Chapter 3 History of Spine Biomechanics
Preclassical Antiquity
The oldest known documents related to spine biomechanics were found in ancient Egypt and India. The Edwin Smith Papyrus—named after the American archeologist who purchased the scroll in 1862—is the only surviving copy of a portion of an Ancient Egyptian surgical text.1 The author is unknown, but postulated to be Imhotep, the well-known physician to the pharaoh. The surviving copy was scribed in 1700 bce, but the ideas represented date further back to at least the Egyptian Old Kingdom (2600–2200 bce).2,3 It contains the first reference to the concept of the spine as a bony column, termed the “djet” column.4 Among the 48 case presentations of trauma, 6 were cases of spine trauma. Not only does the papyrus contain descriptions of the devastating neurologic consequences of high cervical traumatic injury to the spinal cord, but it also details the first classification of spine trauma. Sehem represents vertebral axial failure (likely including both compression and burst fracture), whereas wenekh represents dislocation.3,5,6 Although there is evidence that the Egyptians understood the principle of reduction and immobilization for long bone fractures, they did not advocate treating spinal fractures due to the poor prognosis associated with them.
The oldest Indian reference available for spinal biomechanics is an ancient Hindu mythologic epic, Srimad Bhagwat Mahapuranam, written between 3500 bce and 1800 bce.7 The epic includes a description of Lord Krishna correcting the hunchback of one of his devotees by manually applying opposing axial forces on the lady’s chin and feet.8
Classical Antiquity
Mythologic Period
Homer’s Iliad contains several references to spinal trauma: “Hector with his sharp spear struck Eioneus on the neck below the well-made helmet of bronze, and loosed his limbs.”9 The Greek word translated into “loosed” or “lysed,” probably forms the basis for the development of the term paralysis.10 Empedocles reported data from his studies of the spine in the fifth century bce. He suggested that the vertebrae were initially unified, forming a rigid spine, and that this solid osseous column subsequently segmented into pieces as a result of movements of the body.11,12
Scientific Period
During the scientific period, people gradually became skeptical of the notion of supernatural influence upon diseases and treatments. Hippocrates, the most important figure of this period, is the first physician to reject prevailing superstitions and beliefs and define disease in terms of natural causes; according to him, disease was due to an imbalance of four main bodily fluids, or humors: yellow bile, black bile, blood, and phlegm.
Hippocrates (460–377 bce)
Hippocrates made a careful study of the anatomy and pathology of the spine,12–14 (Fig. 3-1) separating the spinal vertebrae into three parts. The first part included the vertebrae lying above the level of the clavicle (including C7). The second part included the 12 vertebrae at the chest that articulated with ribs, the third part the 5 vertebrae between the chest and pelvis.13 The sacrum and coccyx were not included as components of the spine by Hippocrates. Hippocrates also described the natural curvature of the cervical and lumbar portions of the spine (although the terms lordosis and kyphosis were not introduced until Galen in second century ce).15 He used the term ithioscoliosis to describe the natural curves of the spine in the sagittal plane.13
Hippocrates classified spinal disorders as follows: (1) kyphosis, including both traumatic and nontraumatic etiologies; (2) scoliosis; (3) burst fractures; (4) vertebral dislocations; and (5) fractures of the spinous processes.13 He cited spinal tuberculosis as the most common cause for kyphosis, noting that the severity of deformity was greater when it occurred before puberty. Hippocrates was the first to relate traumatic spinal deformities to causative force mechanisms. He found that traumatic kyphosis could result from forceful falls on the shoulder or buttock.5 He correlated burst fractures with axial loading of the spine. Ventral vertebral dislocation was often secondary to a large force applied to the back such as a fall from a height or a blow from a heavy object.5 Dorsal dislocations were rare, frequently fatal, and associated with severe abdominal injury.5 Given the spinal architecture, Hippocrates noted the extreme force needed to create a dislocation: “a great thrusting-out and rupture of the articulation of one or more of them does not very often occur, but is rare. Such injuries, indeed, are hard to produce.”13,16 He also noted that dislocations (which he termed inward curvatures vs. outward curvatures in kyphosis) were associated with a poor prognosis: “In such cases, then, retention of urine and faeces is more frequent than in outward curvatures; the feet and lower limbs as a whole more usually lose heat, and these injuries are more generally fatal. Even if they survive, they are more liable to incontinence of urine, and have more weakness and torpor of the legs; while if the incurvation occurs higher up, they have loss of power and complete torpor of the whole body.”13,16 He noted that isolated spinous process fractures did not result in deformity, healed well, and did not result in clinical impairment.
