[level-membership-for-physical-medicine-and-rehabilitation-category]
Chapter 17 Wheelchairs and Seating Systems
There is a wide range of choices in wheelchairs. One can choose a wheelchair that is manual, geared, fully powered, power assisted, or standing. There is also an abundance of seating and postural support hardware that can be used to correct or accommodate a wide range of orthopedic deformities and conditions. These include contoured cushions and backrests, tilt-in-space, recline, and custom-molded seating systems. The goals for a wheelchair or seating system are listed in Box 17-1.
Minimize the Risk of Secondary Injuries
Tips and falls account for more than 70% of wheelchair-related accidents.43 It is imperative that individuals be provided with mobility devices that comply with internationally recognized wheelchair standards and can be safely operated (as determined by a skilled therapist or assistive technology professional). Seat belts, wheel locks, and a properly adjusted wheelchair can prevent serious wheelchair-related injuries. Pressure ulcers are also a significant risk for those who use wheelchairs. Advanced cushion designs and seat functions can provide adequate pressure relief for persons who cannot independently off-load the buttocks. Shoulder pathology and nerve compression injuries at the wrist are common among wheelchair users.41 Using proper wheelchair propulsion biomechanics and an optimal wheelchair setup can help delay the onset of overuse injuries.
Ensure Comfort
Along with mobility, comfort has been reported as the most important attribute or function of a wheelchair.16 Research has shown that most wheelchair users experience regular discomfort. Many either ignore it or seek relief by getting out of the wheelchair, using pain medications, or doing weight shifting (either manually or with tilt and recline).16 A wheelchair that allows for “fine-tuning” of the adjustments provides greater options for achieving comfort, as well as meeting the individual’s postural and pressure needs.
Manual Wheelchairs
Persons with good upper body function and stamina might well be able to use a manual wheelchair for mobility. Manual wheelchairs for daily use are often categorized by their design features and costs. Table 17-1 provides an overview of each adult wheelchair category as defined by the Centers for Medicare & Medicaid Services (CMS), which is the leading third-party payer for wheelchairs. The categories are outdated and are being revised to reflect the actual composition of manual wheelchairs on the market.
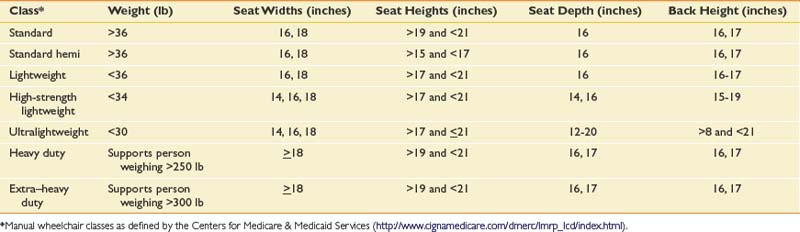
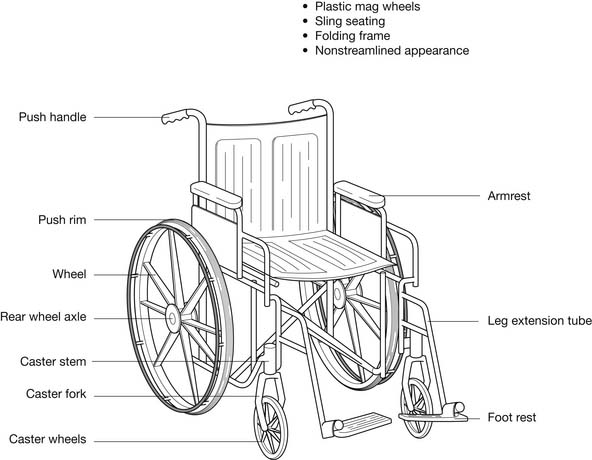
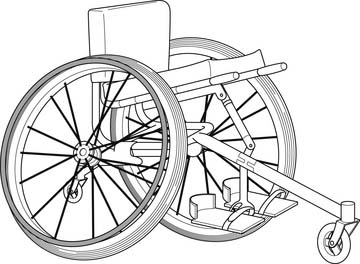
The standard wheelchair (Figure 17-1) is designed for short-term, hospital or institutional use and should not be recommended for the patient to use as a personal wheelchair. As noted in Table 17-1, these can be rather heavy with limited sizes available. Figure 17-1 also illustrates the basic components of a wheelchair. The standard wheelchair folds for easy storage and transportability. A “hemi” wheelchair is essentially a standard wheelchair with a lower seat-to-floor height for persons of shorter stature or who use one or both feet for propulsion. A lightweight wheelchair is slightly lighter in weight but with limited sizes. The first three models have few adjustable parts (some models have no adjustable parts) and generally have sling-type upholstery. Sling upholstery has no capacity to provide pressure relief, and the hammock effect that occurs from wear causes uncomfortable and unstable inward rotation of the hips. However, many users have been sitting in a sling seating system for years and have become accustomed to the hammock effect for comfort. Making the switch to a seating system that supports their posture better can be both frustrating and uncomfortable for these users.
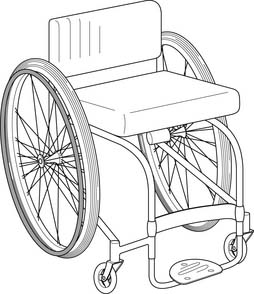
The high-strength lightweight and ultralight wheelchairs are designed for long-term use by individuals who spend more than a couple of hours each day in a wheelchair. They have adjustable features, especially the ultralights. There are many advantages to using ultralight wheelchairs over the other wheelchair types. These are highlighted in the following sections that discuss selecting the appropriate seat dimensions, setting up the wheelchair, propulsion mechanics, and transportability. An ultralight wheelchair is depicted in Figure 17-2.
The last two classes of manual wheelchairs listed in Table 17-1 pertain to persons who weigh more than 250 lb. These wheelchairs are heavier than the wheelchairs in the other classes, to support more body weight. These categories are also outdated because of the increasing number of persons with disabilities who are overweight or obese and need wheelchairs. This trend has resulted in an expanded class of “extra–heavy-duty” wheelchairs, referred to as bariatric wheelchairs, which are built to support individuals who weigh between 300 and 1000 lb.
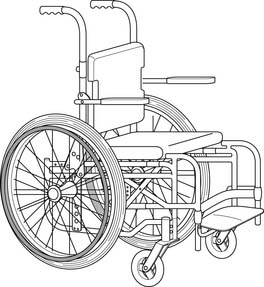
Pediatric manual wheelchairs are similar to the adult wheelchairs but are smaller (seat width or depth <14 inches). Many of these wheelchairs have adjustable frames or kits for accommodating the growth of the child (Figure 17-3). If the child is unable to self-propel the chair, a powered mobility device might provide independent mobility.37 Strollers equipped with a wide range of seating options (Figure 17-4) can also be used to transport children with orthopedic deformities.

