1996; 110:1443–1445.
9. Giner, J, et al. Pain during arterial puncture. Chest. 1996; 110:1443–1445.
10. Gomella, LG, Haist, SA, Bedside proceduresGomella LG, Haist SA, eds.. Clinician’s pocket reference: the scut monkey. ed 11. 2007. www.accessmedicine.com/content.aspx?aID=2694363 [available at].
11. Hudson, TL, Dukes, SF, Reilly, K. Use of local anesthesia for arterial punctures. Am J Crit Care. 2006; 15:595–599.
![]() 12. Hussey, VM, Poulin, MV, Fain, JA. Effectiveness of lidocaine hydrochloride on venipuncture sites. AORN J. 1997; 66:472–475.
12. Hussey, VM, Poulin, MV, Fain, JA. Effectiveness of lidocaine hydrochloride on venipuncture sites. AORN J. 1997; 66:472–475.
![]() 13. Imperial-Perez, F, McRae, M, Protocols for practice . hemodynamic monitoring series. arterial pressure monitoring. American Association of Critical-Care Nurses, Aliso Viejo, CA, 1998.
13. Imperial-Perez, F, McRae, M, Protocols for practice . hemodynamic monitoring series. arterial pressure monitoring. American Association of Critical-Care Nurses, Aliso Viejo, CA, 1998.
14. Intravenous Nurses Society. Infusion nursing standards of practice. J Infusion Nurs. 2006; 29(1 Suppl):S1–92. [Jan-Feb].
![]() 15. Martin, C, et al. Long-term arterial cannulation in ICU patients using the radial artery or dorsalis pedis artery. Chest. 2001; 119:901–906.
15. Martin, C, et al. Long-term arterial cannulation in ICU patients using the radial artery or dorsalis pedis artery. Chest. 2001; 119:901–906.
![]() 16. National Committee for Clinical Laboratory Standards, Procedures for the collection of arterial blood specimens. approved standards H11-A4. ed 4. National Committee for Clinical Laboratory Standards, Wayne, PA, 2004.
16. National Committee for Clinical Laboratory Standards, Procedures for the collection of arterial blood specimens. approved standards H11-A4. ed 4. National Committee for Clinical Laboratory Standards, Wayne, PA, 2004.
17. Oettle, AC, et al. Evaluation of Allen’s test in both arms and arteries of left and right-handed people. Surg Radiol Anat. 2006; 28:3–6.
![]() 18. Okeson, GC, Wulbrecht, PH. The safety of brachial artery puncture for arterial blood sampling. Chest. 1998; 114:748–751.
18. Okeson, GC, Wulbrecht, PH. The safety of brachial artery puncture for arterial blood sampling. Chest. 1998; 114:748–751.
![]() 19. Qvist, J, Peterfreund, R, Perlmutter, G. Transient compartment syndrome of the forearm after attempted radial artery cannulation. Anesth Anal. 1996; 83:183–185.
19. Qvist, J, Peterfreund, R, Perlmutter, G. Transient compartment syndrome of the forearm after attempted radial artery cannulation. Anesth Anal. 1996; 83:183–185.
20. Shiver, S, Blaivas, M, Lyon, M. A prospective comparison of ultrasound-guided and blindly placed radial arterial catheters. Acad Emerg Med. 2006; 13:1275–1279.
![]() 21. Williams, DJ, Ahmed, ST, Latto, IP. A survey of venous and arterial cannulation techniques used for routine adult coronary artery bypass grafting. Internet J Anesthesiol. 2003; 6:12.
21. Williams, DJ, Ahmed, ST, Latto, IP. A survey of venous and arterial cannulation techniques used for routine adult coronary artery bypass grafting. Internet J Anesthesiol. 2003; 6:12.