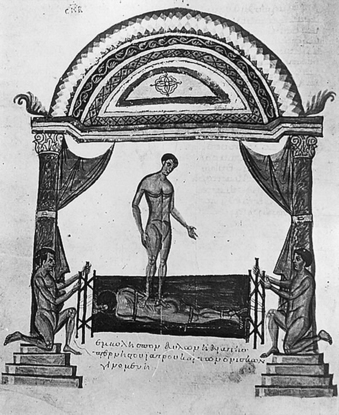
Beyond his keen observations, Hippocrates also devised several innovative therapeutic interventions for spinal disorders, including the Hippocratic board and the Hippocratic ladder. As a first line of intervention, he recommended manual traction of the spine with application of focal pressure using one’s hand or foot over a kyphotic deformity. If this did not work, he recommended use of the Hippocratic board, by which spinal traction could be better obtained using two opposing axial force vectors in combination with manual perpendicular force over the kyphotic deformity (Fig. 3-2). He liked this technique, as he states: “in accordance with nature; for the pressure forces the protruding parts into place, and the extensions according to nature draw asunder the parts that have come together.”13,16
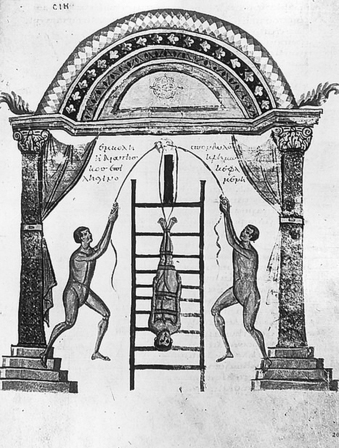
Although he is credited with developing the Hippocratic ladder, his writings reflect less favorably upon this intervention. By this technique, a patient was fixed upside down on a ladder that was connected to a pulley system from which the ladder was raised, suddenly released, and allowed to fall to the ground, and repeated several times (Fig. 3-3). Hippocrates felt it was more difficult to control the direction and magnitude of force with this technique. Perhaps this is why he warned that this technique, which he called “succussion” (shaking), was better at pleasing the mob then correcting a deformity.17
Plato (427–347 bce)
The great philosopher and mathematician, Plato, was founder of the Academy in Athens, the first institution of higher learning in the Western world. He suggested that mathematics, a system of pure ideas, was the best tool for the pursuit of knowledge. Plato’s contributions to mathematics are considered to be the origins and stimulus for the development of the science of mechanics and, consequently, spine biomechanics.18
Aristotle (384–322 bce)
Aristotle provided treatises on many subjects, including physics, metaphysics, poetry, theater, music, politics, ethics, biology, and zoology.16 He should perhaps be considered the first biomechanist. As such, he recorded detailed information regarding the mechanical system of animals in his first book, De Motu Animalium (On the Movement of Animals).18–23 This work provides the first geometric analyses of isolated muscular movements such as flexion and extension.5 He commented on the rotational axes surrounding joints and how one type of motion, such as rotation, could be used to create another type, such as translation.
Aristotle discussed the problems of pushing a boat under various conditions from the standpoint of mechanics, describing, in a primitive form, Newton’s three laws of motion. Aristotle depicted a qualified understanding of the role of the center of gravity in his analyses of gait.23,24 Of note, Aristotle’s findings were purely observational, he did not perform scientific experiments. Even though his work was not directly related to the spine, Aristotle’s work led to the birth of kinesiology and laid further groundwork for spinal biomechanics.19,22
Herophilus of Chalcedon (335–280 bce)
Herophilus of Chalcedon, the world’s first anatomist, dominated the discussions of anatomic studies during this period. Although Herophilus carried out anatomic dissections on human cadavers, he did not comment on spine anatomy and biomechanics in his works. He did, however, make significant contributions to cerebral neuroanatomy and noted the consequences of spinal cord injuries, suggesting that direct surgical intervention on the spinal column should be avoided.11,25
Archimedes (287–212 bce)
Archimedes was a prominent mathematician, physicist, engineer, inventor, and astronomer of this age. He had the greatest influence on the future of spinal biomechanics through his contributions to theoretical mechanics in his work On the Equilibrium of Planes19 He is known for his formulation of the hydrostatic principle (known as Archimedes’ principle) and the development of the Archimedes screw, a cylinder with an internal revolving screw that was built to pump water against gravity. Archimedes described fundamental theorems concerning the center of gravity and laws of leverage.5
Galen of Pergamon (130–200 ce)
In the second century ce, as the Roman Empire rose to prominence, mysticism subsided and scientific thought regained credibility and popularity, albeit under the strict oversight of the Church. Galen (Fig. 3-4) was a physician to the Roman gladiators. More importantly, he made many important discoveries in anatomy and physiology by performing anatomic dissections on animals and extrapolating his findings to humans. Galen’s anatomic studies and interpretations affected medicine for more than a thousand years, until the time of Vesalius. His own work corroborated the findings of Imhotep and Hippocrates on the neurologic sequences of cervical trauma.14,24,26
Galen was the first to determine the reliance of muscular movements on supplying connections from nerves.27 He also demonstrated the neurologic implications following transection of the spinal cord at several levels in live animals. He dealt with spinal tuberculosis as well as an abundance of traumatic injuries to the spine and the spinal cord. He appreciated the structure of the spine in allowing an intersecting balance of neural protection and flexibility for mobility.27 Galen was able to detail the structure of the spine in that the vertebrae were joined ventrally and had articulating components dorsally. He felt that the former allowed for motion and the latter provided greater stability.5 In addition, he was the first to describe the spinal canal which contained the spinal cord—previously termed the “spinal marrow” in the Greek era. He noted that the spinal cord was an extension of the brain, “like a river having its springs in the brain.”27 He also used the Hippocratic board to treat kyphotic deformities, but unlike Hippocrates, advocated surgery in some cases to remove bony fragments impinging on the spine.5,25
Middle Ages (330–1453 ce)
Paulus of Aegina was the last prominent scientist working in the tradition of the Greco-Roman period.5 As the Dark Ages of Europe settled in, religion governed all aspects of life, particularly science. Yet during this same period, Islamic civilization flourished. Major Greco-Roman scientific texts were translated into Persian and Arabic, and many Islamic scientist physicians led the frontier of medical advancement.