Sports wheelchairs are designed specifically for participating in such athletic endeavors as racing, rugby, tennis, and basketball. These wheelchairs are made of lightweight materials, and usually have very aggressive axle positions and camber. Some of the sport wheelchairs have only one wheel in the front, which allows quick turns and enhanced maneuverability (Figure 17-5). Wheelchairs equipped with arm crank mechanisms (called hand cycles) for exercise are available from many manufacturers. Arm crank exercise can help improve cardiovascular fitness, with research showing that arm cranking is more efficient and less of a physical strain than conventional wheelchair propulsion.33
Basic Wheelchair Dimensions
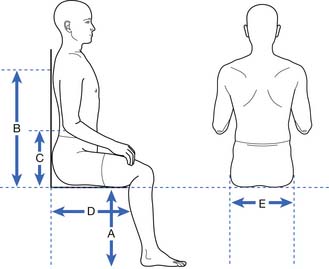
Figure 17-6 shows the measurements that should be taken of the patient’s body for determining wheelchair dimensions. These dimensions are required not only for determining the correct manual (or power) wheelchair size, but also for determining seating system sizes (e.g., cushion, back supports, leg rest lengths).
Seat Height
The seat should be just high enough to accommodate leg length while leaving enough space under the foot rests (about 2 inches or so) to clear obstacles.3 Persons with longer legs often need angled or elevating leg rests that extend the legs slightly outward instead of straight down (knee angle of 90 degrees). This is needed to allow them to get their knees underneath tables. It is more difficult to do if the patient has tight hamstrings. The height of the seat should be adjusted so that the person has enough knee clearance to fit under tables, counters, and sinks at home, at work, at school, and in the community (the Americans with Disabilities Act mandates at least 27-inch-high knee clearance under tables and surfaces). Seat height is also an important consideration for persons who drive while seated in the wheelchair and need to be able to access the steering wheel or hand controls.
Seat Depth
The depth of the seat provides support for the thighs. A seat that is too shallow causes higher sitting pressures because less of the seat is in contact with the thighs. A seat that is too deep can cause excess pressure behind the knees and calves. There can also be a tendency for the pelvis to slide into a posterior tilt so that the back can be adequately supported by the backrest. A 1- to 2-inch gap between the popliteal area and front edge of the cushion is recommended, but might need to be more if the person propels with the feet.3
Back Height
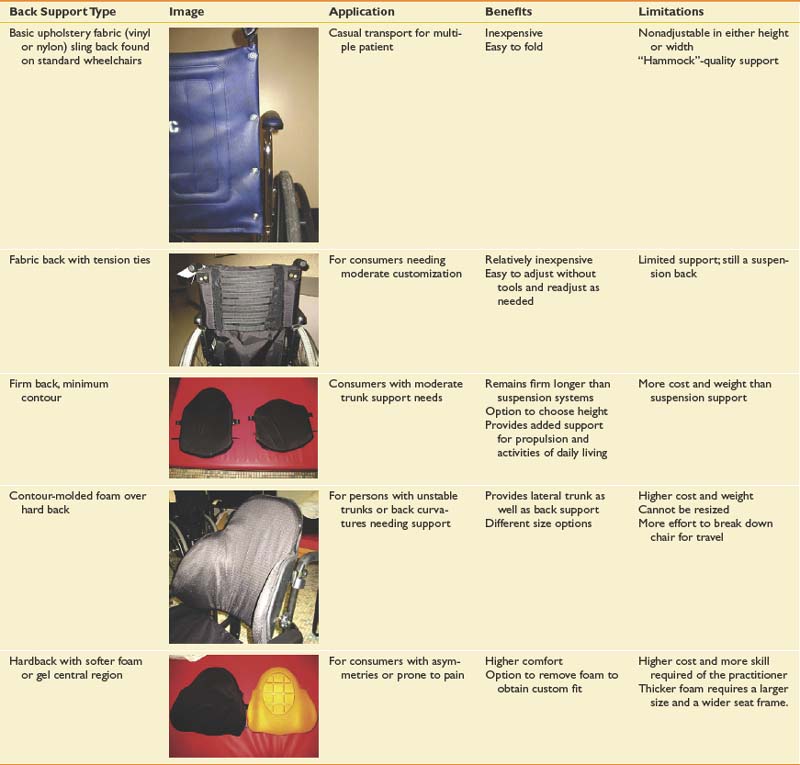
The height of the back is determined by the amount of postural support the person needs. The backrest should be low enough to provide adequate support, but still allow the upper limbs access to as much of the pushrims as possible. Many practitioners use the inferior angle of the scapula as a basis for determining backrest height. The backrest height should be below the inferior angle so that it does not impede arm movements. There are various kinds of back supports (Table 17-2), and some have a tapered area that allows for greater freedom of scapular movement. Only the high-strength lightweight and ultralight wheelchairs permit the attachment of different kinds of back supports.
Manual Wheelchair Setup
Ultralight wheelchairs provide the highest degree of adjustability. This makes it possible to optimize the fit of the wheelchair to the user, which is likely to have a positive impact on propulsion mechanics. In addition to the basic adjustments that can be made on most other wheelchairs (e.g., footrests, armrests), ultralight wheelchair adjustments also allow for adjusting the seat and back angle, rear wheel camber, and rear axle position.
Rear Wheel Camber
Camber is the angle of rear wheel tilt. Zero degrees of camber implies that the rear wheels line up vertically and with the side of the wheelchair. Angling the rear wheels so the top is tilted inward and the bottom outward (see Figure 17-5) results in increased camber and distance between the rear wheels. Most wheelchairs generally have up to 8 degrees of camber. Although more camber is usually possible, it can impede the ability to enter and exit doors and openings. Box 17-2 lists the advantages and disadvantages of camber.
Horizontal Axle Position
Moving the axle forward moves the seat back relative to the rear wheels. This results in a shift of the user’s weight to over or slightly behind the rear axles.9 A more forward axle position requires less muscle effort because rolling resistance is lowered when more weight is distributed over the larger rear wheels than the smaller front casters.31 This position also facilitates “popping a wheelie,” negotiating obstacles, and ascending or descending curbs. In contrast, moving the axle forward can make the wheelchair more “tippy” and difficult to push up a ramp because of the tendency to tip backward. For this reason, wheelchairs are usually delivered with the axle in the most rearward position possible. This position usually needs to be changed, based on input from the patient and the practitioner. An antitipper (Figure 17-7) can help prevent rearward falls; but might also make it more difficult to negotiate a curb and pop a wheelie. Because of the effects on stability, the axle should be moved forward incrementally, provided the wheelchair user feels stable. Adding weight to the chair can also affect stability.27 This is why packages or backpacks ideally should be located underneath the seat of the chair.

Vertical Axle Position
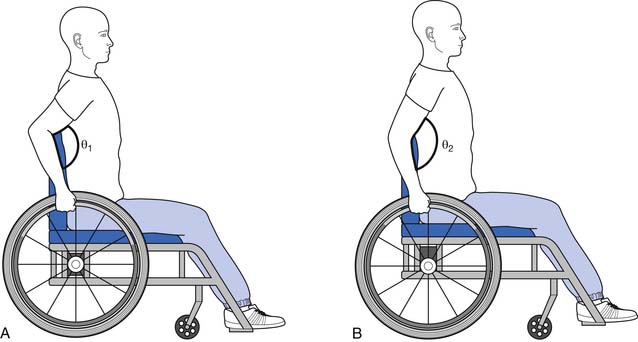
Raising the axle has the effect of lowering the seat, while lowering the axle raises the seat. A lower seat position can improve propulsion biomechanics by increasing hand contact with the pushrim,5,44 lowering stroke frequency,5 and increasing mechanical efficiency.44 Lowering the seat height also increases the stability of the wheelchair. If the seat height is too low, however, the patient has to push with the arm abducted. This can increase the risk of shoulder impingement, another upper limb injury common among manual wheelchair users. The ideal seat height is the point at which the angle between the upper arm and forearm is between 100 and 120 degrees when the hand is resting on the top and center of the pushrim (Figure 17-8, A).5,44 An alternative method that can be used to approximate the same position and angle is to have the individual rest with their arms hanging at the side. The fingertips should be at the same level as the axle of the wheel. If the seat height is too high, less of the pushrim can be accessed and more strokes are needed to go the desired speed (Figure 17-8, B).
Wheelchair Propulsion
Wheelchair Weight
The weight of the wheelchair is an important consideration, especially when prescribing manual wheelchairs. Less propulsive force is needed to push a lighter wheelchair. Ultralight wheelchairs have frames and components made with materials having high strength-to-weight ratios, so less material is needed. One study directly compared ultralight and standard wheelchairs, and found that ultralight wheelchair users pushed at faster speeds, traveled further distances, and used less energy.4 The reduction of force is even more important on inclines where gravitational forces add to the rolling resistance. A light wheelchair is also easier to load into and out of a vehicle.
Quality of the Wheelchair and Setup
Ultralight wheelchairs have better components and are less likely to become misaligned with use, which helps minimize rolling resistance. Keeping the chair in good alignment might require other adjustments, such as to the brakes or caster alignment or height. Axle tubes on rigid ultralight frames can eliminate many of these problems. As discussed previously, a wheelchair that fits the user and is optimized for propulsion by adjusting the axle position makes it easier to push the wheelchair. Lowering stroke frequency and forces through a combination of propulsion training, wheelchair setup, and proper choice of wheelchair can protect the median nerve from injury.7 Instrumented wheels used in prior research15,36 are now available commercially for clinicians to use to objectively evaluate the quality of wheelchair setup and propulsion techniques.
Propulsion Technique
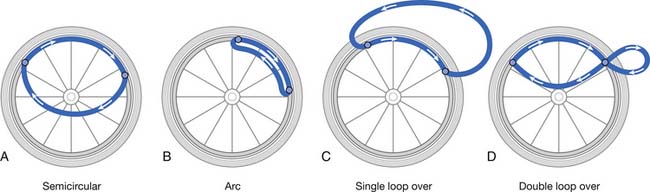
The propulsion techniques of manual wheelchair users have been examined in detail.6,38,40,46 Propulsive strokes are generally described in two phases: when the hand is in contact with the pushrim applying forces (push phase), and when the hand is off the rim and preparing for the next stroke (recovery phase). Four distinct propulsion patterns have been identified, which are defined by the path the hand takes during the recovery phase: arc, semicircular, single-looping over, and double-looping over (Figure 17-9). The single-looping over form of propulsion, which consists of having the hand above the pushrim during recovery, is the most prevalent pattern in individuals with paraplegia.6 However, the semicircular pattern, in which the user’s hand drops below the pushrim during recovery, has better biomechanics (see Figure 17-9, A). The semicircular pattern has been associated with lower stroke frequency and greater time spent in the push phase relative to the recovery phase.6 The semicircular pattern is preferred because the hand follows an elliptical pattern, with no abrupt changes in direction and no extra hand movements. By applying forces to the pushrim in smooth, long strokes, the same amount of energy is imparted to the rim without high peak forces or a high rate of force loading. For example, a long stroke (see Figure 17-9, A), as opposed to a short stroke (see Figure 17-9, B), is likely to minimize the number of strokes needed to push at a desired speed.
Manual Wheelchair Transportability
There are basically two types of manual wheelchair frames: folding and rigid. Folding frames allow the wheelchair to collapse for storage (see Figure 17-1). Rigid frames are mainly available for ultralight wheelchairs (see Figure 17-2) and for wheelchairs with special positioning aids (e.g., tilt or custom seating systems). Rigid frames tend to be more durable than folding because there are fewer moving parts. Fewer moving parts also mean that rigid frame wheelchairs tend to be lighter. The backrests on rigid frames are designed to fold down for improved compactness. A “quick-release” axle allows for easy removal of the wheels on rigid frames and certain folding frames. This option is not available on standard and some lightweight wheelchair models.
Manual Wheelchair Components and Accessories
Refer also to the discussion on seating and positioning.
Wheels and Tires
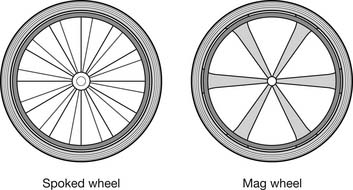
There are several factors to consider when choosing the most suitable wheel and tire configuration for a wheelchair including type of indoor or outdoor terrain, activity level, maintenance, weight, and cost. Many standard and lightweight wheelchairs come equipped with either mag-style or spoked wheels (Figure 17-10). Mag wheels are made from composite plastics or metal (initially they were made from magnesium, hence the term mag). They are usually heavier than spoked wheels but are more durable and require less maintenance. Newer types of mag wheels are composed of high-strength lightweight materials and can even be lighter than spoked wheels, but are more costly. Spoked wheels have a tendency to get out of alignment (wheel wobbles when spun), requiring a trip to a bicycle shop or a wheelchair dealer for the wheels to be trued.
Grade Aids
Grade aids are devices that attach to the frame and are used for persons who have difficulty with slopes and have a tendency to roll backward down hills. These devices only prevent the wheelchair from rolling backward, and forward motion is unimpeded.
Pushrims
Pushrims are available in different sizes, shapes, and surface finishes. The pushrim most commonly found on wheelchairs is about ½ inch in diameter with a smooth surface finish and round cross-sectional area (see Figure 17-1). Persons who have limited gripping ability (e.g., low-level cervical injuries) might need a larger diameter pushrim or a high-friction surface finish (e.g., vinyl or foam), or both. Sometimes these individuals need a pushrim with vertical, horizontal, or angled projections (Figure 17-11, A) to be able to effectively propel their wheelchairs. New designs provide for greater surface area (Figure 17-11, B) and are also contoured for a more natural hand grip.

