[level-membership-for-cardiovascular-category]
History
Current Medications
Physical Examination
Hospital and Procedural Course

Focused Clinical Questions and Discussion Points
Question
Discussion
Question
Discussion
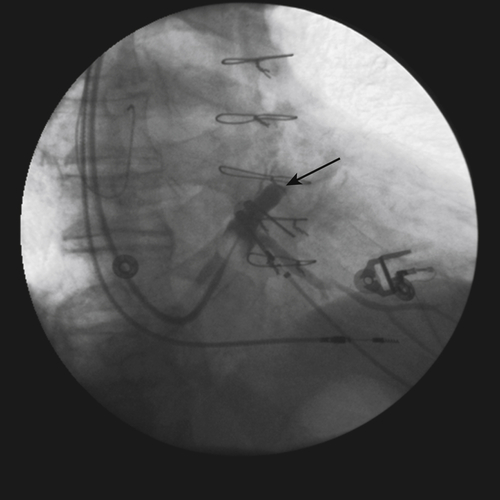
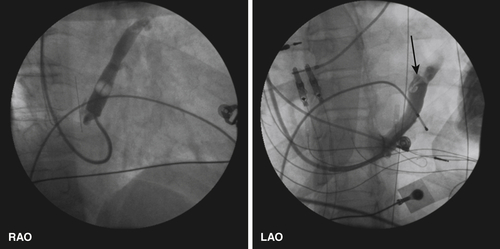
FIGURE 11-2
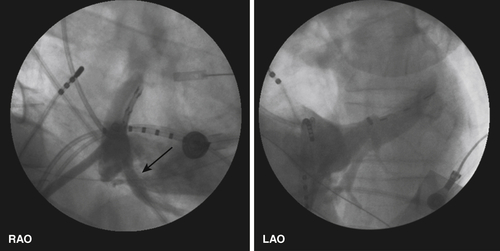
FIGURE 11-3
Question
Discussion
Intervention
 (see Video 11-1). The MCV drains the inferior aspect of the posterior left ventricle; the posterior vein provides a more direct access to the lateral region of the left ventricle. Nonetheless, these distinct venous systems exhibit a high occurrence of anastomoses, resulting in an interconnected venous system near the posterolateral wall of the left ventricle.1 Thus it is useful to recognize these collaterals between the middle cardiac and posterior venous system to the lateral wall. This can be done with occlusion venography in the body of the coronary vein, coronary sinus, or subselective angiography of the MCV (Figure 11-5).
(see Video 11-1). The MCV drains the inferior aspect of the posterior left ventricle; the posterior vein provides a more direct access to the lateral region of the left ventricle. Nonetheless, these distinct venous systems exhibit a high occurrence of anastomoses, resulting in an interconnected venous system near the posterolateral wall of the left ventricle.1 Thus it is useful to recognize these collaterals between the middle cardiac and posterior venous system to the lateral wall. This can be done with occlusion venography in the body of the coronary vein, coronary sinus, or subselective angiography of the MCV (Figure 11-5).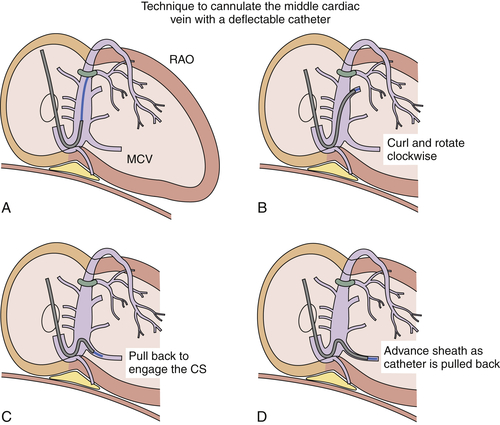
FIGURE 11-4

FIGURE 11-5
FIGURE 11-6
Focused Clinical Questions and Discussion Points
Question
Discussion
FIGURE 11-7
FIGURE 11-8
FIGURE 11-9
FIGURE 11-10
Outcome
Selected References
1. Anderson S.E., Lahm R., Iaizzo P.A. The coronary vascular system and associated medical devices. In: Iaizzo P.A., ed. Handbook of cardiac anatomy, physiology, and devices. Totowa, NJ: Humana; 2005:109–124.
2. Asirvatham S.J. Anatomy of the coronary sinus. In: Yu C.M., Hayes D.L., Auricchio A., eds. Cardiac resynchronization therapy. Malden: Blackwell Futura; 2008:211–238.
3. Bogaert J. Cardiac function. In: Bogaert J., Dymarkowski S., Taylor A.M., Muthurangu V., eds. Clinical cardiac MRI. Berlin: Springer-Verlag; 2012:109–166.
4. Corcoran S.J., Lawrence C., McGuire M.A. The valve of Vieussens: an important cause of difficulty in advancing catheters into the cardiac veins. J Cardiovasc Electrophysiol. 1999;10:804–808.
5. Hansky B., Lamp B., Minami K. et al. Coronary vein balloon angioplasty for left ventricular pacemaker lead implantation. J Am Coll Cardiol. 2002;40:2144–2149.
6. Hansky B., Schulte-Eistrup S., Vogt J. et al. Lead selection and implantation technique for biventricular pacing. Eur Heart J Suppl. 2004;6:D112–D116.
7. Lachman N., Syed F.F., Habib A. et al. Correlative anatomy for the electrophysiologist. II. Cardiac ganglia, phrenic nerve, coronary venous system. J Cardiovasc Electrophysiol. 2011;22:104–110.
8. Leon A.R., Delurgio D.B., Mera F. Practical approach to implanting left ventricular pacing leads for cardiac resynchronization. J Cardiovasc Electrophysiol. 2005;16:100–105.
9. Manolis A.S., Kappos K., Koulouris S. et al. Middle cardiac vein pacing avoids phrenic nerve stimulation, offers optimal resynchronization and obviates surgery for epicardial lead placement. Hosp Chron. 2007;2:44–45.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
History
Current Medications
Physical Examination
Hospital and Procedural Course
Focused Clinical Questions and Discussion Points
Question
Discussion
Question
Discussion
FIGURE 11-2
[/not-level-membership-for-cardiovascular-category]