Paulus of Aegina (625–690 ce)
The Medical Compendium in Seven Books or Epitomês Iatrikê Biblio Hepta was a medical treatise of seven books written by Paulus of Aegina in the seventh century (Fig. 3-5). He used traction tables to treat spinal deformity and employed a new technique of cauterization with a red hot iron to treat various painful illnesses. Paulus of Aegina was the first physician to perform a successful laminectomy for a spinal fracture with symptomatic neural compression. He recommended the use of orthoses for spinal fractures.25

Avicenna (981–1037 ce)
Avicenna, an Islamic physician, was very interested in the mechanical function of the spine. He studied regional anatomic variations of vertebrae and correlated the different features to their mechanical functions. He described quite accurately the mechanical movements involved in flexion, extension, and lateral bending of the spine. Avicenna studied in detail the mechanics of the craniovertebral junction. He believed that movement at the occiput-C1 joint provides lateral bending, and movement at the occiput-C2 segments provides flexion-extension. Also, during head flexion-extension and lateral bending, C1-2 vertebrae move simultaneously. According to Avicenna, the dens was uniquely developed to protect the high cervical spinal cord and limit motion of C1-2.28
Albucasis (936–1013 ce)
Albucasis, also known as Al-Zahrawi, was a prominent Islamic physician and surgeon. He designed instruments and surgical techniques for treating spinal disorders, including lumbar radiculopathy, low back pain, scoliosis, and spinal dislocations. He developed a procedure for cauterization and described a device for reduction of dislocated vertebrae.29 He classified spinal trauma as complete and incomplete. He observed that a complete dislocation presents itself with abolition of sphincter tone and motor function and that an incomplete trauma causes partial neurologic injury. Cerrahiyetul Haniye, a Turkish treatise written by Serafeddin Sabuncuoglu in the 15th century, describes and illustrates the technical details of Albucasis’s surgery and treatments for spinal diseases.30
Renaissance and Premodern Era
The Renaissance began a new period of scientific exploration unfettered by the restraints of religion. Scientists of this era were able to build on the ideas of the Greco-Roman period thanks to the preservation of texts through Arabic translations. However, seeking to break free from classical traditions, two new trends developed. First, skillful anatomists such as Leonardo Da Vinci (1452–1519) and Andreas Vesalius (1514–1564) rejected the archaic galenic anatomic descriptions of animals and dissected human cadavers in painstaking detail. As Vesalius is known to have stated, it became time to learn from dead bodies rather than dead languages. Second, classical theories were tested under scientific rigor for the first time. Instead of applying traditional treatments without question, doctors developed new practices based on experimentation.31 Simultaneously, during this time, the fields of mathematics, physics, and mechanics gained significant theoretical developments through the work of René Descartes, Robert Hooke, Isaac Newton, and Thomas Young. As a precursor to more detailed spinal biomechanical research in the 20th century, earlier work was conducted in kinesiology and the biomechanics of gait by Giovanni Alfonso Borelli, the Weber brothers, Christian Wilhelm Braune, and Otto Fischer.
Leonardo Da Vinci (1452–1519)
Leonardo Da Vinci (Fig. 3-6) was an intelligent engineer with the skill of a master artist. Da Vinci studied detailed anatomy (Figs. 3-7 to 3-9) using dissections in 10 cadavers, from which he produced over 750 illustrations later published in De Figura Humana. He illustrated spinal anatomy with unprecedented accuracy and detail from the variation of regional vertebrae to the natural curvature of the spine, and he included the correct number of vertebrae. He was particularly interested in the mechanics of human movement and therefore focused on the anatomy of motion—muscles, tendons, bones, ligaments, and joints.