Lever Drives
Propelling the wheelchair using levers versus pushrims has proven to be more mechanically efficient. Dual-lever drive wheelchairs are more common in Europe, China, and other countries of the Far East. They are well suited for persons who frequently propel long distances and over outdoor terrain (e.g., dirt roadways). The drawbacks to using a lever drive system include difficulties with maneuvering in tight places, transfers, and transportability. Single-lever drive systems are quite popular in the United States and allow for the wheelchair to be propelled using one arm (Figure 17-12).

Antitippers
Antitippers are devices that attach to the rear of the wheelchair frame and usually have adjustable length tubes with small wheels at the end (see Figure 17-7). These devices protect the user from tipping the wheelchair backward, but can make it difficult for the user to ascend a curb or pop a wheelie. The tube length can be adjusted to allow the user to traverse over small obstacles while still providing some stability. All new manual wheelchairs generally come equipped with antitippers; however, high-end users often remove them after receiving the wheelchair.
Geared and Power-Assisted Wheelchairs
Geared and power-assist devices are appropriate for individuals who use or prefer their manual wheelchairs for mobility, but who need some assistance to reduce the physical effort required to self-propel. These devices are particularly likely to help those with muscle paralysis or weakness, overuse, and fatigue. They are also ideal for individuals who are apprehensive about transitioning to a fully powered wheelchair. This can be due to not wanting to be viewed by peers as being “more disabled,” having homes that do not accommodate the increased size, lacking the financial resources, or having difficulties with transportation. A geared wheelchair does not require batteries and works similar to a bicycle, allowing the user to shift into a lower gear when climbing hills or rolling over uneven or rough terrain. Power-assist devices include stand-alone powered units that are external to the wheelchair and that the wheelchair user holds on to. Another is a power add-on device that attaches to the wheelchair and has a steering mechanism or input device for controlling the wheelchair. Figure 17-13 shows a pushrim-activated system with motors in the wheelchair hubs. Geared and power-assist devices cost less than a fully powered wheelchair system, but require that the individual has a manual wheelchair that is compatible with the power-assist device.

Research has shown that using a geared or pushrim-activated wheelchair results in significant reductions in the physical and physiologic demands of propulsion compared with using a manual wheelchair.11,22 Power-assist devices can increase the width or length of the manual wheelchair base a few inches. Both geared and power-assist devices are more difficult to transport than manual wheelchairs, mainly because the equipment adds between 10 and 50 lb to the wheelchair. This is still considerably lighter, however, than a fully powered wheelchair.
Power Wheelchairs
People who do not have the strength or stamina to propel manual wheelchairs typically need power wheelchairs for mobility independence. Power wheelchairs can be grouped into four broad categories based on wheelchair features and their intended use: (1) conventional power wheelchairs; (2) folding and transport power wheelchairs; (3) combination indoor-outdoor power wheelchairs; and (4) heavy-duty indoor-outdoor power wheelchairs.19
Conventional Power Wheelchairs
Conventional power wheelchairs are not programmable (e.g., no adjustments in acceleration or deceleration, turning speed, joystick sensitivity) and have very basic seating with limited sizes available (Figure 17-14). They are low cost and low quality (see the duscussion of wheelchair standards). They are appropriate for limited indoor use for individuals with good trunk control who do not need specialized seating.

Folding and Transport Power Wheelchairs
Folding and transport power wheelchairs are designed for easy disassembling to facilitate transport (Figure 17-15). They are usually compact for indoor use and have a small footprint (i.e., area connecting the wheels) for greater maneuverability in confined spaces. They might not, however, have the stability or power to negotiate obstacles outdoors. The batteries are often housed in separate boxes having easy-to-separate electrical connectors. These wheelchairs are typically used by individuals with reasonably good trunk and upper body control.

Combination Indoor-Outdoor Power Wheelchairs
Combination indoor-outdoor power wheelchairs (Figure 17-16) are often purchased by people who wish to have mobility indoors (home, school, work) and in the community, but who stay on finished surfaces (e.g., sidewalks, driveways, flooring). These wheelchairs are equipped with standard proportional joysticks and standard programmable electronics (e.g., speed adjustment, tremor dampening, and acceleration control). They come with either standard seating (such as that shown in Figure 17-17) or rehabilitation seating (see Figure 17-16). Rehabilitation seating allows for the attachment of modular seating hardware (e.g., backrests, cushions, laterals, hip guides, and headrests).


Heavy-Duty Indoor-Outdoor Power Wheelchairs
Heavy-duty indoor-outdoor power wheelchairs (Figure 17-18) are for use by people who live in communities without finished surfaces. These wheelchairs usually have large-diameter drive wheels with heavily treaded tires or four-drive wheels for climbing obstacles and traversing rough terrains. Wheelchairs that can support persons who weigh more than 250 lb also fall under this category. These wheelchairs usually weigh 300 to 500 lb.

Power wheelchairs typically use two deep-cycle lead-acid batteries in series, each producing 12 V, for a total of 24 V. There are two types of lead-acid batteries: wet-cell batteries and gel-cell batteries. Gel-cell lead-acid batteries are generally recommended because there is no potential for chemical spills and they are maintenance free.
Power Wheelchair Base Selection
Rear-Wheel Drive
Rear-wheel drive is characterized by large drive wheels in the rear and small pivoting casters in the front (Figure 17-19). The rear-wheel drive power wheelchair steers and handles predictably, and naturally tracks straight, making it is the most appropriate drive configuration for high-speed applications. Additionally, because of its consistent tracking, it is preferred by people who drive with special input devices (chin joystick, head array, etc.) or have reduced fine motor coordination. The disadvantages of this configuration include limited obstacle climbing by the small front casters. It also has the largest turning radius among the three configurations.

Front-Wheel Drive
The front-wheel drive power wheelchair features large drive wheels in the front and small pivoting casters in the rear (see Figure 17-17). It is a very stable setup for uneven terrain and hills. Of the three configurations, it has the best capability to climb forward over small obstacles. The overall turning radius is smaller than that of rear-wheel drive, but larger than that of the midwheel drive power base. However, the front-wheel drive power wheelchair has a tendency for the back of the chair to wander side to side (“fishtailing”), especially with increased speeds. This directional instability requires steering corrections, which could make the wheelchair difficult for some users to steer.
Midwheel Drive
The midwheel drive power wheelchair (see Figure 17-16) has been one of the fastest growing power bases in the wheelchair industry. In this configuration the drive wheels are located near the center of the power wheelchair, allowing the user to seemingly turn on center, dramatically increasing indoor maneuverability. With the drive wheels directly under the user, traction is also increased, and with the use of suspended front antitip wheels, the midwheel drive can be among the most effective at both ascending and descending obstacles for skilled, practiced users. One of the concerns, however, is that when riding on uneven terrain or up and down curb cuts with a steep transition, there is a possibility of getting “stuck” on the front or rear casters. This can suspend the drive wheel in midair with no contact with the ground.
Input Methods
The interface between the wheelchair user and the wheelchair itself is often the most critical component of a power wheelchair. A safe, consistent, and reliable method of accessing powered mobility can sometimes be the most difficult step in wheelchair assessment and evaluation.8 Newer plug-and-play technology allows clinicians to let users try different input devices during the evaluation. This technology also allows the input device to be changed without having to replace the electronics or wheelchair as the client’s medical condition changes.
There are different types of input methods for operating a power wheelchair. Commercially the most common available control interface between the user and the wheelchair is a joystick (Figure 17-20).

