Chapter 12
Wound management, tissueviability and infection
Jeannie Donnelly1, Alison Collins2 and Julie Santy-Tomlinson3
1 Queens University Belfast/Belfast Health and, Social Care Trust, Belfast, UK
2 Belfast City Hospital, Belfast, UK
3 University of Hull, Hull, UK
Introduction
This chapter provides an outline of the knowledge and skills required by practitioners caring for patients with the main types of acute and chronic wounds in the field of trauma and orthopaedics. Recommendations for practice will often be pragmatic as empirical research is, in many instances, lacking. The chapter is divided into two sections. Section 1 focuses on the nursing management of wounds. This will include consideration of both surgical and traumatic wounds, an overview of the wound healing process and will discuss current thinking with regards to dressing techniques. Section 2 will consider issues relating to the prevention and management of pressure ulceration.
Whilst all wound types move through the three main stages of wound healing (inflammation, proliferation and contraction), speed and efficiency of healing is affected by a range of local and systemic factors. Key factors (according to wound type) will be highlighted. These must not, however, be viewed as mutually exclusive as all factors e.g. smoking and infection, will affect all wound types.
Wound management
Surgical wounds
A simple surgical wound is a healthy and uncomplicated break in the continuity of the skin resulting from surgery. It is expected to follow a rapid and predictable pathway towards healing with minimal tissue loss, scarring and loss of function. Surgeons take great care to protect as much tissue as possible from injury, carefully considering the placement of the incision, managing blood loss (to prevent haemorrhage and haematoma) and considering the best way to bring each layer of tissue (muscle, fascia, subcutaneous tissue and skin) into approximation through wound closure (Coulthard et al., 2010). Approximation speeds time to healing, reduces scaring and helps prevent infection. The wound is said to heal by primary intention.
Traumatic wounds
Traumatic wound care is an integral part of the care of the patient following musculoskeletal trauma as soft tissue wounds are often consistent with the rest of the pattern of injury. Such wounds present a number of additional challenges. A compound fracture wound with full thickness tissue loss, for example, requires careful assessment (as there may be damage to nerves, tendons or muscles) and debridement of devitalised tissue. Often the wound cannot be closed immediately due to the risk of or presence of infection or excessive oedema. Closing very oedematous tissue will result in a taut wound leading to stress which can cause tissue ischaemia (reduced blood flow), particularly at the wound edge, potentially leading to tissue death or wound dehiscence (gaping or bursting open). To prevent this from happening body cavities and deeper structures are sutured closed and the layers of the skin left open to allow for free drainage of foreign material or pus or whilst waiting for swelling to decrease. The patient will normally return to surgery after 3–4 days for a further wound assessment, followed by irrigation and debridement and wound closure if it is safe to do so. This is known as delayed primary closure. The wound is said to heal by tertiary intention (Lorenz and Longaker 2008).
Some wounds cannot be closed using surgical techniques due to one or more of the following reasons: (a) the patient is not well enough to undergo surgery, (b) the wound is small or superficial (c) the wound is heavily contaminated, infected or chronic or (d) the wound is deep with a ‘dead space’ and lack of subcutaneous tissue. If the skin is left open it is important to prevent the dead space filling with blood as haematoma is the perfect medium for bacteria to multiply and as it does not have a blood supply to initiate the immune system. Healing is by secondary intention.
The wound healing process
Wound healing is the process by which damaged tissue is replaced and function restored. The wound healing process is dynamic and can be divided into three overlapping phases: haemostasis/inflammation, proliferation and maturation (remodelling).
During haemostasis damaged blood vessels constrict and blood leaking from them begins to coagulate. Platelets in the vicinity are ‘activated’ by collagen fibres in the damaged vessels and clump together forming a relatively unstable plug. The activated platelets release vasoconstrictors and other chemicals which stimulate the clotting cascade and attract other platelets to the area. The end result is a clot (platelets intertwined with fibrin).
The goal of the inflammatory phase of wound healing is to limit the amount of tissue damage and prepare the wound for healing by removing unhealthy tissue and foreign matter such as bacteria. White blood cells (basophils, neutrophils and monocytes) play a major role. Basophils release heparin and histamine. Neutrophils and monocytes (converted to macrophages) migrate from the blood vessels and congregate at the site of injury, engulfing and destroying microorganisms. The inflammatory process is a necessary part of healing. Visible signs of the process are redness, heat, swelling, pain, loss of function and increased exudate.
The goal of the proliferation phase is to close the defect as quickly as possible. The wound fills with granulation tissue (unless it is very superficial in which case it will simply re-epithelialise), contracts down in size and epithelialises. Viable epidermal cells divide and migrate from the wound edges. Migration ceases when the epidermal cells come into contact with each other.
Granulation tissue is a network of collagen fibres, new blood vessels and white blood cells and peaks between five and nine days post-operatively, presenting as a ‘healing ridge’ along the margins of the wound (Doughty and Defriese 2007). New blood vessels form by the process of ‘angiogenesis’. New capillaries (containing oxygen-rich blood and micronutrients) give the tissue a bright red granular appearance. Oxygen is important for cellular activity and any condition that impedes oxygenation of the tissues (e.g. smoking, peripheral vascular disease) slows healing and can lead to wound breakdown (Knuutinen et al., 2002). Dark coloured granulation tissue, which bleeds easily, can be indicative of infection, poor perfusion or ischaemia.
Good nutrition (see Chapter 10) is central to successful wound healing. Malnutrition may involve a deficiency or excess (or imbalance) of energy, protein and other nutrients which can be a significant factor in wounds failing to heal or succumbing to infection.
Maturation occurs once the wound has re-epithelialised and strengthens the scar tissue. Weak Type III collagen fibres (produced by fibroblasts during granulation) are changed into or replaced by strong Type I collagen. As the wound has essentially healed there is a downturn in cellular activity and the need for extra oxygen and nutrients decreases.
In a simple surgical wound, the inflammatory phase is usually complete within 36–48 hours and the proliferative phase is complete in 28 days. Maturation can take around 100 days. A surgical wound is usually ‘sealed’ within 48 hours and will be dry (no bleeding or exudate) and can be exposed. The time frame is variable and may be extended depending on the complexity of the surgery, local wound conditions and the health of the patient. A patient whose wound continues to produce a high amount of exudate five days post-operatively, or who is complaining of increasing pain may have a surgical site infection (SSI). Wounds which are open or continue to ‘weep’ (exude) will need to be carefully monitored and dressed.
The phases of wound healing are dynamic; wounds may move forwards or backwards through each phase depending on the health of the patient. For example, a wound which was healing well (showing signs of granulation) but becomes infected, will move back into the inflammatory stage. A chronic wound is often described as a wound which is ‘stuck’ in the inflammatory or proliferative phase of wound healing.
Factors affecting wound healing
Factors affecting wound healing are often referred to as intrinsic (internal – specific to the individual) or extrinsic (external – applied to the individual). Any systemic condition which results in poor perfusion, a lack of essential micronutrients, the ability to fight infection or tissue wasting/destruction can delay wound healing (Table 12.1).
