Gastric Lavage in Hemorrhage and Overdose
PREREQUISITE NURSING KNOWLEDGE
• Gastric lavage is not recommended as a routine procedure in the management of hemorrhage and overdose. Current evidence (Level D*) shows limited improvement in patient outcomes after lavage, and the procedure may contribute to additional complications, including gastric or esophageal perforation, aspiration, laryngospasm, dysrhythmias, hypothermia, fluid and electrolyte abnormalities, and hypoxia.2,3,5,7–10 The risk-benefit ratio of gastric lavage should be considered before the procedure is performed.
• The use of gastric lavage has been found to be of potential benefit in some cases of hemorrhage and overdose. Specific indications for the use of gastric lavage include:
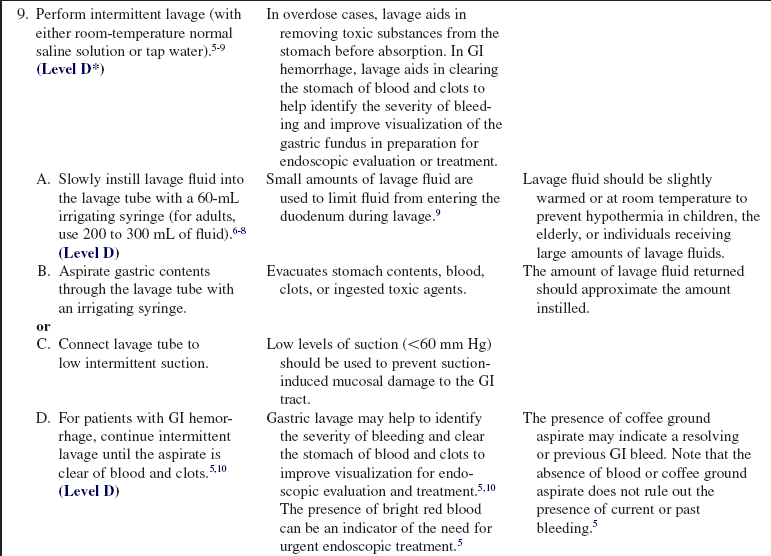
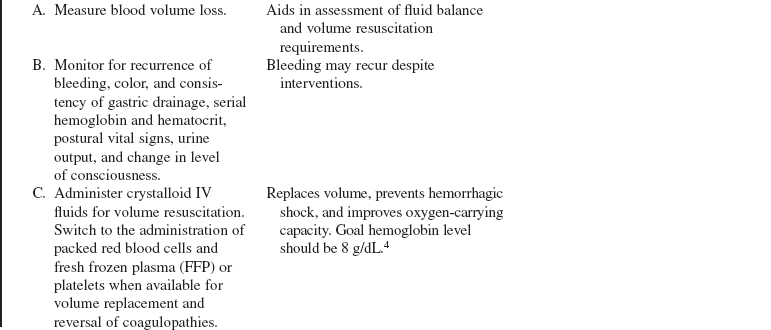
 Gastrointestinal (GI) hemorrhage: The patient who has had GI hemorrhage may present with signs and symptoms of volume loss and a decrease in oxygen-carrying capacity. These symptoms include tachypnea, tachycardia, hypotension, orthostatic changes, decreased hemodynamic filling pressures, decreased urine output, pallor, cold and clammy skin, confusion, anxiety, and somnolence. The patient may also show signs of hematemesis, maroon or tarry stools, or hematochezia. Gastric lavage in GI hemorrhage may be helpful in clearing the stomach of blood and clots to facilitate evaluation of the source of bleeding and to improve visualization of the gastric fundus in preparation for endoscopic treatment.5,10 The presence of bright red blood in the aspirate could be an indicator for the need for urgent enodoscopy.5
Gastrointestinal (GI) hemorrhage: The patient who has had GI hemorrhage may present with signs and symptoms of volume loss and a decrease in oxygen-carrying capacity. These symptoms include tachypnea, tachycardia, hypotension, orthostatic changes, decreased hemodynamic filling pressures, decreased urine output, pallor, cold and clammy skin, confusion, anxiety, and somnolence. The patient may also show signs of hematemesis, maroon or tarry stools, or hematochezia. Gastric lavage in GI hemorrhage may be helpful in clearing the stomach of blood and clots to facilitate evaluation of the source of bleeding and to improve visualization of the gastric fundus in preparation for endoscopic treatment.5,10 The presence of bright red blood in the aspirate could be an indicator for the need for urgent enodoscopy.5