Proportional Control Versus Switched Control
A joystick can be either proportional control or switched control. Proportional control is usually the optimum solution for wheelchair control because it provides continuous adjustment of speed and direction. If the user does not have the fine motor skills necessary for reliable control of a proportional joystick, a switched control joystick could be chosen. Switched control joysticks respond to discrete positions of the joystick and usually have eight driving directions. These directions typically are forward, reverse, left and right, and the four diagonal directions. Speed is not directly controllable by joystick position when the joystick is configured to act like a switch. For users with limited fine motor control, the switched control joystick can be mounted on a wheelchair and positioned to operate by chin, head, shoulder, elbow, arm, knee, foot, or tongue. Joysticks can be ordered in various sizes (e.g., “mini” for small movements) and with different handles (e.g., round, oblong, goalpost shaped).
Position-Sensing Versus Force-Sensing
For proportional control a joystick can use either the position-sensing or force-sensing method. The control output from a position-sensing joystick is proportional to the deflection of the joystick from a neutral position. A change in electrical resistance or inductance can be used to signal the position of the joystick. The control output from a force-sensing joystick is proportional to the force exerted on the stick by the user.18 A strain gauge bridge is usually instrumented to the joystick shaft to measure forces. Force-sensing joysticks could be effective for individuals with tremors, spasms, and limited range of motion.
Sip and Puff
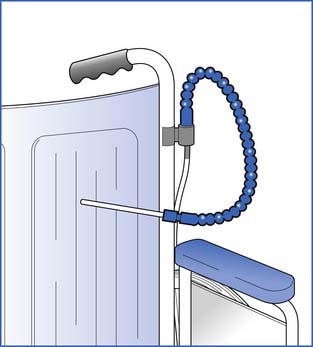
A sip-and-puff input device allows control of the wheelchair by sipping (breathing in) and puffing (breathing out) on a straw located near the mouth (Figure 17-21). Generally a user will sip a specific number of times to indicate a direction, and puff to confirm the choice and activate the movement of the wheelchair.
Integrated Controls
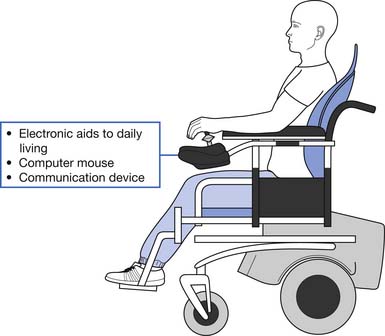
Wheelchair input devices are used for controlling both wheelchairs and electronic aids to daily living or computers. When a single control interface (e.g., joystick, head switches, voice recognition system, or keypad) is used to operate two or more assistive devices, the system is called an integrated control system (Figure 17-22).20 While integrated control is beneficial, if the input device is broken, users can lose access to every operation mode. Using an integrated controller might require additional training.
Programmability
The maximum speed of power wheelchairs varies significantly among different manufacturers and models. Wheelchairs are typically tuned to higher speeds when they are used outdoors. A slow mode of operation is needed for maneuvering indoors. Braking or deceleration is another critical adjustment for maintaining a safe position for users in the wheelchair. An extreme hard setting can cause users to be thrown forward when they release the joystick, while an extreme soft setting can cause the wheelchair to coast and not stop in time to avoid an obstacle. The sensitivity of an input device can compensate for physical limitations or unintentional movements of users so that they have full and safe control over the devices.
Scooters
A scooter is designed to provide intermittent mobility support for individuals with good arm strength, trunk balance, and ability to transfer in and out of the device. Scooters typically have motors in the back and are steered with a tiller (which looks and acts like the handlebar on a bicycle). The tiller can be tilted forward or back and locked at any desired position. Thumb levers are used to drive the scooter. Scooters are usually equipped with automatic braking (similar to power wheelchairs), and are not able to coast. Three-wheeled scooters (Figure 17-23) are more common than four-wheeled scooters (Figure 17-24), which can traverse more rugged terrain but are large for most indoor settings. Compared with power wheelchairs, many scooters are relatively easy to disassemble for storage in a car or trunk. Scooters also cost lesser than a typical power chair.


Stand-Up Wheelchairs
Stand-up wheelchairs offer a variety of advantages over standard wheelchairs. The ability of a person to achieve an almost vertical position has several advantages, including physiologic (i.e., pressure relief, improved circulation and digestion, and improved bone density), practical (i.e., improved reach to higher surfaces, which increases functional independence), and psychological (i.e., interacting with colleagues face to face) (Figure 17-25).1

Stand-up wheelchairs are more complex than most manual or power wheelchairs. All power wheelchairs with a stand-up feature use a separate electric drive system for the stand-up mechanism. Manually powered stand-up wheelchairs use a manual lifting mechanism or an electric-powered lifting mechanism. When in the elevated position, this type wheelchair has a very high center of gravity and can easily topple over. For this reason the user of a stand-up wheelchair should never transition into a stand-up position when outdoors or when on a cracked, rough, or broken floor indoors. Stand-up wheelchairs are safe only on perfectly flat and smooth flooring, and only if the user is properly strapped and secured to the seat and seat back. People who have not stood for a long time might not have the hip, knee, or ankle range of motion to accommodate standing, and can experience orthostatic hypotension. The stand-up mechanism also adds weight to the wheelchair, making it more difficult to lift and transport.
Alternative Powered Mobility Systems
The Segway Personal Transporter is a small motorized vehicle with a step-up platform (Figure 17-26). The rider stands on the platform, grips a vertical tiller, and controls the direction and speed of the Segway by leaning. The Segway was introduced in late 2002 with a primary intent to serve individuals in walking-intensive occupations (e.g., police foot patrols, mail carriers, and warehouse work). It is not a Food and Drug Administration (FDA)-approved device, nor is it being promoted as a form of wheeled mobility for individuals with disabilities. However, research supports considering the Segway as a potential alternative form of mobility to a wheelchair for individuals who are able to stand but have limited ambulation (e.g., persons with lower limb amputation, burns, mild traumatic brain injury, incomplete spinal cord injury, or multiple sclerosis).39 The Independence 4000 IBOT Transporter is an FDA-approved device based on similar technology as the Segway with multiple functions (e.g., stair and curb climbing ability), but accommodates individuals who are unable to stand and ambulate. Its high cost, large bulk (289 lb), and limited rehabilitation seating offerings dampened its market potential, and the company decided in early 2009 to stop manufacturing the device.

Power Wheelchair Transportation
Ramps
Ramps are the inexpensive alternatives to vehicle lifts.42 They can be portable or mounted inside the vehicle (nonpowered or powered), or integrated into the frame of the vehicle. They are usually installed on the side or at the rear of the vehicle, and have either a single track or double track with a nonslip surface. With powered ramps a remote entry button opens the door and extends the ramp. Vehicles having powered ramps (Figure 17-27) can also have a “kneeling” feature that lowers the vehicle before extending the ramp to accommodate for ramp slope needs. Selection of a ramp is based on the size and weight of the user and wheelchair. Also, the user’s ability to push or drive up a ramp is usually a concern when choosing between ramps and lifts.

Lifts
For wheelchair users using personally owned vehicles, a vehicle equipped with an automatic lift can eliminate problems loading and unloading the wheelchair and provide easy transportation for nonfolding wheelchairs and heavy powered wheelchairs. There are also automated systems for eliminating difficult or awkward transfers into and out of the vehicle.
A platform lift (Figure 17-28, A) folds out from the van similar to a drawbridge, and requires perpendicular access to load or unload a wheelchair. It also uses minimal storage space within the van, folding upright against the door. When using a pull-in type of parking space, the equivalent of two parking spaces (8 to 10 feet) is needed to lower the platform lift and load or unload a wheelchair. A platform lift can also be installed on the rear door of the van, but this often requires loading or unloading the wheelchair in a traffic lane. Rear door mounting also eliminates the use of space for extra passenger seats.

