 CombitubeCombitube Insertion and Removal
CombitubeCombitube Insertion and Removal
PREREQUISITE NURSING KNOWLEDGE
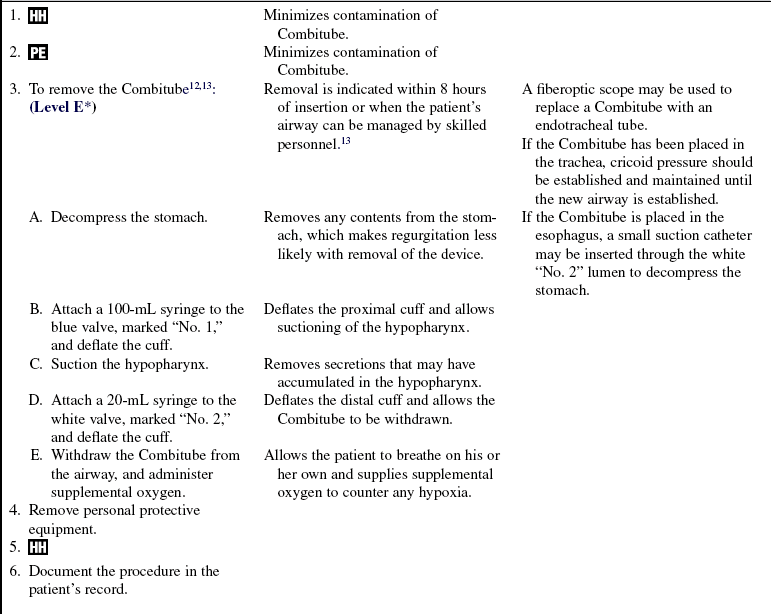
• Anatomy and physiology of the upper airway should be understood.
• The Combitube does not require direct visualization of the airway for insertion and is inserted in a “blind” fashion, as an adjunct when endotracheal intubation attempts fail or trauma makes visualization of the airway difficult.1,8 The Combitube (Fig. 1-1) is available in two sizes, determined by patient height.12
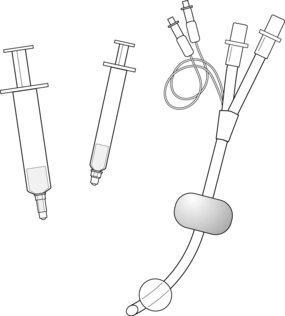
Figure 1-1 Components of the Combitube.
 The 37F size is used for patients 48 to 66 inches tall (122 to 168 cm).
The 37F size is used for patients 48 to 66 inches tall (122 to 168 cm).
 Either size 37F or size 41F is applicable in patients 60 to 66 inches tall (152 to 168 cm).12
Either size 37F or size 41F is applicable in patients 60 to 66 inches tall (152 to 168 cm).12
• For patients greater than or equal to 66 inches (168 cm), the 41F size should be used.
• The Combitube has a unique design that includes:
 A double-lumen, semirigid airway
A double-lumen, semirigid airway
 Blue lumen opening to the perforations between the cuffs
Blue lumen opening to the perforations between the cuffs








• The correct placement of a Combitube in the airway is as follows:
 Esophageal insertion (Figs. 1-2 and 1-3), in which the distal cuff occludes the esophagus and the proximal balloon occludes the hypopharynx, allows ventilation via the blue lumen.
Esophageal insertion (Figs. 1-2 and 1-3), in which the distal cuff occludes the esophagus and the proximal balloon occludes the hypopharynx, allows ventilation via the blue lumen.
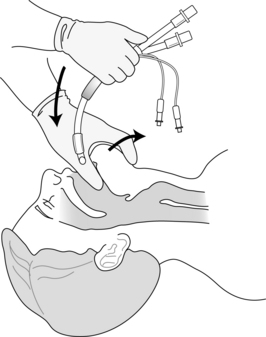
Figure 1-2 Esophageal insertion of a Combitube.
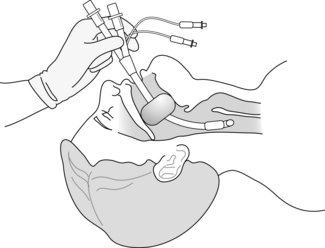
Figure 1-3 Combitube in esophageal position.