Table 12.1 Factors and conditions affecting wound healing
| Factor | Relevant conditions |
| Poor perfusion |
|
| Micronutrient deficiency |
|
| Immunodeficiency/suppression |
|
| Tissue wasting/destruction |
|
To aid wound healing, the general health and well-being of the patient must be optimised. This is achieved by creating a care plan which takes into account relevant health and psychosocial issues. Nurses, as ‘gatekeepers’ of care, have a responsibility to use their knowledge of the patient’s needs and refer to other practitioners when help is needed.
Extrinsic factors that affect healing can be mechanical (pressure, shear, friction), chemical (wound exudate, cleansing solutions etc.) or thermal (heat, cold, radiation). Some of these factors (such as a moist wound environment) can aid healing, whilst others can delay healing.
Moist wound healing
Surgical wound dressings are applied to stem bleeding, absorb exudate and provide protection but there is constant debate about which dressing product best achieves such functions. Dry dressings may adhere to the wound (as fibres integrate into the clot matrix) causing pain and trauma on removal. Woven dressings are commonly used with the objective of absorbing wound moisture. It is claimed, however, that moist wounds heal more quickly than those left to dry out under textile-based dressings because epithelialisation is retarded by the formation of a dry scab (Winter 1962). A dressing which facilitates an optimal level of wound moisture, on the other hand, promotes wound healing (Harle et al., 2005). Orthopaedic wound dressings should therefore have the attributes of the ideal dressing (Box 12.1) in addition to being absorbent and protective. The ability of a wound dressing to stretch with movement to avoid restricting limb movement and accommodate postoperative oedema is also important especially after hip and knee arthroplasty which requires a degree of force on behalf of the surgeon to position the prosthesis firmly, thereby resulting in postoperative bruising and swelling around the joint (Jester et al., 2000).
Permeability and transparency
The permeability of a dressing refers to its ability to permit gaseous exchange (including water vapour) between the wound and external environment. Transparent films allow wound exudate and peri-wound skin to be inspected without dressing removal, minimising the risk of accidental wound contamination and trauma. Exudate, however, can pool under film dressings and cause maceration of the wound and surrounding skin (Cutting and White 2002) and peri-wound blister formation (Harle et al., 2005). Absorbent central pad dressings with an adhesive border are quicker and easier to apply than traditional dressing pads, but offer no additional advantages in terms of permeability. Vapour-permeable film dressings transmit moisture away from the wound bed to varying degrees, but should not be applied as the primary dressing at sites of profuse drainage since absobency is limited. ‘Film plus fabric’ dressings combine transpiration and absorbency, helping to prevent accumulation of fluid (Aindow and Butcher 2005). The moist and relatively hypoxic environment produced by semi-occlusive and occlusive dressings accelerates angiogenesis and promotes tissue repair (Holm et al., 1998). See Box 12.2 for further discussion of wound moisture balance.
Ability to act as a bacterial barrier
Traditional absorbent dressings provide limited protection against microbial ingress and may shed fibres into the wound, causing a focal point for infection (Jones 2006). Microbes pass through the dressing rapidly when it is damp and are dispersed into the environment on dressing removal, increasing the risk of cross-infection (Cooper and Lawrence 1996). Vapour-permeable films, incorporated into a fabric-island dressing or used as a retention dressing, have the advantage of being impermeable to bacteria (Pudner 2001). Hydrocolloids protect the wound from exogenous bacteria and have the advantage of lowering the pH of wounds to slightly acidic, inhbiting the growth of microbes (Bryan 2004). Hydrofibre dressings protect the wound from bacterial invasion by absorbing and retaining large amounts of exudate (including microbes) (Clarke et al., 2009), reducing the need to change the dressing (Ravenscroft et al., 2006) and lessening dispersal of microbes on dressing removal (White 2001).
Bathing and showering
There is a strong correlation between patient satisfaction with the postoperative dressing and ability to perform their usual personal hygiene routine (Bhattacharyya et al., 2005). There is arguably no need to apply any dressing to a surgical wound after the early postoperative period since a natural bacteria-proof barrier (fibrin seal) is quickly re-established. Patient hygiene is facilitated and worry about the wound reduced by use of a vapour-permeable film until the wound is sealed with fibrin and drainage has ceased. Environmental moisture has a minimal effect on waterproof dressings providing it does not migrate under the surface. For this reason showering is preferable to bathing.
Ease of removal
Patients may experience pain where traditional gauze dressings adhere to the wound bed. Paraffin tulle gras also has a tendency to dry out and may result in postoperative wound trauma (Voegeli 2008). According to Gupta et al. (2002), spirit-soaked gauze lifts off the wound as it dries. However, spirit-soaked gauze is likely to cause pain on contact with broken skin due to the astringent properties of alcohol-based preparations. Alcohol solutions delay wound healing and usage should be restricted to prophylactic skin disinfection (Morgan 2004). Ravenscroft et al. (2006) found removal of hydrofibre and film combined to be less painful than an adhesive fabric dressing.
Wounds can exhibit a wide combination of different characteristics, e.g. deep tissues may be exposed or the wound may be malodourous with a high or low exudate. There is no one product which is ‘smart’ enough to manage all of these. Characteristics change as they move through the healing continum and practitioners must use their assessment to set realistic treatment objectives and make evidence based dressing choices.
Wound assessment
The first part of a wound assessment is to take a history of all factors leading to the cause of the wound. This information will provide clues to the underlying aetiology, the amount and type of tissue damage as well as potential complications such as infection. The five questions listed in Table 12.2 will help in this process. The second part of the assessment is to carefully observe the wound and the surrounding tissues to guide care and the choice of dressing. Results of the assessment should be recorded on a wound observation chart.
Table 12.2 Wound history questions for wound assessment
| Question | Rationale |
| Why is it there? |
|
| Where is the wound? |
|
| When did it appear? |
|
| Who is looking after the patient/client and their wound? |
|
| What would the patient/client like to achieve? |
|
Wound measurement
The length, width and depth of the wound should be recorded as accurately as possible using a sterile disposable tape measure (which must not touch the wound). The length and width of the wound should be measured using the body axes as a reference point (as opposed to the longest and shortest part of the wound). Dimensions can change rapidly and over time measurements can become confused. In a wound where depth is easily visualised, a sterile probe can used to measure the distance from the bottom of the wound to the surface of the skin. Some wounds consist of extensive cavities or extremely narrow sinuses and the skin can be undermined, leading to exposure of fragile structures (blood vessels, nerves, organs). Wounds should not be probed unnecessarily as these fragile structures can be easily damaged. A surgeon or a tissue viability nurse may be able to map out the wound to assess the direction/depth of cavities. The dimensions of a wound which contains necrosis or slough will increase as ‘dead’ tissue is autolysed.
