Procedure 1 Closed Cervical Skeletal Tong Placement and Reduction Techniques
Indications
 Subaxial cervical fractures with malalignment
Subaxial cervical fractures with malalignment
 Unilateral and bilateral subaxial cervical facet dislocations
Unilateral and bilateral subaxial cervical facet dislocations
 Displaced odontoid fractures, selected types of hangman’s fractures, and C1-2 rotary subluxations
Displaced odontoid fractures, selected types of hangman’s fractures, and C1-2 rotary subluxations
Controversies
• Magnetic resonance imaging (MRI) before closed reduction of dislocated facets, to exclude an associated disk herniation, is advocated by some.
• For awake, alert patients, closed reduction may be attempted without MRI. If closed reduction fails, MRI should be obtained before operative reduction under general anesthesia.
Examination/Imaging



Surgical Anatomy
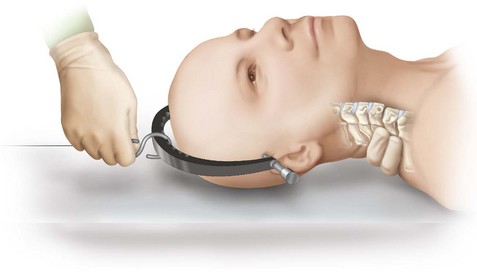
 Correct pin placement site is 1 cm above the pinna, in line with the external auditory meatus and below the equator of the skull (Figures 1-2 and 1-3).
Correct pin placement site is 1 cm above the pinna, in line with the external auditory meatus and below the equator of the skull (Figures 1-2 and 1-3).




Portals/Exposures
• The skin is prepped with a povidone-iodine solution.
• Shaving or skin incisions are not necessary with the use of tapered Gardner-Wells pins. Hair, however, can get wrapped around the pin during insertion. Thoroughly soaking the area with the preparation solution facilitates parting long hair in the area and helps prevent this.
• Local anesthetic is used to infiltrate the skin and down to the skull periosteum.
Procedure
Step 1
 The pins are angled upward slightly and simultaneously tightened until the spring-loaded force indicator (found on one of the two pins) protrudes 1 mm above the flat surface of the pinhead (Figure 1-4).
The pins are angled upward slightly and simultaneously tightened until the spring-loaded force indicator (found on one of the two pins) protrudes 1 mm above the flat surface of the pinhead (Figure 1-4).

Step 2
 An initial weight of 10 lb is applied.
An initial weight of 10 lb is applied.
 The neurologic examination is repeated and a lateral radiograph is taken.
The neurologic examination is repeated and a lateral radiograph is taken.
Step 3
 Weights are increased at 5- to 10-lb increments at intervals of 20 to 30 minutes to overcome muscle spasm and to obtain a soft tissue creep effect.
Weights are increased at 5- to 10-lb increments at intervals of 20 to 30 minutes to overcome muscle spasm and to obtain a soft tissue creep effect.
 Serial neurologic examinations and radiographs are obtained after each increase in weight.
Serial neurologic examinations and radiographs are obtained after each increase in weight.
Step 3 Pearls


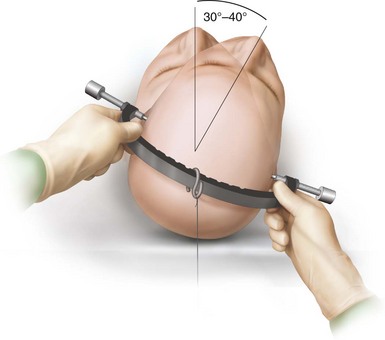
Step 4: Reduction of Unilateral Facet Dislocation
 Manipulation may assist in the final reduction of dislocated facets.
Manipulation may assist in the final reduction of dislocated facets.
 An axial load is applied to the normal facet while the head is rotated 30 to 40 degrees past midline in the direction of the dislocated facet (Figure 1-7).
An axial load is applied to the normal facet while the head is rotated 30 to 40 degrees past midline in the direction of the dislocated facet (Figure 1-7).
 Stop the reduction once resistance is felt, and verify the reduction radiographically.
Stop the reduction once resistance is felt, and verify the reduction radiographically.


Postoperative Care and Expected Outcomes


Cotler HB, Miller LS, DeLucia FA, Cotler JM, Davne SH. Closed reduction of cervical spine dislocations. Clin Orthop Rel Res. 1987;214:185-199.
Cotler JM, Herbison GJ, Nasuti JF, et al. Closed reduction of traumatic cervical spine dislocation using traction weights to 140 pounds. Spine. 1993;18:386-390.
Grauer JN, Vaccaro AR, Lee JY, et al. The timing and influence of MRI on the management of patients with cervical facet dislocations remains highly variable: a survey of members of the Spine Trauma Study Group. J Spinal Disord Tech. 2009;22:96-99.
Hadley MN. Initial closed reduction of cervical spine fracture-dislocation injuries. Neurosurgery. 2002;50:S44-S50.
Littleton K, Curcin A, Novak V, Belkoff S. Insertion force measurement of cervical traction tongs: a biomechanical study. J Orthop Trauma. 2000;14:505-508.
Vaccaro AR, Falatyn SP, Flanders AE, et al. Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine. 1998;24:1210-1217.
Vital J, Gille O, Sénégas J, Pointillart V. Reduction technique for uniarticular and biarticular dislocations of the lower cervical spine. Spine. 1998;23:949-954.