• Tracheal insertion (Fig. 1-4), in which the distal cuff occludes the trachea and the proximal balloon occludes the hypopharynx, allows ventilation through the white lumen.

Figure 1-4 Combitube in tracheal position.
• Before the insertion of a Combitube, adequate ventilation of an unconscious patient with a mouth-to-mask or a bag-valve-mask device is necessary.
• Use of the Combitube is contraindicated for airway management8,12 in the following cases:
 Patients with an intact gag reflex
Patients with an intact gag reflex
 Patients with known esophageal disease
Patients with known esophageal disease
 Patients who have ingested caustic substances
Patients who have ingested caustic substances
 Patients with a known or suspected foreign body in the hypopharynx
Patients with a known or suspected foreign body in the hypopharynx

• The Combitube contains latex and may cause an allergic reaction in patients or in personnel who handle the device with a sensitivity to latex.12
• The Combitube is supplied either in a complete kit (with all of the necessary components for insertion), in soft or rigid packaging, or as a single individual device (without any of the necessary components for insertion). If the single individual device is used, additional components are necessary for insertion.
• Initial and ongoing training is needed to maximize insertion success and minimize complications.7
• Medications delivered via endotracheal tube cannot be used with a Combitube in the esophageal position. Medications may not reach the alveolar surfaces of the lung for absorption.
EQUIPMENT
• Combitube, of the appropriate size for the patient’s height
• Large (100-mL) Luer-tip syringe
• Small (20-mL) Luer-tip syringe
• Mouth-to-mask or self-inflating manual resuscitation bag-valve-mask device and mask attached to a high-flow oxygen source
• Gloves, mask, gown, and eye protection
• Suction equipment (suction canister with control head, tracheal suction catheters, Yankauer suction tip)
 Rationale: This information assists the family in understanding why the procedure is necessary and decreases family anxiety.
Rationale: This information assists the family in understanding why the procedure is necessary and decreases family anxiety.PATIENT ASSESSMENT AND PREPARATION
Patient Assessment
• Assess level of consciousness and responsiveness.  Rationale: In an emergency situation, the Combitube should be inserted only into a patient who is profoundly unconscious, unresponsive, and unable to maintain adequate ventilation. Administration of neuromuscular blocking agents and sedation may be needed to ensure that the patient’s gag reflex does not return while the Combitube is in place.9,13
Rationale: In an emergency situation, the Combitube should be inserted only into a patient who is profoundly unconscious, unresponsive, and unable to maintain adequate ventilation. Administration of neuromuscular blocking agents and sedation may be needed to ensure that the patient’s gag reflex does not return while the Combitube is in place.9,13
• Assess history and patient information for possibility of esophageal disease or caustic substance ingestion.  Rationale: A Combitube is contraindicated in patients with these conditions.8
Rationale: A Combitube is contraindicated in patients with these conditions.8
• Assess patient’s height.  Rationale: This assessment allows the selection of an appropriately sized Combitube.13
Rationale: This assessment allows the selection of an appropriately sized Combitube.13
• Assess risk for hypertensive bleeding and take precautions if increased catecholamine stress response is likely.  Rationale: Combitube insertion may cause pronounced catecholamine response.5,10
Rationale: Combitube insertion may cause pronounced catecholamine response.5,10
Patient Preparation
• Verify correct patient with two identifiers.  Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
Rationale: Prior to performing a procedure, the nurse should ensure the correct identification of the patient for the intended intervention.
• Ensure adequate ventilation and oxygenation with either a mouth-to-mask or a self-inflating manual resuscitation bag-valve-mask device.  Rationale: The patient is nonresponsive and unable to maintain adequate ventilation without assisted ventilation before the Combitube insertion.
Rationale: The patient is nonresponsive and unable to maintain adequate ventilation without assisted ventilation before the Combitube insertion.
• Ensure that the suction equipment is assembled and in working order.  Rationale: The patient may regurgitate during insertion or while the Combitube is in place and need oropharyngeal or tracheal suctioning or both.
Rationale: The patient may regurgitate during insertion or while the Combitube is in place and need oropharyngeal or tracheal suctioning or both.
• Perform a pre-procedure verification and time out, if non-emergent.  Rationale: Ensures patient safety.
Rationale: Ensures patient safety.