Wound bed
The wound bed tends to be described by the colour of tissue observed (black/brown, yellow, red and pink) (Table 12.3), indicating underlying problems such as ischaemia or tendon exposure. For example, if hard black necrosis is noted on the heel (Figure 12.1) it would be wise to assess the blood supply to the lower limb before wound debridement. If there is no blood supply, tissue cannot regenerate or mount an effective host response to infection. Tendons on the other hand, need to be kept moist to prevent dessication and loss of function. If there is no blood supply the practitioner should keep the wound dry and seek specialist help. As wounds can contain a mixture of tissues it can be difficult to accurately quantify what can be seen. Clinical judgement can be used to make a subjective calculation of each tissue type. This is then expressed as a precentage, e.g. 20% black, 50% yellow, 30% red. During dressing changes the percentages are recalculated and compared to the previous assessment. Changes help to determine improvement or deterioration. Photographs can also be useful in charting the progress of extensive wounds.

Figure 12.1 Heel pressure ulcer with necrosis and hard, black eschar
Table 12.3 Wound bed assessment – tissue colour
| Colour | Definition | Differential rationale |
| Black | Tissue is necrotic (dead). There is no blood supply. Hard black necrosis is called eschar. | Dressings and ointments which contain silver (Ag) can stain the tissues a black colour but staining is superficial and temporary |
| Yellow | This tissue is sloughy. Slough is made up of dead cells and wound debris. | Tendons, fascia, bone and fat can also appear yellow. |
| Red | This tissue is healthy. Granulating tissue is comprised of collagen fibres (Type III) and new blood vessels. The new capillaries give the tissue its bright red colour and slightly uneven ‘bumpy’ texture. Dark red granulation tissue is a sign of poor perfusion or infection (Figure 12.2). |
Muscles, organs (such as bowel) and dermis will also be red. Sometimes tissue can over-granulate; often referred to as ‘proud flesh’ as it sits above the level of the skin. It is often seen around trache and peg tube sites. |
| Pink | This tissue is healthy and is re-epithelialising. | The skin surrounding a wound can become very wet and macerated due to excess exudate. This skin can appear pinkish/white in colour. |

Figure 12.2 Wound containing over-granulation tissue
The practitioner must have an understanding of the evidence-based rationale behind dressing selection to enable setting realistic wound management objectives. Dressing products range from those that actively donate moisture to a wound (hydrogels) to those that absorb or contain moisture. Some are impregnated with antimicrobial agents which should not be used unless there are clinical signs of infection or the patient is immunocompromised and there is a very high risk of infection. It is also important that general advice and support is given to the patient with respect to promoting healing and preventing infection.
Surgical site infection
Healthcare-associated infections (HAIs) collectively affect approximately one in ten hospital patients every year (DoH 2006). Such infections are costly complications of heath care that cause pain and discomfort, complicated and delayed recovery and sometimes death (Srinivasaiah 2007). Surgical site infection alone has been reported by NICE (2008) to be responsible for over one-third of perioperative deaths, increased healthcare costs and a significant impact on patient quality of life. Surveillance and prevention of infection are a major focus of health care and are seen as a care quality indicator.
Any infection is the outcome of complex interactions between a host, a pathogen and the environment (EWMA 2005) and is defined as:
(The deposition of organisms in tissues and their subsequent growth and multiplication along with an associated tissue reaction.)
(Ayliffe et al., 2001)
Bacteria cannot penetrate intact skin, but can enter easily if the skin is damaged or an incision is made such as in the case of a surgical or traumatic wound. Infection is a painful and distressing complication that impairs the process of wound healing and is instrumental in delayed recovery. If it is allowed to progress it can lead to death through the spread of infection, septicaemia and organ failure.
The colonisation of any wound with microorganisms is unavoidable. The human body is host to a large number of bacteria and fungi that are part of the normal homeostatic mechanisms and are essential to many physiological processes. Harmful pathogenic organisms, however, are ever-present on the human body, in the atmosphere and in the environment. Ordinarily, the human immune system prevents these potential pathogens from entering the human body and causing harm. Organisms that are normally relatively harmless can become problematic when conventional preventive mechanisms fail.
In the orthopaedic patient the major risk from the spread of infection is osteomyelitis (infection of bone tissue) which is extremely difficult to eradicate. Osteomyelitis is also associated with biofilms attached to implanted devices or haematogenous seeding (spread of bacteria from the blood stream to implant sites) (Trampuz and Zimmerli 2006) and is a much feared complication of bone injury and surgery as the condition often becomes chronic and prevents bone from healing, leading to long-term pain and disability. The prevention of infections, including surgical site infection which may lead to osteomyelitis, is particularly central to the care of all orthopaedic patients.
Surgical site infection (SSI) is defined as:
(Infection occurring up to 30 days after surgery (or up to one year after surgery in patients receiving implants and affecting the incision or deep tissue at the operation site.)
(Owens et al., 2008)
An estimated average of 2–5% of surgical patients develop SSI during their recovery and up to a year following orthopaedic implant surgery (NICE 2008). Most SSIs are caused by skin-derived bacteria, primarily staphylococcus aureus (Dohmen, 2008). Studies of SSI in orthopaedic patients report the incidence of serious deep infections associated with SSIs and highlight consequential increases in the length of hospital stay (Coello et al., 2005). For example, deep wound infection occurs in up to 3% of patients following hip fracture repair. Surveillance data focus on high volume orthopaedic procedures such as arthroplasty and internal fixation of fractures (Morgan et al., 2005). Although rates are dropping each year, SSIs in this group remain a significant problem. In many countries surveillance of SSI rates following orthopaedic surgery for total hip replacement, total knee replacement, hemiarthroplasty and open reduction of long bone fracture is mandatory. Many patients are now discharged from hospital before the surgical wound has healed, so it is likely that the symptoms of SSI may not appear until after discharge from hospital. Following orthopaedic implant surgery, deep surgical site infections may take up to one year to manifest (Health Protection Agency 2008).
Preventing surgical site infection
The use of the most recent evidence-based guidelines for preventing HAIs is central to the prevention of surgical site infection. This should focus on local and national guidance (Chapter 9). Specific measures for the prevention of surgical site infection include:
- Evidence-based preoperative preparation and perioperative care including skin preparation and antibiotic prophylaxis.
- Strict aseptic technique when dressing or handing wounds and wound drains.
- Wound drains should be removed as soon as possible, preferably within 24 hours of surgery.
- Keeping wounds covered in the hospital environment and until the proliferation phase of healing is complete (Box 12.3) and tampering with the wound/dressing as little as possible.
- Ensuring the patient’s general health status and tissue perfusion is optimised through good nutrition and hydration.
- Close postoperative assessment and surveillance of the wound for signs of infection until recovery is complete and immediate medical referral if infection is suspected.