He demonstrated an understanding of the components of force vectors, friction coefficients, and the acceleration of falling objects. He clearly demonstrated an understanding of what was to become Newton s third law.2,32
Andreas Vesalius (1514–1564)
Vesalius rid the study of human anatomy of mythic speculations, which had engulfed it for two millennia. He published De Humani Corporis Fabrica (On the Fabric of the Human Body), an encyclopedic work containing more than 200 anatomic drawings.18,33 Vesalius is credited with being the revolutionary figure of anatomy because the work of Da Vinci remained unpublished and unknown to the medical community for many years.
He termed the spine the “dorsum” (backbone) and confirmed Da Vinci’s descriptions of the spinal column, joints, and foramina. Vesalius only disagreed on the number of sacral vertebrae (six) as opposed to Da Vinci, who believed there was five.34 He was the first to correctly describe the intervertebral disc. He also expounded his view on the mechanics of head movement: “the neck has seven bones…by means of the first of these bones, we move the head directly forward and backward. By the use of the second vertebra (to which a prominent process resembling a canine tooth is attached) we turn the head….”5,34,35 The greatest contribution Vesalius made was to solidify anatomic dissection as a necessary prerequisite to medicine and surgery.
Galileo Galilei (1564–1642)
Galileo is often considered the “first real scientist” because he advocated and practiced the scientific method of hypothesis testing for his experiments.32 Using the mathematical terminology, he founded the basic principles for kinesiology as a science. In Discourses on Two New Sciences (1638), Galileo stated “The mass of animals increase disproportionately to their size, and their bones must consequently also disproportionately increase in girth, adapting to load-bearing rather than mere size,” and later added, “the bending strength of a tubular structure, such as bone, is increased relative to its weight by making it hollow and increasing its diameter.”17,31 Although not directly related to the spine, his work laid early groundwork for mathematical analyses of biomechanical properties of load-bearing bone structures.
René Descartes (1596–1650)
Descartes, a French philosopher, scientist, and mathematician, is often called the founder of modern philosophy. He was not a major contributor in the field of biomechanics, but his thoughts had an indirect influence on the field. In 1675, Descartes wrote Tractatus de Homine et de Formatione Foetus (Treatise on Humans and the Formation of the Fetus). In this treatise, he developed his mechanical view of the universe; movement was the reorganization of matter in a cartesian coordinate system of space. He also equated organisms to God’s machines.32 Aside from inventing the cartesian coordinate system, he is also said to be the founder of analytical geometry. L’Homme was Descartes’ first systematic presentation of physiology.
Giovanni Alfonso Borelli (1608–1679)
Borelli (Fig. 3-10) was a Renaissance physiologist, physicist, and mathematician.36 The Accademia del Cimento (Academy of Experiment), an early scientific society, was founded by Borelli and Marcello Malpighi, a mathematician and naturalist. In this academy, he began his first investigations into the science of animal movement. The collaboration between two authors yielded an abundance of scientific work.18,37

In De Motu Animalium (On the Movements of Animals), one of his most complicated treatises, he investigated in detail the movement of animals. Movement of the musculoskeletal system and internal motions, such as muscle physiology and blood circulation, were also studied.38 Borelli was the first to determine that muscles acted upon joints with short lever arms, debunking Galen’s assumption that muscles acted via long lever arms in order to achieve a biomechanical advantage.2,31
Borelli analyzed the biomechanics of individual components of the spine (Fig. 3-11).39 He described anatomic characteristics that prevent listhesis39 and demonstrated, with modern experimental calculations, the concept of spinal load sharing (Fig. 3-12): “If the spine of a stevedore is bent and supports a load of 120 pounds carried on the neck, the force exerted by nature in the intervertebral discs and in the extensor muscles of the spine is equal to 25,585 pounds. The force exerted by the muscle alone is not less than 6404 pounds. Therefore, the sum of muscular forces which control the fifth lumbar vertebra and a third of the resistance of the intervertebral disc is equal to 826 pounds. The muscular forces are equal to 413 pounds and the forces exerted by the disc are equal to 1239 pounds.”31,38 He explained that strong fibers of the intervertebral disc are much stronger than those in muscle. He suggested that most of the weight of axial loading is carried by the intervertebral discs, with a much smaller portion carried by the spinal musculature.38
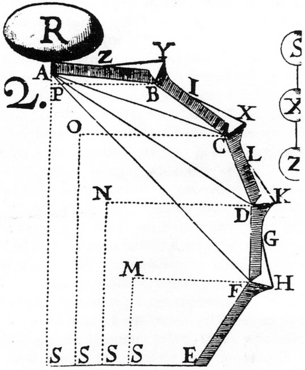
FIGURE 3-11 The spine, muscles, and intervertebral discs were depicted by Borelli, from De Motu Animalium.
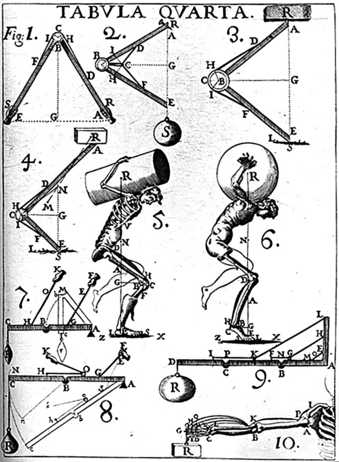
FIGURE 3-12 Illustration by Giovanni Alfonso Borelli analyzing the load-sharing capabilities of the spine.