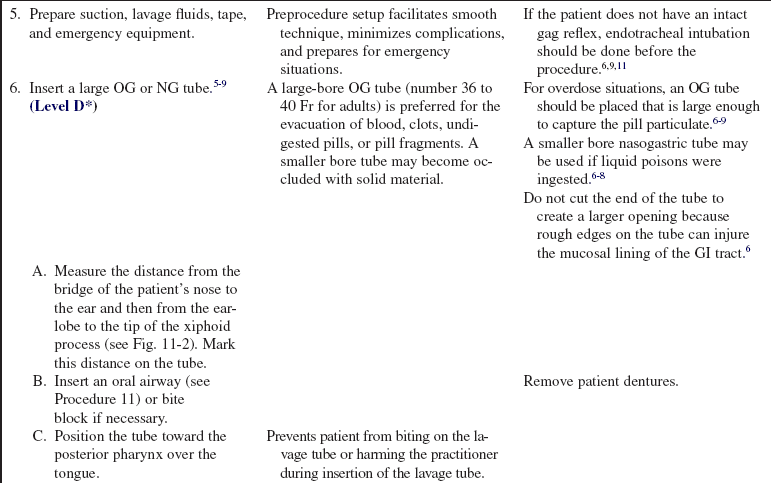
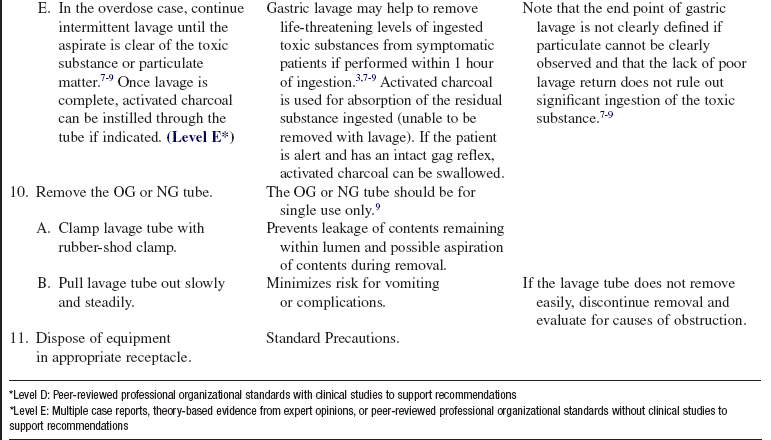
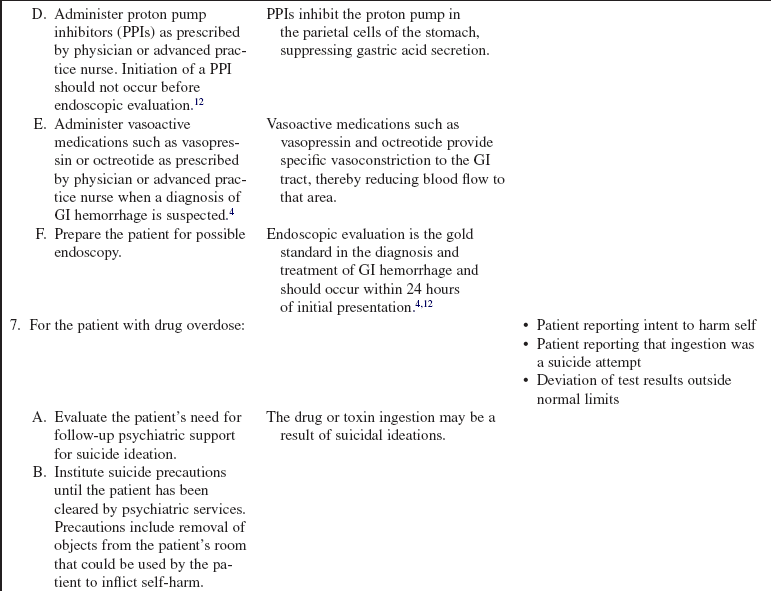
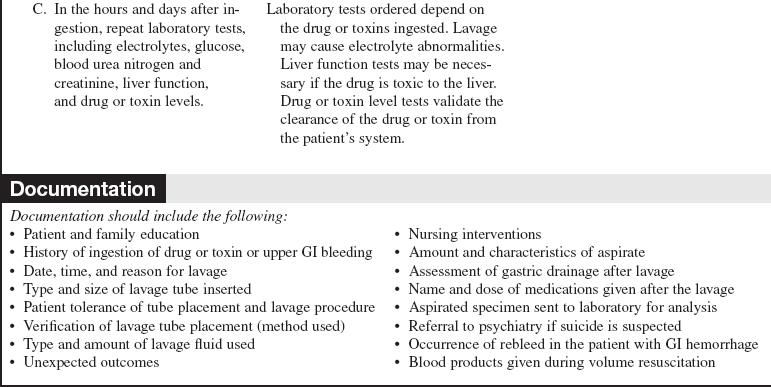
 Overdose: The American Academy of Clinical Toxicology and European Association of Poisons Centres and Clinical Toxicologists do not recommend the use of gastric lavage in the routine management of poisoned patients because of the limited evidence of improved patient outcomes and potential risks of the procedure.3,9 However, in specific poisoning cases, gastric lavage could be of some benefit (Level D*). Indications include if lavage is initiated in symptomatic patients within 1 hour (60 minutes) of ingestion of a potentially life-threatening amount of highly toxic substance, if the substance slows GI motility, or if the substance is a sustained-release medication.3,7–9 Gastric lavage is contraindicated in the use of overdose if the patient has consumed strong corrosives or hydrocarbons (e.g., gasoline, strong acids, or alkali) and if the pills or pill fragments are known to be larger than the opening of the orogastric (OG) tube.6,9 The administration of activated charcoal (AC) has been used in combination with gastric lavage for specific toxins; however, its use must be approached cautiously because the combination of therapies may result in an increased risk for aspiration.7,8 It should be noted that the end point of gastric lavage is not clearly defined if particulate cannot be clearly observed; however, the amount of lavage fluid instilled should approximate the amount of fluid returned.7–9 Gastric lavage after overdose or toxin ingestion has variable efficacy. The amount of toxin or drug recovered depends on variables such as time from ingestion, whether liquid or pills were ingested, specific agent ingested, and size of lavage tube used. Even if lavage is performed close to the time of ingestion, not all the ingested toxin will be recovered and treatment related to effects of the overdose will still be necessary.6–9
