CHAPTER 15 Wound Closure and Postoperative Orthosis
The final steps of the operative procedure are wound closure and placement of the postoperative orthosis. These steps are relatively elementary but no less important than other aspects of the procedure.
TECHNIQUE FOR WOUND CLOSURE
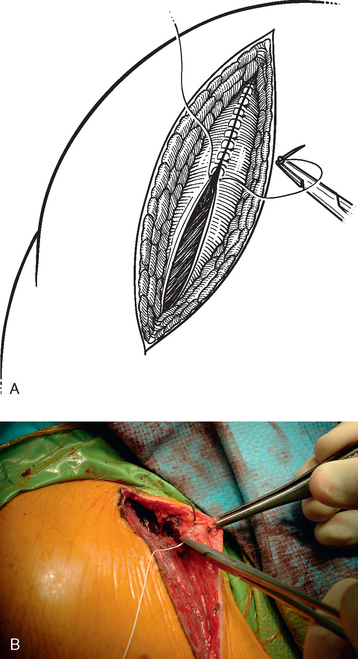
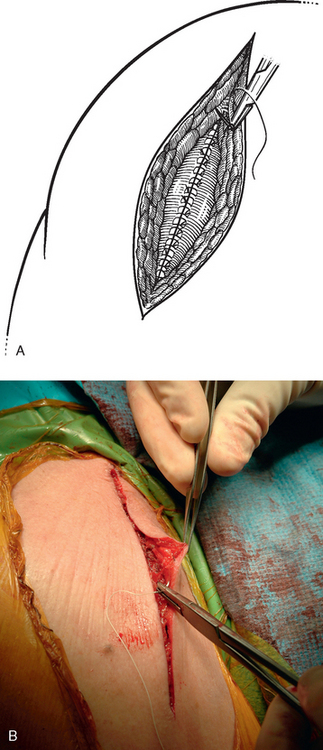
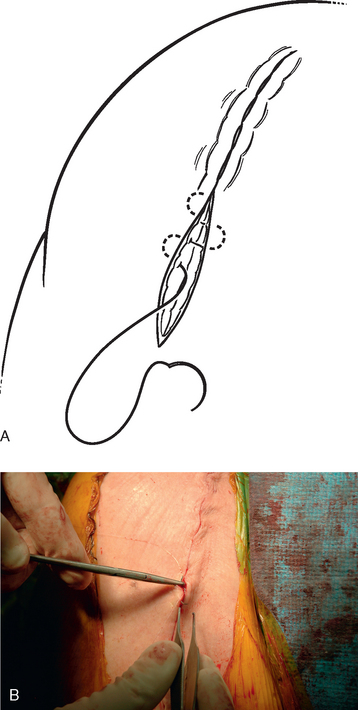
After closure of the subscapularis and rotator interval, the wound is irrigated with 800 mL of antibiotic-impregnated sterile saline (50,000 units bacitracin per liter sterile normal saline) via a bulb syringe. The wound is checked to ensure that adequate hemostasis has been achieved. The electrocautery is used as necessary to minimize any residual hemorrhage. No drain is used because it has been shown to be unnecessary during unconstrained shoulder arthroplasty.1 We do not close the deltopectoral interval but initiate our closure with the overlying fascial layer. This layer is reapproximated with no. 0 braided absorbable suture via an interrupted figure-of-eight technique (Fig. 15-1). The subcutaneous fascia is reapproximated with 2-0 braided absorbable suture via an interrupted figure-of-eight technique (Fig. 15-2). The skin is reapproximated with 3-0 undyed absorbable monofilament suture in a subcuticular running closure (Fig. 15-3).
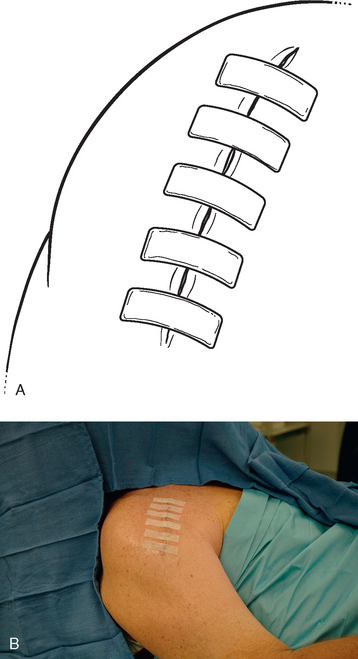
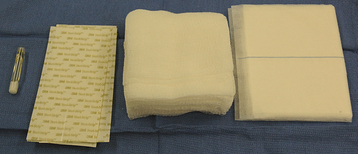
The occlusive draping is removed adjacent to the incision, and the skin is cleansed of blood with a saline-soaked sponge and then dried. Half-inch Steri-Strips are placed over the incision (Fig. 15-4). Sterile gauze is placed over the incision and a sterile absorbent pad is placed over the gauze (Fig. 15-5). The dressing is secured with 3-inch foam tape (Fig. 15-6). The remaining surgical drapes are then removed.

POSTOPERATIVE ORTHOSIS
The postoperative orthosis is placed in the operating room immediately after the dressing is applied. The type of orthosis used is determined by the procedures performed. We use two types of postoperative orthoses. For unconstrained shoulder arthroplasty without an associated posterior capsulorrhaphy, we use a simple sling (Fig. 15-7). This is used for the patient’s comfort and protection and is discontinued whenever the patient decides that it is no longer required, usually between 2 and 4 weeks postoperatively. We ask patients to avoid externally rotating beyond neutral for 4 weeks (6 weeks for inflammatory arthropathy) and to avoid pushing or pulling their body weight with the operated extremity for 8 weeks to protect the subscapularis repair.

In patients who have undergone an associated posterior capsulorrhaphy, we use a neutral-rotation sling (Fig. 15-8). This sling is maintained for 4 weeks to protect the posterior capsulorrhaphy. Patients are allowed to remove the sling only for hygiene and rehabilitative exercises. Additionally, patients who have undergone posterior capsulorrhaphy are cautioned against cross-body adduction and internal rotation behind the back for the first 4 postoperative weeks.