An overhead strap lift (Figure 17-28, C) uses an arm with nylon straps that attach to several points on the wheelchair and hook onto the arm of the lift. The lift has no platform and uses little storage space in the van. The wheelchair is loaded and unloaded perpendicular to the van, but less space is required because there is no platform to lower.
Several systems are available to ease transfers to the driver or passenger side seats. These systems provide a motorized option that allows for lowering and raising either the vehicle seat itself (Figure 17-28, C) or a platform that extends out from the vehicle (Figure 17-28, D) that the person can transfer to first. These systems usually do not require structural modifications to the vehicle and enable a safer and easier transfer because the surface the person is transferring to can be set at the same height as the wheelchair seat. Transferring to a higher surface is more difficult and strenuous because it requires greater force and range of motion to overcome the effects of gravity and should be avoided when possible. These system also allow for aligning the seat next to the wheelchair, reducing the space separating two surfaces, which further assists with transfers. For manual wheelchair users who are independent and drive, one potential solution would be to combine a transfer system with an overhead strap life that attaches to side door opening of a van that can lift and stow the wheelchair behind the driver’s seat (Figure 17-28, E).
To secure a wheelchair and its occupant in a moving vehicle, both the occupant restraint and the wheelchair securement must act together as an integral crash protection system for the user. There are essentially two basic securement approaches: attendant-operated securement systems and mechanical latching or docking devices. The attendant-operated type is the recognized industry standard, dominated by the four strap–type system that attaches to the wheelchair frame. Use of docking securement devices is currently limited mainly to private vehicle applications, primarily because of the need to match wheelchair securement geometry with vehicle anchorage geometry.45
Tie Downs and Securement
If a wheelchair user is going to remain in a wheelchair while riding, special tie-down or restraint systems for the wheelchair and the occupant must be used for safety. Wheelchairs are not designed to withstand crash-level forces like automobile seats are, and can be tipped over easily by even a minor collision or sudden braking of the vehicle. A tie-down system with an occupant restraint as well as wheelchair anchorage provides the best protection (Figure 17-29, A). A typical four-point restraint system has four webbing straps that are secured to the main frame of the chair. The preferred angles for rear wheelchair tie down are between 30 and 45 degrees to the horizontal plane. The preferred angles for front tie down are between 40 and 60 degrees to the horizontal plane. The wheelchair tie-down system only stops the chair from tipping or moving; it does not stop the occupant from being thrown out of the wheelchair in a collision. In addition to the four-point wheelchair restraint system, a pelvis belt is usually used as the occupant restraint. A properly positioned pelvis belt can prevent an occupant from being ejected from the vehicle. In addition, a shoulder belt fixed to the side wall of a vehicle can provide an upper torso restraint. It can reduce chest and head excursions in a crash environment.10 Although the four-point, strap-type securement system has been shown to be one of the most effective and versatile methods for securing a wide range of wheelchairs, it is also a system that is difficult and time-consuming to use.
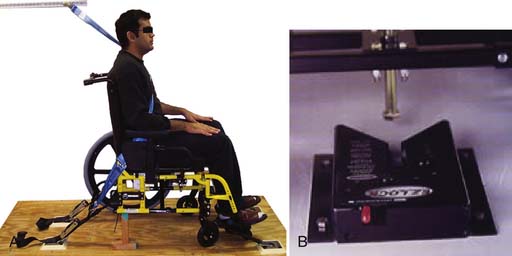
FIGURE 17-29 Wheelchair tie-downs and securement. (A) Wheelchair and occupant restraint system. (B) Wheelchair docking system.
A docking system (Figure 17-29, B) is another type of wheelchair restraint system. For example, the EZ Lock wheelchair restraint system is a simple and effective docking system to secure an occupied wheelchair in a moving vehicle. The automatic locking mechanism simply requires that the occupant guides the wheelchair over the top of the lock until the interface on the wheelchair is fully engaged. A conveniently located push-button switch is used to release the wheelchair from the system. A dock-type restraint system requires matching components, one attached to the wheelchair frame and the other to the vehicle. The advantages are that it is quick and easy to operate, and offers increased user independence. However, it relies on having a location on the wheelchair frame to which one component of the securement system can be attached. It is also two to five times as expensive as standard belt restraint systems. Docking devices have been shown to work reasonably well for private (rather than public) vehicles in which the matching components can be individually configured to the specific wheelchair and vehicle. This has yet to happen in public vehicles that must be able to accept any wheelchair to be universally applicable.
Wheelchair Standards
Wheelchair standards were developed to provide a means to objectively compare the durability, strength, stability, and cost-effectiveness of commercial products. Wheelchair standards are voluntary in the United States, but the test results are accepted by the FDA, which approves commercial marketability of the device. Most countries have adopted the International Organization for Standardization (ISO), which acts to continually develop and refine wheelchair standards. The American National Standards Institute (ANSI) and the Rehabilitation Engineering and Assistive Technology Society of North America (RESNA) are member organizations of ISO for the United States.
Manual Wheelchair Performance
Ultralight wheelchairs have been shown to last about 13 times longer than standard wheelchairs and cost about three and a half times less to operate.11 Ultralights lasted about five times longer and cost approximately two times less to operate than lightweight wheelchairs.12 When tested to failure, ultralight wheelchairs had the longest survival rate and fewer catastrophic failures in comparison with standard and lightweight wheelchairs.23 Using wheelchairs that are less prone to failure is safer for individuals.26,43 Ultralight models with suspension elements incorporated into the frame, the castors, or both, perform similarly to lightweight wheelchairs with respect to wheelchair durability and cost-effectiveness.29 Models in which the frame and parts are composed of titanium metal offer the lightest possible option in the ultralight category, and have other advantages such as anticorrosive properties and a smoother ride. However, manufacturers are not as experienced yet working with titanium as they are with aluminum. Titanium ultralights have failed to meet the minimum number of cycles for passing the fatigue test.30 Improvements in the design and manufacturing techniques of titanium wheelchairs are necessary to increase their durability and cost-effectiveness, since wheelchairs made with titanium cost more than those made with aluminum.
Power Wheelchair Performance
Component failures and engineering factors are responsible for 40% to 60% of the injuries to power wheelchair users.24,26 Power wheelchairs undergo all the same tests as manual wheelchairs, and also have a series of tests on the power and control systems and batteries.
Power wheelchair test results indicate that heavy-duty indoor-outdoor models perform better than the other categories of power wheelchairs in terms of durability (total equivalent cycles on the double-drum machine).21 Conventional power wheelchairs performed the worst in several areas (poorer durability and reliability, dynamically unstable, and prone to wiring failures).34 It is important to look at the test results in each area in relation to what is important to the individual. For instance, a wheelchair might outperform others in terms of durability but have poor static and dynamic stability results. If durability is an important factor (most health insurance companies limit the patient to one wheelchair per 5 years), the user might choose to sacrifice the wheelchair’s performance concerning stability. Stability for certain individuals can be a more important factor than durability if the patient has a high risk for falling from the wheelchair or frequently traverses up and down steep ramps.