Overdose: The American Academy of Clinical Toxicology and European Association of Poisons Centres and Clinical Toxicologists do not recommend the use of gastric lavage in the routine management of poisoned patients because of the limited evidence of improved patient outcomes and potential risks of the procedure.3,9 However, in specific poisoning cases, gastric lavage could be of some benefit (Level D*). Indications include if lavage is initiated in symptomatic patients within 1 hour (60 minutes) of ingestion of a potentially life-threatening amount of highly toxic substance, if the substance slows GI motility, or if the substance is a sustained-release medication.3,7–9 Gastric lavage is contraindicated in the use of overdose if the patient has consumed strong corrosives or hydrocarbons (e.g., gasoline, strong acids, or alkali) and if the pills or pill fragments are known to be larger than the opening of the orogastric (OG) tube.6,9 The administration of activated charcoal (AC) has been used in combination with gastric lavage for specific toxins; however, its use must be approached cautiously because the combination of therapies may result in an increased risk for aspiration.7,8 It should be noted that the end point of gastric lavage is not clearly defined if particulate cannot be clearly observed; however, the amount of lavage fluid instilled should approximate the amount of fluid returned.7–9 Gastric lavage after overdose or toxin ingestion has variable efficacy. The amount of toxin or drug recovered depends on variables such as time from ingestion, whether liquid or pills were ingested, specific agent ingested, and size of lavage tube used. Even if lavage is performed close to the time of ingestion, not all the ingested toxin will be recovered and treatment related to effects of the overdose will still be necessary.6–9
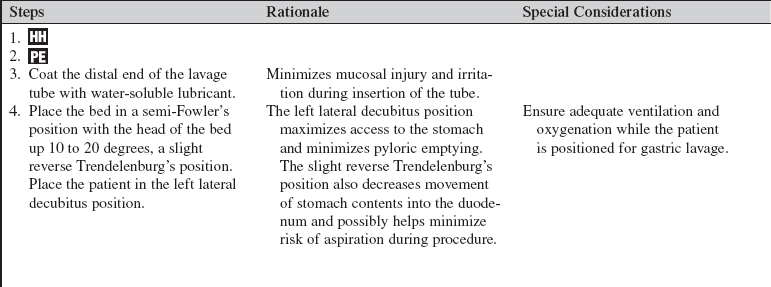
• Nonintubated patients who need gastric lavage must be alert and have adequate pharyngeal and laryngeal reflexes. If the patient has a limited gag reflex or is unable to protect the airway, the patient should be intubated before gastric lavage is performed.6,9,11 All patients undergoing gastric lavage should be positioned in the left lateral decubitus position to assist with passage of the gastric tube.7–9