Borelli was also the first to experimentally demonstrate the human center of gravity as a point between the pelvis and buttocks. He devised a wooden plank resting on a pyramidal fulcrum to conduct his experimental measurements (Fig. 3-13).26,31 Several centuries later, Braune and Fisher40 verified that his assessment was correct. After Borelli, biomechanical studies were sparse until the 19th century.

Robert Hooke (1635–1703)
Hooke went further to describe how solids react under a full range of deforming forces, from zero net sum forces to deforming forces that alter the mechanical properties of the solid. He essentially described the neutral zone, the elastic zone, the plastic zone, and the point of failure.32
Isaac Newton (1642–1727)
The English mathematician and founder of classical mechanics, Isaac Newton, invented complex mathematical and engineering principles. Newton described three laws of motion, now known as Newton’s laws of motion (laws of inertia, momentum, and interaction).32,41 With the introduction of these physical laws, biomechanical mechanisms and structures could be simulated and studied. He was also credited with calculating resultant force vectors from individual component vectors.
Leonard Euler (1707–1783)
The Swiss mathematician Leonard Euler is known for his work in mathematics, astronomy, and physics. He studied columns under compressive loads and found that columns had a point at which they would deform.32,41 This point was related to the height and stiffness of the column. At later points in history, the spine was studied as a Euler column.39
Thomas Young (1773–1829)
Thomas Young studied the human voice and vibration. He developed Young’s modulus, a coefficient that can be calculated to define the relation of stress and strain for a given body. This important concept is employed in contemporary spinal biomechanics to measure the elasticity of both the spine and the spinal constructs.32
Weber Brothers
Three brothers, Ernst Heinrich Weber (1795–1878), Wilhelm Eduard Weber (1804–1891), and Eduard Friedrich Wilhelm Weber (1806–1871), in their publication Die Mechanik der Menschlichen Gehwerkzeuge (Mechanics of the Human Gait), developed the modern concept of locomotion.42 It was assumed that the human torso was kept in erect posture primarily via tension of the ligaments, with little or no muscular exertion. The Weber brothers demonstrated that muscle contraction contributed substantially to posture.43 They also studied the movement of the center of gravity in locomotion.
Christian Wilhelm Braune (1831–1892) and Otto Fischer (1861–1917)
The development of a new three-dimensional mathematical analysis of human gait was published by Christian Wilhelm Braune and Otto Fischer. They described the first plausible theory related to the mechanics of walking and running in Mechanik der Menschlichen Gehwerkzeuge (Mechanics of the Human Walking Apparatus).44 They determined the human center of gravity by suspending frozen human cadavers on thin rods in three perpendicular axes. They observed the center of gravity during locomotion and investigated the forces supplied by the musculature to maintain the center of gravity during locomotion.40
Julius Wolff (1836–1902)
Wolff’s law embodies the fundamental relationships between applied loads and the body’s adaption to such loads. Julius Wolff (Fig. 3-14), a German orthopedic surgeon, studied bony architecture and found that it paralleled mathematically calculated stress trajectories.45 His law states: “Every change in the form and function of a bone, or of function alone, is followed by specific definite change in its internal architecture and equally definite secondary changes in its external configuration, in accordance with mathematical laws.”31,45 In modern spine biomechanics, this law influences spinal construct design in order to maximize fusion rates.

Emergence of Modern Biomechanics in the 20th Century
An increasing interest in athletics, gymnastics education, and World Wars I and II were major contributors to the development of the field of biomechanics in the 20th century. The technologic advances that emerged during this century led to new and greater force applications to the human body via trauma, such as from motor vehicle and plane accidents and civilian injuries from explosions. These new problems rejuvenated interest in spine biomechanics.22
The Human Motor by Jules Amar (1879–1935) was an analysis of the physical and physiologic components of gait and task performance in thousands of disabled veterans in France.46,47 This was the first biomechanical evaluation derived from human force and motion data.
In World War II, high-speed aircraft with emergency ejection seats provided another inspiration for biomechanical research. Multiple biomechanical studies were conducted to test the safe range of compressive loads tolerable at different levels of the spine. The appropriate spinal posture at the time of ejection was determined by Olof Perey in 1945, and the Martin-Baker aircraft company in England in 1944.48 Similar studies were performed by the U.S. Air Force in 1945.48
Detailed research on the intervertebral disc was performed at Massachusetts General Hospital and Massachusetts Institute of Technology.48 Parallel to these studies, at Wayne State University, H. R. Lissner and E. S. Gurdjian investigated the effect of applying axial compression and transverse bending on lumbar disc herniation.48–52
Friedrich Pauwels (Fig. 3-15) (1885–1980) and Nikolai A. Bernshtein (1896–1966) conducted seminal work in musculoskeletal biomechanics.13,53 Russell Plato Schwartz established his myodynamics laboratory in the Department of Surgery of the University of Rochester School of Medicine and Dentistry in 1926. The laboratory focused on gait analysis for shoe design and other biomechanical applications. He developed the recording instrumentation and surgical tools necessary to measure normal and abnormal gait.