Power wheelchairs perform similarly to ultralight wheelchairs in terms of their durability.21 In regard to value, power wheelchairs are more costly than ultralight and lightweight manual wheelchairs. They are, however, more economical than standard wheelchairs, considering how long they last, the number of repairs, the cost of repairs, and the initial cost of the device. Few test data have been reported on scooters and power-assist wheelchairs. Three-wheel scooters are less stable than power and manual wheelchairs in the lateral direction.35 Power-assisted wheelchairs vary widely in performance depending on the model.25
Seating and Positioning
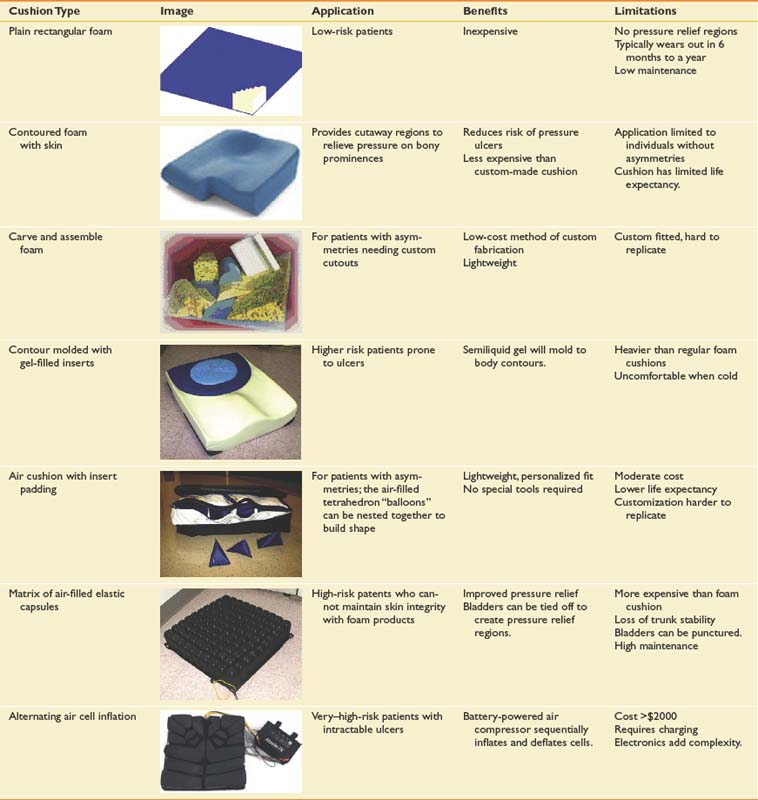
Seat Cushions
Table 17-3 provides an overview of the types of cushions that are commercially available. Commercial cushions are composed of foam, air, gel, or a combination of these materials. If pressure sores remain a problem with these cushions, more aggressive measures must be taken. Alternating pressure cushions are one alternative. These products have a small, battery-powered air compressor and an embedded microprocessor chip that directs the compressed air, alternately inflating multiple air bladders and providing rolling pressure reduction at variable time intervals. Tilt-in-space, recline, or both, can also be used to redistribute weight for more effective pressure relief.
Back Cushions
A well-chosen back cushion should meet the following criteria:
Table 17-2 reviews various types of back supports.
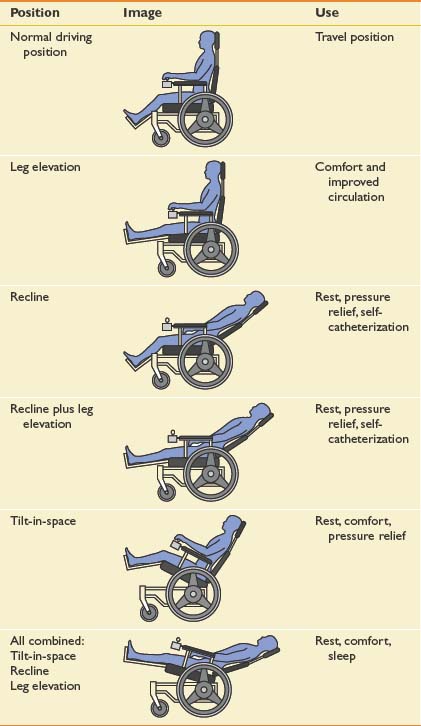
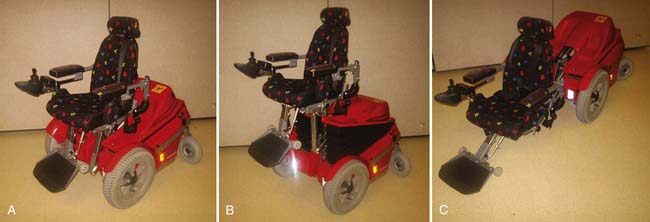
Seat Functions: Tilt, Recline, and Elevation
Tilt and recline are useful for handling complex seating needs through pressure distribution management. If the individual has upper limb weakness or pain that limits independent weight relief (e.g., “push-up” or leaning to the side or forward), a wheelchair equipped with tilt or recline, or both, is needed.17 Seat elevators increase independence, productivity, and social interactions by extending reach capability, enabling and facilitating transfers, and providing peer height at different ages.2 Table 17-4 provides an overview of the seating configurations possible.
Table 17-4 Seating Configurations Possible With Tilt-in-Space, Recline, and Leg Rest Elevation
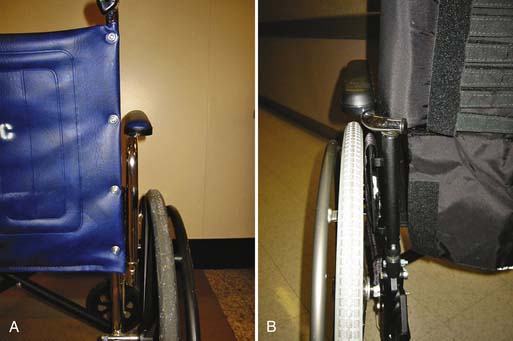
Armrests and Troughs
Standard wheelchairs have narrow armrests covered with fairly firm upholstery. The armrests on standard wheelchairs are integrated with the side frames and cannot be adjusted or removed. A wheelchair for long-term use should provide height-adjustable armrests and the ability to remove them for side transfers. Armrests can be ordered with conventional mounting hardware (Figure 17-30, A) or “space-saving” hardware (Figure 17-30, B), which reduces the overall wheelchair width. Users of ultralight wheelchairs often choose not to have armrests, to improve access to the pushrims for propulsion. Another option found on high-strength or ultralight wheelchairs are tubular armrests that pivot at the rear. These are lightweight and easy to swivel out of the way for desk access and transfers. Individuals using manual and power wheelchairs who need access to desks can order desk-style armrests, which are a few inches shorter in the front section to fit under a table or desk.
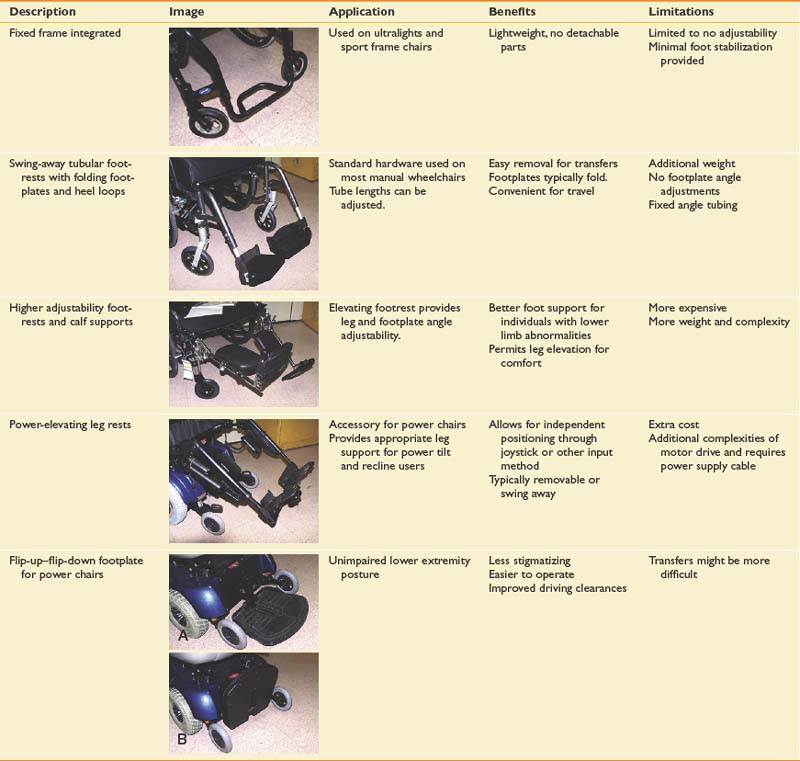
Footrests, Leg Rests, and Foot Plates
Also referred to collectively as front rigging, these components provide support for the legs and feet. If an individual has remaining leg function that can be used to assist the arms in propulsion, the front riggings might need to be removed on one or both sides. For most wheelchairs the front rigging must be quickly detachable to facilitate transfers. Footrests have length adjustments, and models with angular adjustments can be ordered. These allow fitting the footrests to the individual for optimum comfort. Individuals with impaired lower limb circulation and those having a powered recliner often use powered elevating leg rests with calf supports. It is important to consider the tightness of hamstring muscles when evaluating the type of leg rest. Overextending the legs in this case can lead to sacral sitting. Table 17-5 shows examples of various types of front riggings.
Headrests
Seat Belts
Seat belts are typically in the form of a lap belt with a latch similar to those found in motor vehicles. They can help keep the buttocks back in the seat and keep the individual from sliding forward. A seat belt or postural strap, if improperly used, can cause choking. Although many wheelchair users choose not to wear a seat belt, it can help prevent serious wheelchair-related injuries.14
Seating and Mobility Assessment
The following sections describe and discuss the key elements of a wheelchair and seating system assessment, as well as the major variables that need to be considered.
Professionals and Participants
Active participation by the end-user, the family, and/or caregivers in all stages of the seating and mobility assessment is critical. A proper assessment begins with listening to their needs, concerns, and goals for a device. Optimal wheelchair prescription occurs when performed by an interdisciplinary team that includes a physiatrist, occupational therapists or physical therapists with specialty training or certification, and a good working knowledge of wheelchair seating and mobility needs. A rehabilitation engineer also plays an important role in understanding and assessing the capabilities and application of various technologies. A qualified equipment supplier is another important team member to include early in the process, because the supplier is well versed in available devices and how they can be applied to solve problems and address needs. The supplier is also the team member who, in most service delivery models, orders, assembles, and delivers the equipment, and consults with the team regarding securing funding. The RESNA offers certifications for Assistive Technology Professional and Rehabilitation Engineering Technologist. These certifications are for clinicians, engineers, and suppliers who meet certain qualifications and who pass an examination to demonstrate generalist knowledge in the area of assistive technology. A subspecialty certification in the area of seating and mobility is also being developed. RESNA provides a directory of certified professionals (http://www.resna.org).
Physical and Functional Variables
Physical assessments should be followed by observation of performance in ADLs that are reported by the person or the family or caregiver as being essential. These include self-care, reaching, accessing surfaces at various heights, transferring to various surfaces, and functional mobility. Functional mobility should be assessed in the user’s home and community. Ambulation should be assessed from the perspective of the surfaces and distances encountered in a routine day, and whether walking or pushing a manual wheelchair is safe and efficient. When considering manual wheelchair propulsion, stress applied to the upper limbs needs to be considered for manual wheelchair users, because this has been associated with repetitive strain injuries. There is no evidence that upper limb strength correlates with the ability to propel manual wheelchairs, especially when one considers people with cardiac or pulmonary impairments, arthritis, multiple sclerosis, or cerebral palsy.
Obtaining proper seating includes observation of posture in a seat and on a therapy mat table to assess postural alignment and joint range of motion. This can determine what limitations are present and whether they are fixed or flexible. Assessment of pelvic alignment is critical because the pelvis becomes the base of seating support. An obliquity of the pelvis to one side needs to be accommodated or corrected (if possible) to prevent leaning or development of spinal deformities. Likewise, spinal deformities need to be accommodated in the design of the backrest, to allow the user to tolerate sitting. The amount of available hip flexion determines what seat-to-back angle can be tolerated. The degree of knee extension with the hips flexed is important because the hamstrings cross both these joints. Tight hamstrings (common in many wheelchair users) significantly affect the positioning of foot supports. It is important that excessive tension not be placed on the hamstrings because this can be painful and pull the pelvis into a posterior tilt. It is also necessary to respect a person’s preference for different seated postures, even if these postures do not appear appropriate. Humans automatically find different alternative positions to sit to be comfortable, functional, and stable.
Seating Principles
Loss of Sensation
When unimpaired persons sit on hard or irregular surfaces, they rapidly feel discomfort and alter their position to relieve the pressure, or they get up and stretch. If sensation is impaired, the patient can be unaware that a particular contact area is being injured. An inadequate pressure-relieving seating system or technique can ultimately lead to ulcer formation.