• Passage of the lavage tube may cause vagal stimulation and precipitate bradydysrhythmias.
• Patients with esophageal varices, coagulopathy, a recent history of upper GI tract surgery, or an underlying pathology should be carefully evaluated for the risk/benefit ratio before gastric lavage is performed.6,9
EQUIPMENT
• Adult lavage tube, external diameter 12 to 13.3 mm9


• Lavage fluid (warm normal saline solution or tap water)
• Measurable container for lavage fluid
• Disposable basin or suction canister for aspirate
• Suction source and connecting tubing
• Rigid pharyngeal suction-tip (Yankauer) catheter
• Endotracheal suction equipment
• Tape for securing nasogastric (NG) or OG tube
Additional equipment, to have available based on patient need, includes the following:
PATIENT AND FAMILY EDUCATION
• Explain the indications and procedure for gastric lavage.  Rationale: Patient and family anxiety may be decreased.
Rationale: Patient and family anxiety may be decreased.
• Evaluate the patient and family understanding of the risks and benefits of gastric lavage.  Rationale: The patient and family may be unaware of the risks and benefits of the procedure.
Rationale: The patient and family may be unaware of the risks and benefits of the procedure.
• Explain the patient’s role in assisting with passage of the tube and lavage of the stomach.  Rationale: The patient’s cooperation during the procedure is elicited.
Rationale: The patient’s cooperation during the procedure is elicited.
• Explain the purpose of the cardiac monitor, automatic blood pressure cuff, and pulse oximeter.  Rationale: Patient and family anxiety may be decreased.
Rationale: Patient and family anxiety may be decreased.
• Assess the need for family presence during the procedure.  Rationale: Patient and family anxiety may be decreased and patient cooperation during the procedure could potentially be improved.
Rationale: Patient and family anxiety may be decreased and patient cooperation during the procedure could potentially be improved.
• Evaluate patient and family need for information on prevention of accidental ingestion of drugs or toxic agents.  Rationale: The patient and family may be unaware or uninformed that the agent or drug is potentially toxic.