Box 12.3 Evidence digest: Wound dressings to prevent wound surgical site infection
A frequent change of dressings is a potential risk factor for SSI (Leaper 2000) as exogenous bacteria may contaminate the wound during the dressing procedure. The rate of miotic cell division and leucocyte activity (necessary for wound healing and bacterial defence) is increased under wound dressings which facilitate near to core body temperatures (Xia et al., 2000). Frequent cooling associated with changing the dressing should therefore be avoided as a means of reducing the risk of SSI.
Recognising surgical site infection
There are two common approaches to diagnosing infection:
- Assessment of the clinical symptoms of infection based on observation of the wound and the localised and systemic inflammatory response and generalised systemic patient symptoms.
- The laboratory analysis of samples taken from the wound used to identify the type and amount of growth of organisms (microbial load) in the wound.
Clinical assessment findings are widely considered to be a reliable approach to identifying infection in most wounds (Serena et al., 2006) (Table 12.4). Damage to tissue causes an inflammatory reaction that is manifested as symptoms which provide potentially useful indicators of infection. There are four ‘cardinal’ signs of acute inflammation; redness, heat, swelling and pain. An important factor to consider is that, in deep surgical site infections, redness and heat at the base of the wound cannot be seen and may only manifest as pain. Hence any patient report of increasing or unresolved pain must be taken seriously. The presence or drainage of pus is an additional sign of infection in some wounds where the causative organism is ‘pyogenic’ (pus-forming).
Table 12.4 Signs of surgical site infection which should be considered as part of the clinical assessment. Reproduced with permission from The Cochrane Collaboration
| Sign | Rationale |
| Wound site/pain | Pain may reappear after the pain following injury or surgery has subsided. It may also last beyond that which would normally be expected for that injury or surgery. |
| Exudate | Excessive wound exudate which does not settle may be clear serous exudate or a purulent discharge. Discharge may also be dark brown if it arises from infection of a haematoma deep within the surgical site. |
| Foul odour | Indicates the presence of pathogenic microorganisms. |
| Wound breakdown | This may become apparent at the time of removal of sutures or clips and can be the result of an infected haematoma which acts as a barrier to wound healing. |
| Systemic symptoms | The patient may feel generally unwell with flu-like symptoms such as aches, lethargy, pyrexia and hot or cold shivers, disturbed sleep and loss of appetite. |
The use of ‘film plus fabric’ dressings and films (as retention dressings), does not permit clear visual assessment of the wound area for early signs of wound infection such as spreading erythema to be identified (Mansha et al., 2005). Additional signs of infection such as unexpected wound pain or tenderness, malodour, dehiscence, purulent discharge, localised swelling or heat in conjunction with microbiological analysis (Santy 2009) aid differentiation between the normal postoperative inflammatory response and that of inflammation due to infection.
A wound that exhibits clinical signs of infection may instigate sampling of the wound. Laboratory analysis of wound samples can provide the clinician with information about the microbial load within the wound. It cannot, however, differentiate between a colonised wound and an infected wound, so cannot diagnose infection. It can only confirm the presence of organisms in or around the wound and does not provide any information about whether this is having a detrimental effect on the host tissue (Sibbald 2003). Hence, diagnosis of infection should be based on clinical signs. Wound sampling should only be considered in wounds not responding to chosen antibiotics.
Pressure ulcers
Pressure ulcers (PUs, decubitus ulcers, bedsores, pressure sores/injuries) are localised areas of tissue damage that result from pressure or a combination of pressure and shear forces (EPUAP and NPUAP 2009). They usually occur over bony prominences, most commonly the sacrum and the heel bone, but can occur at any site that is subjected to pressure. Global incidence and prevalence surveys show that pressure ulcers remain a common problem. Prevalence rates are influenced by numerous factors such as mortality, length of stay and the influx of admissions, which vary considerably, but can help measure the burden of the problem and help in decision making regarding resource allocation. Incidence studies, which are based on the accumulation of new pressure ulcers, reflect the nosocomial (acquired in hospital/during care) problem and are particularly useful in determining patients at risk and allow inferences regarding the effect of preventive care measures (International Guidelines 2009). Some patient groups are at a higher risk than the general hospital population including those who are critically ill, older adults (>65 years) and people who have reduced mobility such as many orthopaedic patients.
It is difficult to determine the true cost of pressure-related tissue damage but a high prevalence or incidence of pressure ulcers leads to human suffering, lost opportunity costs, extra resources used and potential litigation. It is important that nurses act to reduce the number and severity of ulcers through the delivery of evidence-based care. The physical, social and psychological suffering experienced by patients with pressure ulcers is immense. Hopkins et al. (2006) used a phenomenological approach to explore the ‘endless pain’ and ‘restricted life’, which patients suffer. This distress is caused by: (1) local factors such as pain, wound exudate and malodour, often leading to social isolation; (2) delayed rehabilitation, which may result in economic hardship and (3) serious complications such as cellulitis, osteomyelitis, septicaemia, limb amputation and even death.
Classification of pressure ulcers
In order to improve written and verbal communication amongst practitioners the EPUAP/NPUAP (2009) scale is widely used to classify pressure ulcers. Ulcers are classified into four (six in the USA version) categories depending on the depth of tissue damage:
- The wound is assessed as category/stage I when there is observable erythema that is non-blanchable or persistent along with pain and raised tissue temperature.
- Category/stage II is denoted by partial thickness skin loss with a shallow, open, red/pink ulcer without slough or bruising. This stage might also present as a fluid-filled blister.
- Category/stage III presents as full thickness skin or tissue loss in which subcutaneous fat may be visible. The ulcer may, however, be either shallow or deep and there may also be slough, but not to any great depth (Figure 12.3).
- Category IV refers to deep ulcers in which there is full thickness tissue loss in which there may be exposed bone, tendon or muscle. There may also be slough or eschar present within the wound along with undermining or tunnelling.
In the USA two further categories are often used. Unstageable/unclassified ulcers are those in which there is full thickness skin or tissue loss but the depth is unknown as the wound may be obscured by slough and/or eschar. Suspected deep tissue injury is a further category referring to other wounds in which the depth is unknown. A localised area of purple or maroon but intact skin is recognised as denoting damage to the underlying tissue but the full depth of tissue damage cannot be ascertained.