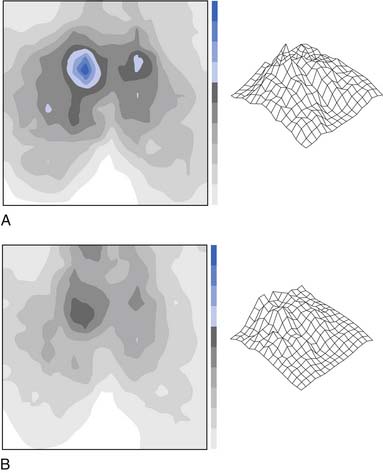
Pressure Mapping as an Assessment Tool
A pressure-mapping device is often used to supplement clinical observations and impressions. This is a thin mat with pressure sensors that can be placed over a surface where the person sits to determine interface pressures. The mat is connected to a computer that produces the topography of pressure that can be displayed on a monitor (Figure 17-31). This can be helpful in comparing the pressure-relieving qualities of various cushions, or to verify the effectiveness of a custom-molded system. Pressure mapping alone should not be the sole determinant for selecting a specific cushion, because there are performance trade-offs with different designs and materials. Other factors need to weigh in the decision, especially user preference. For example, fluid- or air-filled cushions can provide optimal pressure distribution, but might be difficult to slide across for transfers, give the user a sense of instability, or require significant maintenance. Pressure mapping can also serve as a biofeedback method to show the wheelchair user effective weight-shifting techniques.
Manual Wheelchair Versus Power Wheelchair Debate
The feasibility of transitioning from a manual wheelchair to powered mobility is often a significant issue. Manual wheelchair users typically adapt their environment and daily routine around a manual wheelchair. This might include the type of vehicle they use, home and worksite accessibility, transfer methods, or popping wheelies to negotiate curbs. The use of a powered mobility device often requires a significant change in the way ADLs are performed, as well as the need to learn new skills. Other changes include procuring alternative transportation resources, such as using a ramp-equipped van or accessible public transportation, and modifying the home or relocating to a completely barrier-free living arrangement. Clinicians need to recognize these issues and address them appropriately on a case-by-case basis.
Outcome Measures
As with most services in health care, the effectiveness of seating and mobility interventions needs to be demonstrated. To meet this need, standardized outcome measures related to these interventions are evolving. These range from simple but validated self-report questionnaires, such as the Functioning Everyday with a Wheelchair,32 to more involved capacity and performance measures, such as the Wheelchair Skills Test.28 The tools can be administered before the provision of an intervention, yielding a numeric score, which can be compared with scores that are determined after the provision of the intervention.
Considerations for Select Populations
Pediatric
In terms of wheelchair and seating selection, children need the following:
Weight Disparity
Older Adults
Wheelchair-Mounted Accessories: Assistive Technology
Electronic Aids to Daily Living
Because of the postural restrictions imposed by wheelchairs, consumers often have difficulty reaching standard doorknobs, switches, appliances and home entertainment systems, even if they have unimpaired arm function. Seat elevators and stand-up wheelchairs are one solution, but are costly and not always funded by third-party payers. One way to gain increased access to items in the environment is to use wireless electronic aids to daily living (EADL) units. These units operate by transmitting ultrasound, radio frequency or infrared signals to receivers that are connected to the appliance or device to be controlled. Examples of devices include door openers, and controls for lights, television, radio, fan, and thermostat. Some power wheelchairs are equipped with an “EADL” mode so that the individual can operate items directly from their wheelchair (see Chapter 23).
1. Arva J., Paleg G., Lange M.L., et al. RESNA position on the application of wheelchair standing devices. Assist Technol. 2009;21:169-171.
2. Arva J., Schmeler M.R., Lange M.L., et al. RESNA position on the application of seat-elevating devices for wheelchair users. Assist Technol. 2009;21:69-72.
3. Axelson P.W., Yamada Chesney D., Minkel J., et al. The manual wheelchair training guide: Minden. Beneficial Designs: PAX Press; 1998.
4. Beekman C.E., Miller-Porter L., Schoneberger M. Energy cost of propulsion in standard and ultralight wheelchairs in people with spinal cord injuries. Phys Ther. 1999;79:146-158.
5. Boninger M.L., Baldwin M.A., Cooper R.A., et al. Manual wheelchair pushrim biomechanics and axle position. Arch Phys Med Rehabil. 2000;81:608-613.
6. Boninger M.L., Souza A.L., Cooper R.A., et al. Propulsion patterns and pushrim biomechanics in manual wheelchair propulsion. Arch Phys Med Rehabil. 2002;83:718-723.
7. Boninger M.L., Waters R.L., Chase T., et al. Preservation of upper limb function following spinal cord injury: a clinical practice guideline for healthcare professionals. Consortium for Spinal Cord Medicine, Washington, DC, Paralyzed Veterans of America, 2005.
8. Brienza D.M., Angelo J., Henry K. Consumer participation in identifying research and development priorities for power wheelchair input devices and controllers. Assist Technol. 1995;7:55-62.
9. Brubaker C.E. Wheelchair prescription: an analysis of factors that affect mobility and performance. J Rehabil Res Dev. 1986;23:19-26.
10. Chaves E.S., Cooper R.A., Collins D.M., et al. Review of the use of physical restraints and lap belts with wheelchair users. Assist Technol. 2007;19:94-107.
11. Cooper R.A., Fitzgerald S.G., Boninger M.L., et al. Evaluation of a pushrim-activated, power-assisted wheelchair. Arch Phys Med Rehabil. 2001;82:702-708.
12. Cooper R.A., Gonzalez J., Lawrence B., et al. Performance of selected lightweight wheelchairs on ANSI/RESNA tests. American National Standards Institute–Rehabilitation Engineering and Assistive Technology Society of North America. Arch Phys Med Rehabil. 1997;78:1138-1144.
13. Cooper R.A., Robertson R.N., Lawrence B., et al. Life-cycle analysis of depot versus rehabilitation manual wheelchairs. J Rehabil Res Dev. 1996;33:45-55.
14. Corfman T.A., Cooper R.A., Fitzgerald S.G., et al. Tips and falls during electric-powered wheelchair driving: effects of seatbelt use, legrests, and driving speed. Arch Phys Med Rehabil. 2003;84:1797-1802.
15. Cowan R.E., Boninger M.L., Sawatzky B.J., et al. Preliminary outcomes of the SmartWheel Users’ Group Database; a proposed framework for clinicians to objectively evaluate manual wheelchair propulsion. Arch Phys Med Rehabil. 2008;89:260-268.
16. Crane B., Hobson D. No room for discomfort. Rehab Manag. 2003;16:30-35.
17. Dicianno B., Arva J., Lieberman J.M., et al. RESNA position on the application of tilt, recline, and elevating legrests for wheelchairs. Assist Technol. 2009;21:13-22.
18. Dicianno B.E., Spaeth D.M., Cooper R.A., et al. Force control strategies while driving electric powered wheelchairs with isometric and movement-sensing joysticks. IEEE Trans Neural Syst Rehabil Eng. 2007;15:144-150.
19. Dicianno B.E., Tovey E. Power mobility device provision: understanding Medicare guidelines and advocating for clients. Arch Phys Med Rehabil. 2007;88:807-816.
20. Ding D., Cooper R.A., Kaminski B.A., et al. Integrated control and related technology of assistive devices. Assist Technol. 2003;15:89-97.
21. Fass M.V., Cooper R.A., Fitzgerald S.G., et al. Durability, value, and reliability of selected electric powered wheelchairs. Arch Phys Med Rehabil. 2004;85:805-814.
22. Finley M.A., Rodgers M.M. Effect of 2-speed geared manual wheelchair propulsion on shoulder pain and function. Arch Phys Med Rehabil. 2007;88:1622-1627.
23. Fitzgerald S.G., Cooper R.A., Boninger M.L., et al. Comparison of fatigue life for 3 types of manual wheelchairs. Arch Phys Med Rehabil. 2001;82(10):1484-1488.
24. Gaal R.P., Rebholtz N., Hotchkiss R.D., et al. Wheelchair rider injuries: causes and consequences for wheelchair design and selection [see comments]. J Rehabil Res Dev. 1997;34:58-71.
25. Karmarkar A., Cooper R.A., Liu H.Y., et al. Evaluation of pushrim-activated power-assisted wheelchairs using ANSI/RESNA standards. Arch Phys Med Rehabil. 2008;89:1191-1198.
26. Kirby R.L., Ackroyd-Stolarz S.A. Wheelchair safety: adverse reports to the United States Food and Drug Administration. Am J Phys Med Rehabil. 1995;74:308-312.
27. Kirby R.L., Ashton B.D., Ackroyd-Stolarz S.A., et al. Adding loads to occupied wheelchairs: effect on static rear and forward stability. Arch Phys Med Rehabil. 1996;77:183-186.
28. Kirby R.L., Dupuis D.J., MacPhee A.H., et al. The Wheelchair Skills Test (version 2.4): measurement properties. Arch Phys Med Rehabil. 2004;85:794-804.
29. Kwarciak A.M., Cooper R.A., Ammer W.A., et al. Fatigue testing of selected suspension manual wheelchairs using ANSI/RESNA standards. Arch Phys Med Rehabil. 2005;86:123-129.