Rationale: The patient and family may be unaware or uninformed that the agent or drug is potentially toxic.
• Evaluate patient and family need for information on emergency treatment for accidental ingestion of drug or toxic agents.  Rationale: Emergency first aid measures may be helpful with some ingestions to decrease potential toxicity or systemic absorption.
Rationale: Emergency first aid measures may be helpful with some ingestions to decrease potential toxicity or systemic absorption.
PATIENT ASSESSMENT AND PREPARATION
Patient Assessment
• Perform baseline cardiovascular and neurologic assessments and assess hemodynamic status, cardiac rhythm, and vital signs.  Rationale: Passage of the lavage tube may cause changes in heart rate, blood pressure, or vagal stimulation, which can precipitate bradydysrhythmias or other electrocardiographic (ECG) changes, including ST elevation.9 In the overdose case, toxic levels of certain classes of drugs can also cause ECG changes.3
Rationale: Passage of the lavage tube may cause changes in heart rate, blood pressure, or vagal stimulation, which can precipitate bradydysrhythmias or other electrocardiographic (ECG) changes, including ST elevation.9 In the overdose case, toxic levels of certain classes of drugs can also cause ECG changes.3
• Perform baseline respiratory assessment and pulse oximetry.  Rationale: Gastric lavage has been shown to cause changes in oxygen saturation, leading to hypoxia. Patients who are unable to protect the airway should be intubated before gastric lavage.
Rationale: Gastric lavage has been shown to cause changes in oxygen saturation, leading to hypoxia. Patients who are unable to protect the airway should be intubated before gastric lavage.
• Signs and symptoms of major blood loss are as follows:




 Decreased hemodynamic filling pressures
Decreased hemodynamic filling pressures

 Changes in mental status or somnolence
Changes in mental status or somnolence



 Rationale: Esophageal or gastric varices can cause significant blood loss. The clinical presentation is dependent on amount of blood lost.
Rationale: Esophageal or gastric varices can cause significant blood loss. The clinical presentation is dependent on amount of blood lost.
• Evaluate the patient for a history of esophageal varices, recent GI surgery, coagulopathy, or underlying pathology.  Rationale: Varices, recent surgery, coagulopathies, or other contraindications may predispose the patient to complications during lavage tube insertion.
Rationale: Varices, recent surgery, coagulopathies, or other contraindications may predispose the patient to complications during lavage tube insertion.
• Obtain baseline coagulation studies, hematocrit and hemoglobin values, basic metabolic panel, renal and liver function tests, and blood type.  Rationale: Baseline information is provided so that treatment can be determined and progress can be more accurately monitored.
Rationale: Baseline information is provided so that treatment can be determined and progress can be more accurately monitored.
• Serum toxicology screen, urinalysis, urine toxicology screen, and anion gap (overdose case) are other laboratory tests that also may be monitored.  Rationale: Baseline information for diagnosis is provided so that intervention can be made appropriately and patient progress can be more accurately monitored.3
Rationale: Baseline information for diagnosis is provided so that intervention can be made appropriately and patient progress can be more accurately monitored.3
• Obtain arterial blood gas (ABG) values.  Rationale: Overdose victims with hypoventilation and patients with GI hemorrhage with significant blood loss or comorbid disease are at risk for hypoxia, hypercapnea, and acid-base disorders.
Rationale: Overdose victims with hypoventilation and patients with GI hemorrhage with significant blood loss or comorbid disease are at risk for hypoxia, hypercapnea, and acid-base disorders.