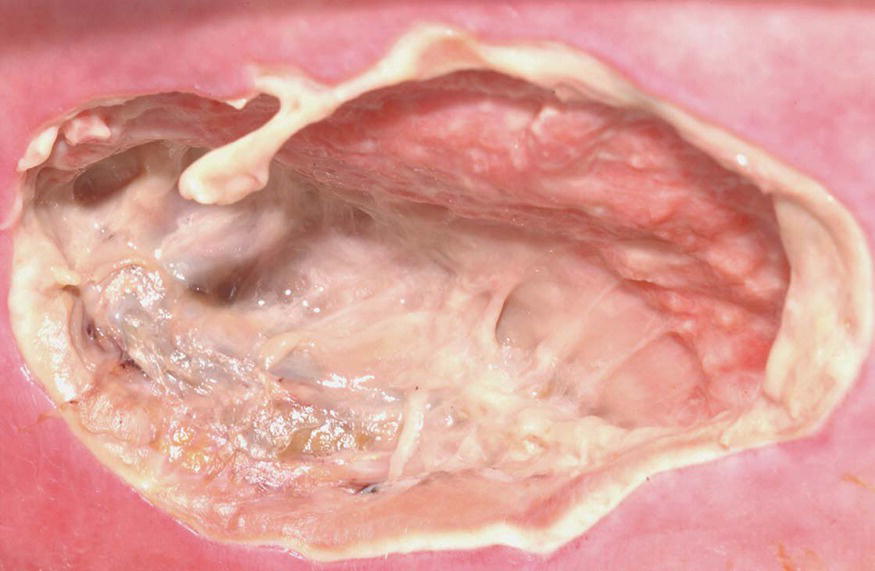
Figure 12.3 Pressure ulcer containing slough
A quick reference guide to this scale can be viewed and downloaded at:
http://www.npuap.org/wp-content/uploads/2012/02/Final_Quick_Prevention_for_web_2010.pdf which offers the practitioner further advice and evidence-based rationale for use of the system.
Pressure ulcer formation
When an external load is applied to the skin, autoregulatory processes allow the internal capillary pressure to rise so that blood flow is reduced. It is believed that pressure damage occurs when the blood supply to the skin is occluded by an external perpendicular force which supersedes internal capillary closing pressure. Intense pressures of short duration are as injurious to tissues as lower pressures applied for a longer period. This demonstrates that, in order to prevent pressure damage, it is essential to reduce the intensity and duration of pressure by, for example, repositioning immobile patients and the use of pressure-redistributing support surfaces.
Other forces such as friction and shear can significantly decrease the tolerance of tissue to directly applied pressure. Extrinsic factors, such as moisture, friction and shear impinge upon the surface of the skin and intrinsic factors reduce the sensation or perception response mechanism or alter the structural constituents and perfusion of tissues. More than 200 contributing factors have been identified in the development of pressure ulcers.
Superficial ulceration
It has been suggested that superficial pressure ulcers occur in one of two ways: (1) the epidermis is simply stripped away from the dermis; this typically occurs as a result of skin being abraded through, for example, repetitive rubbing or poor ‘moving and handling’ techniques (frictional forces); or (2) shear forces distort and damage the microvasculature, which feeds the epidermal basal layer. The basal layer becomes ischaemic and sloughs off.
Deep ulceration
There are two main ways in which deep tissue can suffer significant damage. A typical stage 4 pressure ulcer occurs when the fascia between fat and muscle is unable to block the pressure from damaging underlying muscle and bone (Black et al., 2007). This force directly occludes blood vessels, causing ischaemia. It may also affect arteries that penetrate into bone marrow, sometimes resulting in aseptic necrosis of underlying bone. Meanwhile the dermal capillaries remain largely unaffected, possibly because of other factors such as shear. Shear forces disrupt arterioles in the muscle but, since muscle is a well vascularised tissue, the resulting haematoma is likely to be large and well beyond the capacity of the body to absorb. The lesion will track towards the skin surface. Tissue insult does not end when the pressures and forces are withdrawn, as rapid reperfusion may also contribute to injury.
Preventative care
The detection of early or superficial tissue damage along with the instigation of appropriate and timely care can prevent or reverse the majority of impending pressure ulcers. Guidance for preventative care is enshrined in local, national and international guidelines that highlight that pressure ulcer prevention begins on admission with a baseline skin assessment to determine the presence or absence of pressure damage. This is followed by a holistic assessment to identify factors that may heighten susceptibility.
Risk assessment scales numerically rate a range of risk factors which are added together to indicate the likelihood of pressure damage. Many risk assessment scales, however, have not been tested for predictive ability and factors such as the client group and preventive care can affect sensitivity and specificity. It is important to use scales as a framework for assessment as opposed to the sole indicator of risk. The level of risk can change along with the patient’s condition and it is vital that risk is reassessed at regular intervals. Most healthcare providers have a standard risk assessment format that is used by all staff and local guidelines often govern the frequency and triggers for this.
Following each assessment a care plan must be tailored to address risk factors such as pressure, shear, friction, incontinence, pain and malnutrition with the goal of:
- Maintaining and improving tissue tolerance to pressure through evidence-based skin care and addressing malnutrition.
- Protecting against the adverse effects of external mechanical forces.
Moisture (urine, faeces, perspiration and wound drainage) adversely affect skin in one of five ways:
- It may make skin more susceptible to tissue damage by enhancing the frictional component of a shearing force (Sprigle 2000)
- It can irritate and macerate skin, making it more prone to infections and rashes, resulting in superficial skin loss (Kotter and Halfens 2010).
- Elevated humidity at the skin surface may cause discomfort and agitation, leading to abrasions (Clark 1996).
- Many skin cleansers contain products that remove sebum and surface lipids, drying skin, rendering it vulnerable to water-soluble irritants and increasing friction (Gray et al., 2002).
- Moisture may interact with chemical residues left on bed linen following the laundering process (Alberman 1992) resulting in chemical burn that leads to skin damage.
In order to combat these problems, clinical guidelines highlight the importance of:
- Daily systematic skin assessments, paying attention to bony prominences.
- The promotion of continence and immediate cleansing at time of soiling.
- Mild cleansing agents (pH 5.5) and judicious use of moisturisers that keep skin well hydrated.
- Minimising friction and shear forces through careful positioning, transferring and turning techniques.
Malnutrition, particularly protein–calorie malnutrition, increases an individual’s risk of developing pressure ulcers. This point has been supported by Langer et al. (2003) who carried out a systematic review in order to (a) summarise the best available research and (b) enable evidence-based guidance on the role of nutritional interventions in pressure ulcer prevention and treatment (Box 12.4 and Chapter 10).
The adverse effects of external mechanical forces can be minimised in two ways:
- Completely remove pressure (offload) from the pressure areas using manual repositioning techniques, devices such as pillows and splints and/or alternating mattresses.
- Use a conforming support surface to distribute the body weight over a larger surface area (pressure reduction) and reduce the magnitude and/or duration of pressure between a patient and their support surface (the “interface pressure”) (McInnes et al., 2011).
Turning
The traditional 2-hourly turn originates from attempts to prevent pressure damage in a spinal injury unit (Clark 1998). While there appears to be very little scientific evidence to support its efficacy, research by Moore et al. (2011) indicates that 3-hourly repositioning using the ‘30-degree tilt’ reduced the incidence of pressure damage when compared to a 6-hourly turn. It is not always possible, however, to reposition patients if their underlying physiological condition is critical and unstable. One study that has examined this issue is considered in Box 12.5. Furthermore, 2-hourly repositioning can lead to sleep disruption, which can lengthen recovery, suppress immune function and pre-dispose patients to infection (Carskadon 2005). Gillespie et al. (2012) note that whilst regular movement is important, unnecessary repositioning may cause increased discomfort for people with wounds, stiff joints, bony pain or contractures.
