CHAPTER 22 Wound Closure and Postoperative Orthosis
The final steps of the operative procedure are wound closure and placement of the postoperative orthosis. The major difference from patients undergoing unconstrained shoulder arthroplasty performed for chronic disease is the type of postoperative orthosis used.
TECHNIQUE FOR WOUND CLOSURE
After fixation of the tuberosities, the wound is irrigated with 800 mL of antibiotic-impregnated sterile saline (50,000 units bacitracin per liter sterile normal saline) via a bulb syringe. The wound is checked to ensure that adequate hemostasis has been achieved. An electrocautery is used as necessary to minimize any residual hemorrhage. A drain is not routinely used. However, some patients, particularly those with a history of anticoagulant therapy, may have substantial bleeding from fractured bone surfaces. In this circumstance we consider the use of a medium closed wound suction drain (Bard, Inc., Covington, GA) for 24 hours after surgery (Fig. 22-1). The drain is placed deep to the deltopectoral interval with the trocar provided and exits the skin approximately 3 cm distal to the terminal extent of the skin incision (Fig. 22-2). The proximal extent of the drain tubing is trimmed with heavy scissors to allow the proximal tip of the drain to reach the superior aspect of the humerus (Fig. 22-3). Care is taken to not cut the drain tubing through a side portal because this risks fracture of the drain during removal (Fig. 22-4). Uncut half-inch Steri-Strips are applied immediately to secure the drain distally to skin (Fig. 22-5).

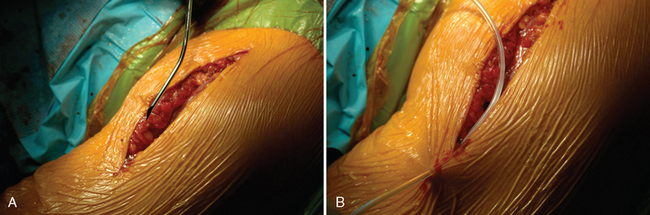
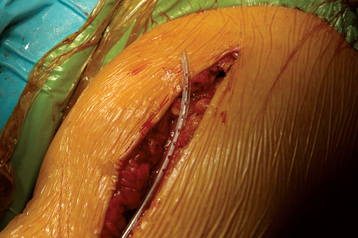
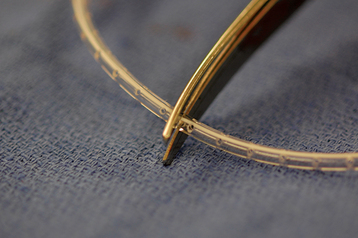

Figure 22-5 Uncut half-inch Steri-Strips are used immediately to secure the drain distally to the skin.
Wound closure is performed in the same manner as described for unconstrained arthroplasty (Chapter 15). We do not close the deltopectoral interval but initiate our closure with the overlying fascial layer. This layer is reapproximated with no. 0 braided absorbable suture in an interrupted figure-of-eight technique. If a drain has been placed, care is taken to avoid passing a suture through or around the drain. Always check that the drain slides freely after sutures are placed in the fascia. The subcutaneous fascia is reapproximated with 2-0 braided absorbable suture via an interrupted figure-of-eight technique. The skin is reapproximated with 3-0 undyed absorbable monofilament suture in a subcuticular running closure.
POSTOPERATIVE ORTHOSIS
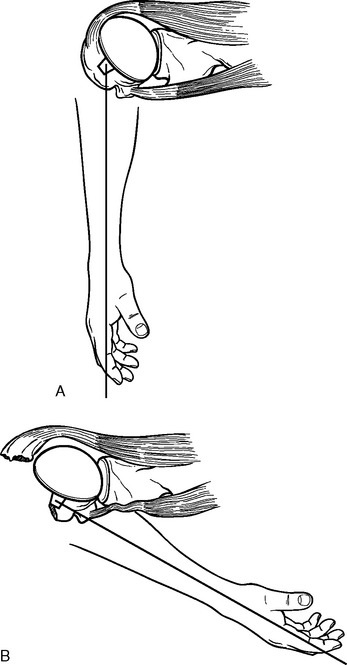
The postoperative orthosis is placed immediately after the dressing in the operating room and consists of a neutral-rotation sling (Fig. 22-6). This sling avoids internal rotation, a situation that places increased tension on the greater tuberosity fixation (Fig. 22-7). The sling is maintained for 4 to 6 weeks to protect the tuberosity repair. In patients with good bone quality and secure tuberosity fixation, the sling is discontinued at 4 weeks. In patients with poor bone quality or less secure tuberosity fixation (or both), the sling is maintained until 6 weeks postoperatively. Patients are allowed to remove the sling only for hygiene and rehabilitation exercises. Patients are discouraged from internally rotating or adducting the arm before the postoperative orthosis has been discontinued because of the potential for tuberosity migration.