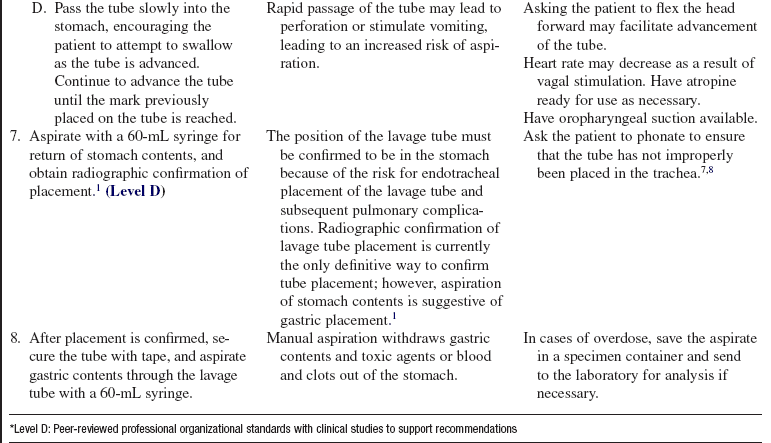
• Assess adequacy of gag reflex.  Rationale: Lack of an adequate gag reflex indicates the need for endotracheal intubation before lavage begins.6,9,11
Rationale: Lack of an adequate gag reflex indicates the need for endotracheal intubation before lavage begins.6,9,11
• Assess the type of drugs or toxic substances ingested, quantity ingested, and time since ingestion. Use of common toxidromes (classifications of the signs and symptoms that develop with poisoning) can help to identify unknown ingested substances (for the overdose case).3  Rationale: Certain substances may require neutralization before tube evacuation is attempted. A poison control center should be contacted if the practitioner is unsure that lavage is indicated. Side effects can be anticipated if the drugs or toxins that were swallowed and the quantity are known.
Rationale: Certain substances may require neutralization before tube evacuation is attempted. A poison control center should be contacted if the practitioner is unsure that lavage is indicated. Side effects can be anticipated if the drugs or toxins that were swallowed and the quantity are known.
• Perform careful skin assessment (overdose case).  Rationale: Assessment may give evidence regarding toxin ingested because various drugs can cause cutaneous changes. Changes to look for include diaphoresis, bullae, acneiform rash, flushed appearance, and cyanosis.
Rationale: Assessment may give evidence regarding toxin ingested because various drugs can cause cutaneous changes. Changes to look for include diaphoresis, bullae, acneiform rash, flushed appearance, and cyanosis.
• Assess any odors present (overdose case).  Rationale: Some toxins have a distinctive odor, which can aid in identification of substance ingested.
Rationale: Some toxins have a distinctive odor, which can aid in identification of substance ingested.
• Perform a 12-lead ECG and continuous cardiac monitoring.  Rationale: In an overdose case, the drug or toxin ingested may be cardiotoxic. For the patient with a GI hemorrhage, comorbid disease states may increase risk for tissue hypoxia and ischemia.
Rationale: In an overdose case, the drug or toxin ingested may be cardiotoxic. For the patient with a GI hemorrhage, comorbid disease states may increase risk for tissue hypoxia and ischemia.
Patient Preparation
• Ensure that the patient understands preprocedural teachings. Answer questions as they arise, and reinforce information as needed.  Rationale: Understanding of previously taught information is evaluated and reinforced.
Rationale: Understanding of previously taught information is evaluated and reinforced.
• Place the patient on a cardiac monitor, automatic blood pressure cuff, and pulse oximeter. Set up oropharyngeal suction.  Rationale: This action allows for close cardiovascular and respiratory system monitoring during the procedure and ensures suction is available for the procedure.
Rationale: This action allows for close cardiovascular and respiratory system monitoring during the procedure and ensures suction is available for the procedure.
• Establish and maintain intravenous (IV) access. For the patient with GI hemorrhage, place a minimum of two large-bore IVs or provide central access.  Rationale: IV access is necessary for emergency IV medication administration and volume resuscitation in the case of GI hemorrhage.5
Rationale: IV access is necessary for emergency IV medication administration and volume resuscitation in the case of GI hemorrhage.5
• Position patient in left lateral decubitus position.7,8  Rationale: This position facilitates passage of the tube into the stomach. The left lateral position is the position of choice to prevent aspiration if the patient should vomit.