References
1. American Heart Association. ACLS Resource Text (ACLS). Dallas: AHA; 2008.
2. Calkins, T, et al. Success and complication rates with -prehospital placement of an esophageal-tracheal Combitube as a rescue airway. Prehosp Disaster Med. 2006; 21(2 Suppl 2):97–100.
![]() 3. Frass, M, Combitube retrieved June 22, 2009. Internet J Anesthesiol. 2001; 5(2). www.ispub.com
3. Frass, M, Combitube retrieved June 22, 2009. Internet J Anesthesiol. 2001; 5(2). www.ispub.com
![]() 4. Frass, M, et al. Evaluation of esophageal Combitube in -cardiopulmonary resuscitation. Crit Care Med. 1987; 15:609–611.
4. Frass, M, et al. Evaluation of esophageal Combitube in -cardiopulmonary resuscitation. Crit Care Med. 1987; 15:609–611.
5. Kayhan, D, et al, Which is responsible for hemodynamic response due to laryngoscopy and endotracheal intubation. Eur J -Anaesthesiol. Catecholamines, vasopression or angiotensin. 2005; 22(10):780–785.
![]() 6. Keller, C, et al. The influence of cuff volume and anatomic location on pharyngeal, esophageal, and tracheal mucosal pressures with the esophageal tracheal Combitube. Anesthesiology. 2002; 96:1074–1077.
6. Keller, C, et al. The influence of cuff volume and anatomic location on pharyngeal, esophageal, and tracheal mucosal pressures with the esophageal tracheal Combitube. Anesthesiology. 2002; 96:1074–1077.
7. Kory, P, et al, Initial airway management skills of senior residents. Simulation training compared with traditional training. Chest. 2007; 132(6):1927–1931.
8. Lavery, G, McCloskey, B, et al. The difficult airway in adult critical care. Crit Care Med. 2008; 39(7):2163–2173.
9. Mace, SE, Challenges and advantages in intubation. Rapid sequence intubation. Emerg Med Clin North Am. 2008; 4(26):1043–1068.
![]() 10. Oczenski, W, et al. Hemodynamic and catecholamine stress responses to insertion of the Combitube, laryngeal mask airway, and tracheal intubation. Anesth Analg. 1999; 88(6):1389–1394.
10. Oczenski, W, et al. Hemodynamic and catecholamine stress responses to insertion of the Combitube, laryngeal mask airway, and tracheal intubation. Anesth Analg. 1999; 88(6):1389–1394.
11. Rich, J, Thierbach, A, Frass, M. The Combitube, self-inflating bulb, and colorimetric carbon dioxide detector to advance airway management in the first echelon of the battlefield. Mil Med. 2006; 171(5):389–395.
12. Tyco, Hare. Combitube, Mansfi eld, MA, 2005,Tyco. www.nellcor.com/Serv/Manuals.aspx?ID=259 www.nellcor.com/_catalog/pdf/sns/dfu/10000643b_dfu_combitube.pdf, June 19, 2009. [Text available at. Linked from, retrieved].
![]() 13. Tyco Healthcare, Combitube quick guide Mansfield, MA, 2000. Tyco. www.nellcor.com/prod/Product.aspx?S1=AIR&S2=&id=259 Text available at. www.nellcor.com/_Catalog/PDF/Product/Combitube%20QRG.pdf, June 19, 2009 [Linked from, retrieved].
13. Tyco Healthcare, Combitube quick guide Mansfield, MA, 2000. Tyco. www.nellcor.com/prod/Product.aspx?S1=AIR&S2=&id=259 Text available at. www.nellcor.com/_Catalog/PDF/Product/Combitube%20QRG.pdf, June 19, 2009 [Linked from, retrieved].
14. Vezina, M, et al. Complications associated with esophageal-tracheal Combitube in the pre-hospital setting. Can J Anaesth. 2007; 54(2):124–128.
Agro, F, et al, Current status of the Combitube. a review of the literature. J Clin Anesth 2002; 14:307–314.
Foley, LJ, Ochroch EA. Bridges to establish an emergency -airway and alternate intubating techniques. Crit Care Clin. 2000; 16:429–444.
Gaitini, LA, Vaida, SJ, Agro, F. The esophageal-tracheal -Combitube. Anesthesiol Clin North Am. 2002; 20:893–906.
Idris, AH, Gabrielli, A. Advances in airway management. Emerg Med Clin North Am. 2002; 20:843–857.