Box 12.5 Evidence digest: Preventive schemes to assess the effects of turning (Defloor et al., 2005)
30-degree tilting regime
It has been argued that the 30o tilt is more effective in off-loading bony prominences than a 90o body turn (Figure 12.4). Each time the patient needs to be repositioned, they are gently rolled 20–30o medially or laterally from the starting point onto ‘soft sites’ (e.g. the side of the buttock) as opposed to bony prominences. Pillows are used to support the body and to act as space fillers. One corner of the pillow is placed under the ankle (to elevate the heel) and the rest of the pillow is moulded into any gaps made by the contour of the limb to create more uniform pressure loads. This should, in theory, reduce the pressure over any one area. Defloor (2000) used TCPO2 measurements to show the benefits of offloading bony prominences using the 30o tilt technique and Moore et al. (2011) showed that it reduced the incidence of pressure damage in elderly at-risk patients in comparison to standard care. The technique is not, however, suitable for all patients; it is contra-indicated, for example, in patients with an acute spinal injury and may be contraindicated in patients following a hip arthroplasty due to the risk of iatrogenic injury and contractures.
Figure 12.4 (a, b, c, and d) Performing the 30 degree tilt
Pillows
The benefits and risks associated with the use of pillows as a pressure relieving device is under-researched. Heels which project beyond pillows are subject to zero pressure (Smith 1984), suggesting that carefully placed pillows (Figure 12.4c) can be a cost-effective way of offloading the heel. Smith, however, believed that pillows were unacceptable due to the increased risk of deep venous thrombosis and there are also concerns about the pressure which may be exerted over the Achilles tendon. Sigel et al. (1973), however, noted that a body tilt to a 10-degree foot-up position increased venous flow by 30%, suggesting that with a pillow in situ simply tilting the bed could offset any risk of deep venous thrombosis. In acutely ill bed-bound patients any potential risk of a venous thromboembolism would be minimised through the current standard treatment (Chapter 9). Concern that inappropriately placed pillows can lead to knee contractures can be overcome by placing pillows lengthways, i.e. from just below the crease of the knee to the ankle or using the pillow as a ‘space-filler’. Both of these techniques should maximise the surface contact area and reduce pressure on all parts of the lower leg. In addition, bending the knee section of a profiling bed helps to reduce the risk that the knee will become hyperextended. Pillows are easily ‘kicked’ out of the safe position; heels may lie on the pillow rather than over the edge of the pillow and the heel area will be subject to pressure and tissue could become damaged (Donnelly 2005).
Collars
Cervical collar related pressure ulcers remain relatively common. They commonly occur on the occiput, the chin and the shoulders. Risk factors include ICU admission (P = 0.007), mechanical ventilation (P = 0.005), the necessity for cervical MRI (P ≤ 0.001) and time to cervical spine clearance (P ≤ 0.001) (Ackland et al., 2007). Interestingly, the time to cervical spine clearance was the major indicator, with a 66% increase in risk of tissue damage for every one day increase in cervical collar time (Chapter 19). There are a number of actions which nurses can take to reduce the risk of pressure damage:
- change the patient from a rigid to a semi-rigid collar as soon as possible
- ensure the collar is fitted correctly and is the right size
- remove the collar every 4 hours for skin assessment and hygiene
- hair should be parted and hidden pressure points such as the occiput inspected for signs of redness or discolouration
- check the chin, mandible, ears, shoulders, sternum and laryngeal prominence for pressure damage
- wash and dry the skin carefully
- men should be shaved for comfort and to prevent skin irritation.
- check the collar padding – this must be changed if it is wet or soiled
- if necessary adjust the pad so that no plastic touches the skin.
Heel splints
Devices which completely offload the heel, appear to be more effective than support surfaces in reducing the incidence of heel pressure ulcers. In a recent study (Donnelly et al., 2011), older patients with a fracture of the hip were randomly allocated to receive heel elevation plus use of a pressure-redistributing support surface or standard care (pressure-redistributing support surface alone). Findings indicated that subjects in the control group (heels down) were more likely than those in the intervention group (heel elevation) to suffer pressure damage. The challenge with current devices is that many patients find them uncomfortably warm and too heavy. Further consideration is given to safe care of casts and traction in Chapter 8.
Alternating support surfaces
Alternating pressure redistributing devices (mattresses replacements, overlays and cushions) contain a number of air-filled ‘cells’, which alternately inflate and deflate beneath the patient, mimicking normal body movement. As these cells inflate they generate high interface pressures, but because these are only sustained for a short period of time, the body is (arguably) able to withstand the pressure. As soon as the cells deflate, the hypoxic tissue is reperfused by the normal hyperaemic response. Allen et al. (1993) noted, however, that no studies have shown that bony prominences such as the heel are completely offloaded and remain vulnerable to damage. As most immobilised patients experience reduced blood flow, alternating pressure may also have an effect on tissue perfusion, resulting in improved blood flow and facilitating the prevention of pressure ulcers.
Pressure-reducing support surfaces (constant low pressure devices)
Pressure-reducing support surfaces are designed to mould around the shape of the patient. They increase the amount of contact that the body has with the support surface, thus reducing the magnitude of interface pressures at any given anatomical location. Although many different types of pressure-reducing devices are available, a systematic review of the literature has been unable to determine which is most effective with regards to pressure ulcer prevention (McInnes et al., 2011). The review determined that higher specification foam mattresses offer more protection than standard hospital foam mattresses and that air-fluidised beds may improve pressure ulcer healing rates. Pressure-redistributing equipment presently used to prevent pressure ulcers has not been fully and reliably evaluated.
Management of pressure ulcers
Inevitably, most orthopaedic practitioners will continue to care for patients with pressure ulcers. Good fundamental care which includes nutritional support and hydration remains central to this. Without the pressure ulcer prevention measures discussed above no pressure ulcer will heal. Hence it is only when all possible prevention measures are in place that a focus on good wound management practice can be made with a view to healing the ulcer. Practitioners must make intelligent use of wound management guidelines discussed in the first section of this chapter.
Recommended further reading
- Bryant, R.A. and Nix, D.P. (eds) (2011) Acute and Chronic Wounds: Current Management Concepts, 4th edn. Mosby, St. Louis.
- Dealey, C. (2012) The Care of Wounds. A Guide for Nurses, 4th edn. Wiley Blackwell, Oxford.
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel (EPUAP/NPUAP) (2009) Treatment of Pressure Ulcers: Quick Reference Guide. Washington DC: National Pressure Ulcer Advisory Panel (online). Available at: http://www.npuap.org/wp-content/uploads/2012/02/Final_Quick_Prevention_for_web_2010.pdf (accessed 2 January 2014).
- Flanagan, M. (2013) Wound Healing and Skin Integrity. Principles and Practice. Wiley Blackwell, Oxford.