Rationale: This position facilitates passage of the tube into the stomach. The left lateral position is the position of choice to prevent aspiration if the patient should vomit.
• Apply oxygen via nasal prongs or mask as needed. Continue to evaluate the patient for possible need of airway intubation.  Rationale: Supplemental oxygen may optimize the patient’s oxygen saturation.
Rationale: Supplemental oxygen may optimize the patient’s oxygen saturation.
References
![]() 1. American Association of Critical-Care Nurses, AACN practice alert. verification of feeding tube placement. www.aacn.org/WD/Practice/Docs/PracticeAlerts/Verification_of_Feeding_Tube_Placement_05-2005.pdf, 2005 [retrieved April 26, 2009 from].
1. American Association of Critical-Care Nurses, AACN practice alert. verification of feeding tube placement. www.aacn.org/WD/Practice/Docs/PracticeAlerts/Verification_of_Feeding_Tube_Placement_05-2005.pdf, 2005 [retrieved April 26, 2009 from].
2. Caravati, EM, Erdman, AR, Scharman, EJ, et al, Long-acting anticoagulant rodenticide poisoning. an -evidence-based consensus guideline for out-of hospital management. Clin Toxicol. 2007; 45(1):1–22.
3. Criddle, LM. An overview of pediatric poisonings. AACN Adv Crit Care. 2007; 18(2):109–118.
4. Garcia-Tsao G, Sanyal, AJ, Grace, ND, et al, Practice -guidelines. prevention and management of gatroesophageal varices and variceal hemorrhage in cirrhosis. Am J -Gastroenterol. 2007; 102(9):2086–2102.
5. Gralnek, IM, Barkun, AN, Bardou, M. Management of acute bleeding from a peptic ulcer. N Engl J Med. 2008; 359(9):928–937.
6. Greene, S, Harris, C, Singer, J. Gastrointestinal decontamination of the poisoned patient. Pediatr Emerg Care. 2008; 24(3):176–189.
![]() 7. Heard, K. Gastrointestinal decontamination. Med Clin North Am. 2005; 89(6):1067–1078.
7. Heard, K. Gastrointestinal decontamination. Med Clin North Am. 2005; 89(6):1067–1078.
8. Heard, K. The changing indications of gastrointestinal decontamination in poisonings. Clin Lab Med. 2006; 26(1):1–12.
![]() 9. Kulig, K, Position paper. gastric lavageAmerican Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol. 2004; 42(7):933–943.
9. Kulig, K, Position paper. gastric lavageAmerican Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. J Toxicol Clin Toxicol. 2004; 42(7):933–943.
![]() 10. Lee, SD, Kearney, DJ. A randomized controlled trial of gastric lavage prior to endoscopy for acute upper gastrointestinal bleeding. J Clin Gastroenterol. 2004; 38(10):861–865.
10. Lee, SD, Kearney, DJ. A randomized controlled trial of gastric lavage prior to endoscopy for acute upper gastrointestinal bleeding. J Clin Gastroenterol. 2004; 38(10):861–865.
11. Madden, M. Responding to pediatric poisoning. Nursing. 2008; 52–55. [August].
12. Palmer, K, Nairn, M, Management of acute gastrointestinal blood loss. summary of SIGN guidelines. BMJ. 2008; 337(a1832):928–933.
Li, Y, Tse, ML, Gawarammana, I, et al. Systematic review -of controlled clinical trials of gastric lavage in acute -organophosphorus pesticide poisoning. Clin Toxicol. 2009; 47(3):179–192.
Larkin, GL, Claassen, C. Trends in emergency department use of gastric lavage for poisoning events in the United States, 1993-2003. Clin Toxicol. 2007; 45(2):164–168.
Scottish Intercollegiate Guidelines Network, Management of acute upper and lower gastrointestinal bleeding. a national clinical guideline. www.sign.ac.uk/guidelines/fulltext/105/index.html, 2008 [retrieved April, 26, 2009 from].
