CHAPTER 31 Wound Closure and Postoperative Orthosis
The final steps in the operative procedure are wound closure and placement of the postoperative orthosis. Wound closure after implantation of a reverse prosthesis is performed similar to cases of unconstrained shoulder arthroplasty. Because of the void created by lack of a rotator cuff, wound closure becomes more important after insertion of a reverse prosthesis than in cases of unconstrained arthroplasty because postoperative hematoma has been the most commonly reported complication after this procedure.1
WOUND CLOSURE TECHNIQUE
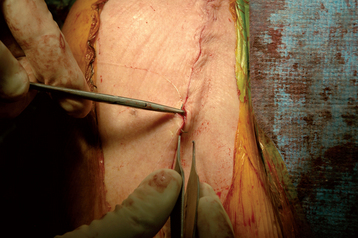
After reduction of the prosthesis and closure of the subscapularis, if present, the wound is irrigated with 800 mL of antibiotic-impregnated sterile saline (50,000 units bacitracin per liter sterile normal saline) via a bulb syringe. The wound is checked to ensure that adequate hemostasis has been obtained. The electrocautery is used as necessary to minimize any residual hemorrhage. A medium-size closed suction drain is placed to help prevent postoperative hematoma formation. The trocar of the drain is used to puncture the soft tissue from inside the wound, and the skin is exited approximately 2 cm distal to the distal extent of the skin incision (Fig. 31-1). The drain is pulled through the skin until the transverse mark on the drain tube reaches the level of the skin (Fig. 31-2). The trocar is removed from the drain with scissors, and the other end of the drain is cut with scissors so that the tip of the drain rests in the void left by the absent rotator cuff (Fig. 31-3). When trimming the proximal end of the drain, care is taken to cut the drain between holes to minimize the risk of drainage tube breakage during removal (Fig. 31-4).


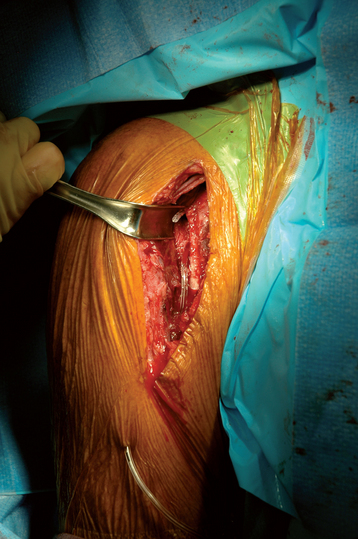
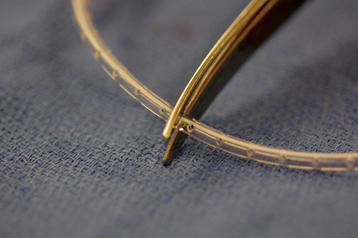
Figure 31-4 Proper trimming of the drain proximally to prevent breakage of the drain during removal.
Wound closure is initiated by reapproximating the deep fascial layer with no. 0 braided absorbable suture in an interrupted figure-of-eight technique (Fig. 31-5). Just as in cases of unconstrained shoulder arthroplasty, we do not close the deltopectoral interval. The sub-cutaneous fascia is reapproximated with 2-0 braided absorbable suture in an interrupted figure-of-eight technique (Fig. 31-6). The skin is reapproximated with 3-0 undyed absorbable monofilament suture in a subcuticular running closure technique (Fig. 31-7).


After skin closure is completed, the drain is checked to ensure that its position has been maintained. The occlusive draping is carefully removed from the site at which the drain tubing exits the skin. The skin in this area is cleaned and dried. Half-inch Steri-Strips are wrapped around the drain tubing to fix the drain to the skin and prevent inadvertent removal of the drain; we use two or three Steri-Strips (Fig. 31-8).

More of the occlusive draping is removed adjacent to the incision, and the skin is cleansed of blood with a saline-soaked sponge and then dried. Half-inch Steri-Strips are placed over the incision. Sterile gauze is then placed over the incision and a sterile absorbent pad is placed over the gauze. The dressing is secured with 3-inch foam tape. The remainder of the surgical drain is connected to the drainage tube, and the suction function of the drain is activated (Fig. 31-9). The remaining surgical drapes are then removed.

The surgical drain is removed the day after surgery regardless of the amount of drainage recorded. The dressing is maintained in place until postoperative day 3, at which time it is removed and not replaced. After removal of the dressing, the patient is allowed to shower, but submerging the incision in a bathtub is prohibited until 2 weeks postoperatively. The Steri-Strips are progressively removed by the patient as they lose their adhesion to the skin.
POSTOPERATIVE ORTHOSIS
The postoperative orthosis is placed in the operating room immediately after the dressing is applied. For a reverse prosthesis, we use a neutral-rotation sling (Ultrasling, Donjoy, Inc., Vista, CA; Fig. 31-10). The patient is allowed to remove the sling for performance of hand, wrist, and elbow mobility exercises and for hygiene. The duration for which the orthosis is maintained is determined by the presence or absence of humeral metaphyseal bone loss. In uncomplicated cases with sufficient metaphyseal bone, the sling is discontinued and physical therapy initiated 3 weeks after surgery. In patients with humeral metaphyseal bone loss, the sling is maintained for an additional week, and physical therapy is initiated 4 weeks after surgery. Details of the postoperative rehabilitation regimen are provided in Chapter 43.