The mechanical properties of the cervical vertebra in vitro were studied for the first time by Erland Lysell in Sweden. He inserted small steel balls at each cervical vertebra in the cervical spines of 28 fresh cadavers, and using quantitative stereoradiography, he measured intervertebral motion.31 As an aside, he observed no effect of age on extent of degeneration.54
Advanced studies were performed on the effect of bending moments on the spine. Load-deflection, energy-absorption, and other analyses were performed by Virgin,55 Hirsch,56 Hirsch and Nachemson,57 Hirsch and Schajowicz,58 Hirsch,59 Evans,60,61 Evans and Lissner,49 Higgins,62 Friberg and Hirsch,63 Sylven et al.,64 and Werne.65 Carl Hirsch (Fig. 3-16) (1913–1973), a Swedish orthopaedic surgeon, had substantial influence on the development of biomechanics. His interest centered on the knee, hip, and spine in the 1940s.56 He applied his knowledge and findings to orthopaedic problems. He attracted many visitors and fellows to his laboratory, including Victor Frankel, George Galante, Augustus White, Wilson C. Hayes, and Albert B. Scultz, and many of his fellows went on to establish their own biomechanics laboratories.31

Finite Element Analysis
Finite element analysis (FEA), developed by R. Courant and Hilbert66 in 1943, is a technique originally developed for numerical analysis of complex structural mechanics problems. FEA is based on the idea of building complicated objects from small manageable pieces and is used by engineers in the aerospace industry. Applied to spinal biomechanics, it takes the whole spine and breaks it down into smaller geometric forms at any given level, which can individually be tested and analyzed more easily. Computer programs can then derive composite analyses of discrete finite elements. Using this method, the risk of spinal injury in emergency pilot ejection was investigated for the first time in the second half of 1950s.67 This technique has become popular for biomechanical testing of the spine in recent years due to its cost-effectiveness.
Clinical Studies
High-quality evidence from clinical trials provided a new valuable source of data. New definitions of ‘’stability’’ and associated scoring systems were developed and utilized.68 The column system for spinal stability assessment was first introduced as a two-column system, defined in 1962 by Sir Frank Holdsworth.69 A three-column system, proposed by Francis Denis,70 provided further refinement. For tumor-related instability, a six-column system71 and a cube system for ventral column stability were described.39 These studies exemplify the transition of evidence obtained from the biomechanical laboratory to clinically applicable knowledge.
Goodrich J.T. History of spine surgery in the ancient and medieval worlds. Neurosurg Focus. 2004;16:E2.
Hirt S. What is kinesiology? A historical review. Phys Ther Rev. 1955;35:419-426.
Marketos S.G., Skiadas P. Hippocrates. The father of spine surgery. Spine. 1999;24:1381-1387.
Marketos S.G., Skiadas P.K. Galen. A pioneer of spine research. Spine. 1999;24:2358-2362.
Naderi S., Andalkar N., Benzel E.C. History of spine biomechanics. Part IThe pre-Greco-Roman, Greco-Roman, and medieval roots of spine biomechanics. Neurosurgery. 2007;;60(2):382-390. discussion 390–391
Naderi S., Andalkar N., Benzel E.C. History of spine biomechanics. Part IIFrom the Renaissance to the 20th century. Neurosurgery. 2007;;60(2):392-403. discussion 403–404
1. Apuzzo M.L., Liu C.Y., Sullivan D., et al. Honored guest presentation: surgery of the human cerebrum: a collective modernity. Clin Neurosurg. 2002;49:27-89.
2. Sanan A., Rengachary S.S. The history of spinal biomechanics. Neurosurgery. 1996;39:657-669.
3. Breasted J.H. The Edwin Smith Surgical Papyrus: published in facsimile and hieroglyphic transliteration with translation and commentary in two volumes,. Chicago: University of Chicago Press; 1930.
4. Lang J.K., Kolenda H. First appearance and sense of the term “spinal column” in ancient Egypt: historical vignette. J Neurosurg. 2002;97(Suppl 1):152-155.
5. Naderi S., Andalkar N., Benzel E.C. History of spine biomechanics.Part I. The pre-Greco-Roman, Greco-Roman, and medieval roots of spine biomechanics. Neurosurgery. 2007;;60(2):382-390. discussion 390–391
6. Wilkins R.H. Neurosurgical classics I. Park Ridge: American Association of Neurological Surgeons; 1992. pp 1–5
7. Kostuik J.P., Errico T.J., Gleason T.F., Errico C.C. Spinal stabilization of vertebral column tumors. Spine. 1988;13:250-256.