References
- Ackland, H.M., Cooper, J., Malham, G.M. and Kossmann, T. (2007) Cervical Spine Factors Predicting Cervical Collar-Related Decubitus Ulceration in Major Trauma Patients. Spine, 32(4), 423–428.
- Aindow, D. and Butcher, M. (2005) Films or fabrics: is it time to reappraise postoperative dressings? British Journal of Nursing, 14(19), S15–S20.
- Alberman, K. (1992) Is there any connection between laundering and the development of pressure sores? Journal of Tissue Viability, 2(2), 55–56.
- Allen, V., Ryan, D.W. and Murray, A. (1993) Potential for bed sores due to high pressures: influence of body sites, body position, and mattress design. British Journal of Clinical Practice, 47(4),195–197.
- Ayliffe, G.A., Babb, J.R. and Taylor, L.J., (2001) Hospital Acquired Infection. Principles and Prevention, 3rd edn. Arnold, London.
- Bhattacharyya, M., Bradley, H., Holder, S. and Gerber, B. (2005) A prospective clinical audit of patient dressing choice for post-op arthroscopy wounds. Wounds UK, 1(1), 30–34.
- Black, J., Baharestani, M., Cuddigan, J. et al. (2007) National Pressure Ulcer Advisory Panel’s Updated Pressure Ulcer Staging System. Urologic Nursing, 27(2), 144–150.
- Bryan, J. (2004) Moist wound healing: a concept that changed our practice. Journal of Wound Care, 13(6), 227–228.
- Carskadon, M.A. and Dement, W.C. (2005) Normal Human Sleep: An Overview, in Principles and Practice of Sleep Medicine, 4th edn. (eds M.H. Kryger, T. Roth and W.C. Dement), Elsevier Sanders, Philadelphia.
- Clark, M. (1996) The aetiology of superficial sacral pressure sores, in Proceedings of the 6th European Conference on Advances in Wound Management (edsD.L. Leaper, Cherry, G.W. and C. Dealey), MacMillan Press, Amsterdam, pp. 167–170.
- Clark, M. (1998) Repositioning to prevent pressure sores – what is the evidence. Nursing Standard, 13(93), 58–64.
- Clarke, J. V., Deakin, A.H., Dillon, J.M., Emmerson, S. and Kinninmonth, A.W.G. (2009) A prospective clinical audit of a new dressing design for lower limb arthroplasty wounds. Journal of Wound Care, 18(1), 5–11.
- Coello, R., Charlett, A., Wilson, J. et al. (2005) Adverse impact of surgical site infections in English hospitals. Journal of Hospital Infection, 60(2), 93–103.
- Cooper, R. and Lawrence, J. C. (1996) The prevalence of bacteria and implications for infection control. Journal of Wound Care, 5(6), 291–295.
- Coulthard, P., Esposito, M., Worthington, H.V., van der Elst, M., van Waes, O.J.F. and Darcey, J. Tissue adhesives for closure of surgical incisions. Cochrane Database of Systematic Reviews 5(Art. No.: CD004287). DOI: 10.1002/14651858.CD004287.pub3.
- Cosker, T., Elsayed, S., Gupta, S., Mendonca, A. and Tayton, K. (2005) Choice of dressing has a major impact on blistering and healing outcomes in orthopaedic patients. Journal of Wound Care, 14(1), 27–29.
- Cutting, K.F. and White, R.J. (2002) Maceration of the skin and wound bed 1: its nature and causes. Journal of Wound Care, 11(7), 275–278.
- Defloor, T. (2000) The effect of position and mattress on interface pressure. Applied Nursing Research, 13(1), 2–11.
- Defloor, T. and Clark, M. (2005) Pressure ulcer classification tool (PULCLAS), EPUAP, Oxford (online). Available at: http://www.epuap.org (accessed 21 April 2013).
- Department of Health (DOH) (2006) The Health Act 2006: Code of Practice for the Prevention and Control of Healthcare Associated Infection. DoH, London.
- Dillon, J.M., Clarke, J.V., Emmerson, S. and Kinninmonth, A.W.G. (2007) The Jubilee method: A novel, effective wound dressing following total hip and knee arthroplasty, Poster presentation, in Proceedings of the American Academy of Orthopaedic Surgeons Annual Meeting, San Diego, California.
- Dohmen, P.M. (2008) Antibiotic resistance in common pathogens reinforces the need to minimise surgical site infections. Journal of Hospital Infection, 70(S2), 15–20.
- Donnelly, J. (2005) The Importance of a Pilot Study in Informing a Main Study Design, Poster Presentation, in National Pressure Ulcer Advisory Panel 9th National Conference: Merging Missions. Salt Lake City, USA. February 25–26.
- Donnelly, J., Winder, J., Kernohan, W.G. and Stevenson, M. (2011) An RCT to determine the effect of a heel elevation device in pressure ulcer prevention post-hip fracture. Journal of Wound Care, 20(7), 309–312, 314–318.
- Doughty, D.B. and Defriese, B. (2007) Wound-healing physiology, in Acute and Chronic Wounds: current Management Concepts, 3rd edn (eds R.A. Bryant and D.P. Nix), Mosby, St. Louis.
- European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel (EPUAP/NPUAP) (2009) Treatment of Pressure Ulcers: Quick Reference Guide. National Pressure Ulcer Advisory Panel, Washington DC. Available at: www.npuap.org (accessed 21 April 2013).
- Gaine, W.J., Ramamohan, N.A., Hussein, M.G., Hullin, M.G. and McCreath, S.W. (2000) Wound infection in hip and knee arthroplasty. The Journal of Bone and Joint Surgery (British) 82-B(4), 561–565.
- Gillespie, B.M., Chaboyer, W.P., McInnes, E., Kent, B. and Whitty, J.A. (2012) Repositioning for pressure ulcer prevention in adults (Protocol). Cochrane Database of Systematic Reviews 4(Art. No.: CD009958). DOI: 10.1002/14651858.CD009958.pub2.
- Gray, M., Ratliff, C. and Donovan, A. (2002) Perineal skin care for the incontinent patient. Advances in Skin and Wound Care, 15(4), 170–175.
- Gupta, S., Lee, S. and Moseley, L. (2002) Postoperative wound blistering: is there a link with dressing usage? Journal of Wound Care, 11(7), 271–273.
- Harle, S., Korhonen, A., Kettunen, J. and Seitsalo, S. (2005) A randomised clinical trial of two different wound dressing materials for hip replacement patients. Journal of Orthopaedic Nursing, 9(4), 205–210.
- Health Protection Agency (2008) Protocol for Surveillance of Surgical Site Infection. Version 3.4 Surgical Site Infection Surveillance Service. Available at: http://www.hpa.org.uk/webc/hpawebfile/hpaweb_c/1194947388966 (accessed 17 April 2014)
- Holm, C., Petersen, J. S., Gronboek, F. and Gottrup, F. 1998 Effects of occlusive and conventional gauze dressings on incisional healing after abdominal operation. European Journal of Surgery, 164:179–183.