8. Subramaniam K. Srimand Bhagavatam. Bombay: Bharatiya Vidya Bhavan; 1979.
9. Murray A.T., Wyatt W.F. The Iliad/Homer: Books 1–12 (translation). Cambridge: Harvard University Press; 1999. Vol 2, ed 2
10. Sahlas D.J. Functional neuroanatomy in the pre-Hippocratic era: observations from the Iliad of Homer. Neurosurgery. 2001;48:1352-1357.
11. Acar F., Naderi S., Güvençer M. Herophilus of Chalcedon: a pioneer of neuroscience. Neurosurgery. 2005;56:861-867.
12. Çitak G., Naderi S. History of spine biomechanics. In: Naderi S., editor. Essentials of spine biomechanics [in Turkish]. Izmir: Publications of Spine and Peripheral Nerve Surgery Section of the Turkish Neurosurgical Society; 2004:1-8.
13. Marketos S.G., Skiadas P. Hippocrates: the father of spine surgery. Spine. 1999;24:1381-1387.
14. Wiltse L.L. The history of spinal disorders. In: Frymoyer J.W., editor. The adult spine: principles and practice. Philadelphia: Lippincott-Raven; 1997:3-40.
15. Galen. On the affected parts [translated from the Greek by Siegel RE]. Basel: S. Karger; 1976. p 113
16. Hippocrates. On joints. In: Capps E., Page T.E., Ruse W.H., editors. Hippocrates: the Loeb Classical Library, vol 3. London: W. Heinemann; 1927:200-397.
17. Loeser J.D. History of skeletal traction in the treatment of cervical spine injuries. J Neurosurg. 1970;33:54-59.
18. Martin R.B. A genealogy of biomechanics. http://asb-biomech.or/ history/biomech/. Accessed March 20, 2005
19. Braun G.L. Kinesiology: From Aristotle to the twentieth century. Res Q. 1941;12:164-173.
20. Dugas R. A history of mechanics. New York: Dover Publications; 1988.
21. Fung Y.C. Biomechanics: mechanical properties of living tissues. New York: Springer Verlag; 1993. pp 1–13
22. Hirt S. What is kinesiology? A historical review. Phys Ther Rev. 1955;35:419-426.
23. Rasch P.J. Notes toward a history of kinesiology. I. J Am Osteopath Assoc. 1958;57:572-574.
24. Parts of animals. Movement of animals. Progression of animals (Forster ES, translator). Cambridge: Harvard University Press; 1937. Aristotle
25. Goodrich J.T. History of spine surgery in the ancient and medieval worlds. Neurosurg Focus. 2004;16:E2.
26. Maquet P. Iatrophysics to biomechanics. From Borelli (1608–1679) to Pauwels (1885–1980). J Joint Bone Surg (Br). 1992;74:335-339.
27. Marketos S.G., Skiadas P.K. Galen. A pioneer of spine research. Spine. 1999;24:2358-2362.
28. Naderi S., Acar F., Mertol T., et al. Functional anatomy of the spine by Avicenna in his eleventh century treatise Al-Qanun fi al-Tibb (The Canons of Medicine). Neurosurgery. 2003;52:1449-1454.
29. Albertsone C.D., Naderi S., Benzel E.C. History of spine surgery. In: Benzel E.C., editor. Spine surgery. Techniques, complication avoidance, and management. ed 2. Philadelphia: Elsevier Churchill Livingstone; 2005:1-21.
30. Naderi S., Acar F., Arda M.N. History of spinal disorders and Cerrahiyetul Haniye (Imperial Surgery): a review of a Turkish treatise written by Serefeddin Sabuncuoglu in the 15th century. Historical vignette. J Neurosurg. 2002;96(Suppl 3):352-356.
31. Naderi S., Andalkar N., Benzel E.C. History of spine biomechanics. Part II. From the Renaissance to the 20th century. Neurosurgery. 2007;;60(2):392-403. discussion 403–404
32. Gribbin J. Science. A history. London: Penguin Books; 2003. pp 1453–2001
33. Vesalius A. De Humani Corporis Fabrica Libri Septem. Basel: Ex officina Ioannis Oporini; 1543.
34. Benini A., Bonar S. Andreas Vesalius: 1514–1564. Spine. 21(11), 1996. 1393–1399
35. Saunders JBdeCM, O’Malley C.D. The illustrations from the works of Andreas Vesalius of Brussels with annotations and translations, a discussion of the plates and their background, authorship and influence, and a biographical sketch of Vesalius. Cleveland and New York: World Publishing Co; 1950.
36. Provencher M.T., Abdu W.A. Giovanni Alfonso Borelli: “father of spinal biomechanics.”. Spine. 2000;25:131-136.
37. Mow V.C., Huiskes R. A brief history of science, and orthopaedic biomechanics. In: Mow V.C., Huiskes R., editors. Basic Orthopaedic Biomechanics and Mechanobiology. Philadelphia: Lippincott Williams and Wilkins; 2005:1-28.