- Hopkins, A., Dealey, C., Bale, S., Defloor, T. and Worboys, F. (2006) Patient stories of living with a pressure ulcer. Journal of Advanced Nursing, 56(4), 345–353.
- International Guidelines (2009) Pressure Ulcer Prevention: Prevalence and Incidence in Context. A Consensus Document. MEP Ltd, London. Available at: http://www.woundsinternational.com/pdf/content_24.pdf (accessed 17 April 2014)
- Jester, R., Russell, L., Fell, S., Williams, S. and Prest, C. (2000) A one hospital study of the effect of wound dressings and other related factors on skin blistering following total hip and knee arthroplasty. Journal of Orthopaedic Nursing, 4(2), 71–77.
- Jones, V.J. (2006) The use of gauze: will it ever change? International Wound Journal, 3(2), 79–86.
- Kotter, J. and Halfens, R. (2010) Moisture lesions: Inter-rater agreement and reliability. Journal of Clinical Nursing, 19,716–720.
- Knuutinen, A., Kokkonen, N., Risteli, J. et al. (2002) Smoking affects collagen synthesis and extracellular matrix turnover in human skin. British Journal of Dermatology, 146,588–594.
- Langer, G., Knerr, A., Kuss, O., Behrens, J. and Schlömer, G.J. (2003) Nutritional interventions for preventing and treating pressure ulcers. Cochrane Database of Systematic Reviews 4(Art. No.: CD003216). DOI: 10.1002/14651858.CD003216.
- Leaper, J. (2000) Wound Infection, in Bailey and Love’s Short Practice of Surgery, 23rd edn. Arnold, London, pp. 87–98.
- Lorenz, P. and Longaker, M.T. (2008) Wounds: biology, pathology and management, in Surgery: Basic Science and Clinical Evidence (eds J.A. Norton, P.S. Barrie, R.R., Bollinger et al. ), Springer, New York, pp. 191–205 .
- Mansha, M., Sharif, K., Sharif, Z., Kashif, F.A. and Diggory, P. 2005 The impact of different methods of wound closure and dressing on the rate of wound infection in patients with fracture neck of femur. Journal of Orthopaedic Nursing, 9(4), 195–198.
- McInnes, E., Jammali-Blasi, A., Bell-Syer, S.E.M., Dumville, J.C. and Cullum, N. (2011) Support surfaces for pressure ulcer prevention. Cochrane Database of Systematic Reviews 4(Art. No.: CD001735). DOI: 10.1002/14651858.CD001735.pub4.
- Moffat, C.J (2005) Identifying Criteria for Wound Infection. European Wound Management Association (EWMA) Position Document. MEP Ltd., London.
- Moore, Z., Cowman, S. and Conroy, R.M. (2011) A randomised controlled clinical trial of repositioning, using the 30° tilt, for the prevention of pressure ulcers. Journal of Clinical Nursing, 20, 2633–2644.
- Morgan, D.A. (2004) Formulary of Wound Management Products. A Guide for Healthcare Staff, 9th edn. Euromed Communications Limited, Surrey.
- Morgan, M., Black, J., Bone, F. et al. (2005) Clinician-led surgical site infection surveillance of orthopaedic procedures: a UK multi-centre pilot study. Journal of Hospital Infection, 60(3), 201–212.
- National Institute for Clinical Excellence (NICE) (2008) Surgical Site Infection: Prevention and Treatment of Surgical Site Infection. NICE, London.
- Nixon, J, (2001) The Pathophysiology and Aetiology of Pressure Ulcers, in The Prevention and Treatment of Pressure Ulcers, 2nd edn (ed. M.J. Morison), Mosby, Edinburgh, pp. 17–36.
- Owens, C.D. and Stoessel, K. (2008) Surgical site infection: epidemiology, microbiology and prevention. Journal of Hospital Infection, 70(S2), 3–10.
- Pudner, R. (2001) Postoperative dressings in wound management. Journal of Community Nursing, 15(9), 33–37.
- Ravenscroft, M., Harker, K. and Buch, K. (2006) A prospective, randomised, controlled trial comparing wound dressings used in hip and knee surgery: Aquacel® and Tegaderm™ versus Cutiplast™. Annals of the Royal College of Surgeons of England, 88(1), 18–22.
- Santy, J. (2009) Recognising infection in wounds. Nursing Standard, 23(7), 53–4, 56, 58.
- Serena, T., Robson, M.C., Cooper, D.M. and Ignatius, J. (2006) Lack of reliability of clinical/visual assessment of chronic wound infection: the incidence of biopsy-proven infection in venous leg ulcers. Wounds, 18, 197–202.
- Sibbald, R.G., Orsted, H., Schultz, G.S., Coutts, P. and Keast, D. (2003) Preparing the wound bed 2003: focus on infection and inflammation. Ostomy Wound Management, 49(11), 24–51.
- Sigel, B., Edlestein, A.L., Felix, R. and Memhardt, C.R. (1973) Compression of the deep venous system of the lower leg during inactive recumbence. Archives of Surgery, 106, 38–43.
- Smith, I. (1984) Heel aids. Nursing Times, 80(36), 35–39.
- Sprigle, S. (2000) Effects of forces and the selection of support surfaces. Topics in Geriatric Rehabilitation, 16(2), 47–62.
- Srinivasaiah, N. Dugdall, H., Barrett, S. and Drew, P. (2007) A point prevalence survey of wounds in the north-east of England. Journal of Wound Care, 16(10), 413–419.
- Trampuz, A. and Zimmerli, W., (2006) Diagnosis and treatment of infections associated with fracture fixation devices. Injury, 37(2 Suppl), S56–S59.
- Vanderwee, K., Grypdonck, M.H.F. and Defloor, T. (2005) Effectiveness of an alternating pressure air mattress for the prevention of pressure ulcers. Age and Ageing, 34(3), 261–267.
- Voegeli, D. (2008) The effect of washing and drying practices on skin barrier function. Journal of Wound, Ostomy and Continence Nurses, 35(1), 84–90.
- Winter, G.D. (1962) Formation of the scab and the rate of epithelialisation of superficial wounds in the skin of the young domestic pig. Nature, 193, 293–294.
- White, R. (2001) New developments in the use of dressings on surgical wounds. British Journal of Nursing, 10(6), S70.
- Xia, Z., Sato, A., Hughes, M.A. and Cherry, G.W. (2000) Stimulation of fibroblast growth in-vitro by intermittent radiant warming. Wound Repair Regeneration, 8(2), 138–144.
Related posts:
 Professional development, competence and education
The complications of musculoskeletal conditions and trauma
Professional development, competence and education
The complications of musculoskeletal conditions and trauma
 The team approach and nursing roles in orthopaedic and musculoskeletal trauma care
The team approach and nursing roles in orthopaedic and musculoskeletal trauma care
 Soft tissue, peripheral nerveand brachial plexus injury
Soft tissue, peripheral nerveand brachial plexus injury
 Key musculoskeletal interventions
Key musculoskeletal interventions