38. Borelli G.A. On the movement of animals. Berlin: Springer-Verlag; 1989.
39. Benzel E.C. Biomechanics of spine stabilization. Park Ridge: American Association of Neurological Surgeons; 2001.
40. Braune W., Fischer O. On the center of gravity of the human body [in German]. Berlin: Springer-Verlag; 1988.
41. Richardson J.A. History of biomechanics and kinesiology. www.usd.edu/ jarichar/Hist.html. Accessed March 25, 2005
42. Weber W., Weber E. Mechanics of the human walking apparatus [in German]. Böttingen: Dietrich; 1836.
43. Weber E.H. Anatomical and physiological tests on some systems of human spine mechanism [in German]. Arch Anat Physiol. 1827;1:240-271.
44. Braune W., Fischer O. Human gait: trial on loaded and unloaded humans [in German]. Saech Gesellsch Wissensch. 1895;21:153-322.
45. Wolff J. The law of bone remodeling [in German]. Berlin: A Hirschwald; 1892.
46. Amar J. The human motor, or the scientific foundation of labour and industry. New York: G. Routledge; 1920.
47. Drewlinger D.M. Biomechanics. Emergence of an academic discipline in the United States. Denton: Texas Woman’s University; 1996. (Dissertation
48. Crawford H. Survivable impact forces on human body constrained by full body harness. 2003. Report HSL/2003/09 prepared for health and safety executive www.hse.gov.uk/research/hsl_pdf/2003/hsl03-09.pdf.
49. Evans F.G., Lissner H.R. Biomechanical studies on the lumbar spine and pelvis. J Bone Joint Surg (Am). 1959;41:278-290.
50. Gurdjian E.S., Lissner H.R. Mechanism of head injury as studied by the cathode ray oscilloscope: preliminary report. J Neurosurg. 1944;1:393-399.
51. Gurdjian E.S., Webster J.E., Lissner H.R. Studies on skull fracture, with particular reference to engineering factors. Am J Surg. 1949;78:736-742. 749–751
52. Hardy W.G., Lissner H.R., Webster J.E., et al. Repeated loading tests of the lumbar spine; a preliminary report. Surg Forum. 1958;9:690-695.
53. Pauwels F. A collective treatise on functional anatomy of locomotor apparatus [in German]. Berlin: Springer-Verlag; 1965.
54. Lysell E. Motion in the cervical spine. An experimental study on autopsy specimens. Acta Orthop Scand Suppl. 1969;123:1.
55. Virgin W.J. Experimental investigations into the physical properties of the intervertebral disc. J Bone Joint Surg (Br). 1951;33:607-611.
56. Hirsch C. The reaction of intervertebral discs to compression forces. J Bone Joint Surg (Am). 1955;37A:1188-1196.
57. Hirsch C., Nachemson A. New observations on the mechanical behavior of lumbar discs. Acta Orthop Scand. 1954;23:254-283.
58. Hirsch C., Schajowicz F. Studies on structural changes in the lumbar annulus fibrosus. Acta Orthop Scand. 1953;22:184-231.
59. Hirsch C. Studies on the mechanism of low-back pain. Acta Orthop Scand. 1951;20:261-274.
60. Evans F.G. Studies in human biomechanics. New York Acad Sci. 1955;63:586-615.
61. Evans F.G. Stress and strain in bones. Their relation to fractures and osteogenesis. Springfield: Charles C. Thomas; 1957.
62. Higgins L.S. Studies on vertebral injuries sustained during aircrew ejection. Washington, D.C.: Office of Naval Research, Contract No. NONR-4675(00); May 1965.
63. Friberg S., Hirsch C. Anatomical and clinical studies on lumbar disc degeneration. Acta Orthop Scand. 1949;19:222-242.
64. Sylven B., Paulson S., Hirsch C., et al. Biophysical and physiological investigations on cartilage and other mesenchymal tissues. II. The ultrastructure of bovine and human nuclei pulposi. J Bone Joint Surg (Am). 1951;33:333-340.
65. Werne S. Studies in spontaneous atlas dislocation. Acta Orthop Scand Suppl. 1957;23:1-150.
66. Courant R., Hilbert D. Methods of mathematical physics. New York: Interscience Publishers, 1953;vol 1.
67. Hess J.L., Lombard C.V. Theoretical investigations of dynamic response of man to high vertical accelerations. J Aviation Med. 1958;29:66.
68. White A.A., Panjabi M.M. Clinical biomechanics of the spine. Philadelphia: Lippincott Williams and Wilkins; 1990.
69. Holdsworth F. Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg (Am). 1970;52:1534-1551.
70. Denis F. The three column injury and its significance in the classification of acute thoracolumbar spinal injuries. Spine. 1983;8:817-831.
71. Kumar K. Did the modern concept of axial traction to correct scoliosis exist in prehistoric times? J Neurol Orthop Med Surg. 1987;8:309-310.