30. Liu H.Y., Cooper R.A., Pearlman J., et al. Evaluation of titanium ultralight manual wheelchairs using ANSI/ RESNA standards. J Rehabil Res Dev. 2008;45:1251-1267.
31. Masse L.C., Lamontagne M., O’Riain M.D. Biomechanical analysis of wheelchair propulsion for various seating positions. J Rehabil Res Dev. 1992;29:12-28.
32. Mills T.L., Holm M.B., Schmeler M. Test-retest reliability and cross validation of the Functioning Everyday with a Wheelchair Instrument. Assist Technol. 2007;19:61-77.
33. Mukherjee G., Samanta A. Physiological response to the ambulatory performance of hand-rim and arm-crank propulsion systems. J Rehabil Res Dev. 2001;38:391-399.
34. Pearlman J.L., Cooper R.A., Karnawat J., et al. Evaluation of the safety and durability of low-cost nonprogrammable electric powered wheelchairs. Arch Phys Med Rehabil. 2005;86:2361-2370.
35. Rentschler AJ, Cooper RA. A comparison of the dynamic and static stability of power wheelchairs versus scooters. Proceedings of the First Joint BMS/EMBS Conference, Atlanta, October 13-16, 1999. CD-ROM.
36. Richter W.M., Rodriguez R., Woods K.R., et al. Stroke pattern and handrim biomechanics for level and uphill wheelchair propulsion at self-selected speeds. Arch Phys Med Rehabil. 2007;88:81-87.
37. Rosen LE, Arva J, Furumas J, et al: RESNA position on the application of power wheelchairs for pediatric users, Assist Technol 21:218-225, 2009.
38. Sanderson D.J., Sommer H.J. Kinematic features of wheelchair propulsion. J Biomech. 1985;18:423-429.
39. Sawatzky B., Denison I., Tawashy A. The Segway for people with disabilities: meeting clients’ mobility goals. Am J Phys Med Rehabil. 2009;88:484-490.
40. Shimada S.D., Robertson R.N., Bonninger M.L., et al. Kinematic characterization of wheelchair propulsion. J Rehabil Res Dev. 1998;35:210-218.
41. Sie I.H., Waters R.L., Adkins R.H., et al. Upper extremity pain in the postrehabilitation spinal cord injured patient. Arch Phys Med Rehabil. 1992;73:44-48.
42. Storr T., Spicer J., Frost P., et al. Design features of portable wheelchair ramps and their implications for curb and vehicle access. J Rehabil Res Dev. 2004;41:443-452.
43. Ummat S., Kirby R.L. Nonfatal wheelchair-related accidents reported to the National Electronic Injury Surveillance System. Am J Phys Med Rehabil. 1994;73:163-167.
44. van der Woude L.H.V., Veeger D.J., Rozendal R.H., et al. Seat height in handrim wheelchair propulsion. J Rehabil Res Dev. 1989;26:31-50.
45. van Roosmalen L., Bertocci G.E., Hobson D.A., et al. Preliminary evaluation of wheelchair occupant restraint system usage in motor vehicles. J Rehabil Res Dev. 2002;39:83-93.
46. Veeger H.E.J., van der Woude L.H.V., Rozendal R.H. Wheelchair propulsion technique at different speeds. Scand J Rehabil Med. 1989;21:197-203.
[/level-membership-for-physical-medicine-and-rehabilitation-category][not-level-membership-for-physical-medicine-and-rehabilitation-category]
Chapter 17 Wheelchairs and Seating Systems
There is a wide range of choices in wheelchairs. One can choose a wheelchair that is manual, geared, fully powered, power assisted, or standing. There is also an abundance of seating and postural support hardware that can be used to correct or accommodate a wide range of orthopedic deformities and conditions. These include contoured cushions and backrests, tilt-in-space, recline, and custom-molded seating systems. The goals for a wheelchair or seating system are listed in Box 17-1.
Minimize the Risk of Secondary Injuries
Tips and falls account for more than 70% of wheelchair-related accidents.43 It is imperative that individuals be provided with mobility devices that comply with internationally recognized wheelchair standards and can be safely operated (as determined by a skilled therapist or assistive technology professional). Seat belts, wheel locks, and a properly adjusted wheelchair can prevent serious wheelchair-related injuries. Pressure ulcers are also a significant risk for those who use wheelchairs. Advanced cushion designs and seat functions can provide adequate pressure relief for persons who cannot independently off-load the buttocks. Shoulder pathology and nerve compression injuries at the wrist are common among wheelchair users.41 Using proper wheelchair propulsion biomechanics and an optimal wheelchair setup can help delay the onset of overuse injuries.
Ensure Comfort
Along with mobility, comfort has been reported as the most important attribute or function of a wheelchair.16 Research has shown that most wheelchair users experience regular discomfort. Many either ignore it or seek relief by getting out of the wheelchair, using pain medications, or doing weight shifting (either manually or with tilt and recline).16 A wheelchair that allows for “fine-tuning” of the adjustments provides greater options for achieving comfort, as well as meeting the individual’s postural and pressure needs.
Manual Wheelchairs
Persons with good upper body function and stamina might well be able to use a manual wheelchair for mobility. Manual wheelchairs for daily use are often categorized by their design features and costs. Table 17-1 provides an overview of each adult wheelchair category as defined by the Centers for Medicare & Medicaid Services (CMS), which is the leading third-party payer for wheelchairs. The categories are outdated and are being revised to reflect the actual composition of manual wheelchairs on the market.
The standard wheelchair (Figure 17-1) is designed for short-term, hospital or institutional use and should not be recommended for the patient to use as a personal wheelchair. As noted in Table 17-1, these can be rather heavy with limited sizes available. Figure 17-1 also illustrates the basic components of a wheelchair. The standard wheelchair folds for easy storage and transportability. A “hemi” wheelchair is essentially a standard wheelchair with a lower seat-to-floor height for persons of shorter stature or who use one or both feet for propulsion. A lightweight wheelchair is slightly lighter in weight but with limited sizes. The first three models have few adjustable parts (some models have no adjustable parts) and generally have sling-type upholstery. Sling upholstery has no capacity to provide pressure relief, and the hammock effect that occurs from wear causes uncomfortable and unstable inward rotation of the hips. However, many users have been sitting in a sling seating system for years and have become accustomed to the hammock effect for comfort. Making the switch to a seating system that supports their posture better can be both frustrating and uncomfortable for these users.
The high-strength lightweight and ultralight wheelchairs are designed for long-term use by individuals who spend more than a couple of hours each day in a wheelchair. They have adjustable features, especially the ultralights. There are many advantages to using ultralight wheelchairs over the other wheelchair types. These are highlighted in the following sections that discuss selecting the appropriate seat dimensions, setting up the wheelchair, propulsion mechanics, and transportability. An ultralight wheelchair is depicted in Figure 17-2.
The last two classes of manual wheelchairs listed in Table 17-1 pertain to persons who weigh more than 250 lb. These wheelchairs are heavier than the wheelchairs in the other classes, to support more body weight. These categories are also outdated because of the increasing number of persons with disabilities who are overweight or obese and need wheelchairs. This trend has resulted in an expanded class of “extra–heavy-duty” wheelchairs, referred to as bariatric wheelchairs, which are built to support individuals who weigh between 300 and 1000 lb.
Pediatric manual wheelchairs are similar to the adult wheelchairs but are smaller (seat width or depth <14 inches). Many of these wheelchairs have adjustable frames or kits for accommodating the growth of the child (Figure 17-3). If the child is unable to self-propel the chair, a powered mobility device might provide independent mobility.37 Strollers equipped with a wide range of seating options (Figure 17-4) can also be used to transport children with orthopedic deformities.
Sports wheelchairs are designed specifically for participating in such athletic endeavors as racing, rugby, tennis, and basketball. These wheelchairs are made of lightweight materials, and usually have very aggressive axle positions and camber. Some of the sport wheelchairs have only one wheel in the front, which allows quick turns and enhanced maneuverability (Figure 17-5). Wheelchairs equipped with arm crank mechanisms (called hand cycles) for exercise are available from many manufacturers. Arm crank exercise can help improve cardiovascular fitness, with research showing that arm cranking is more efficient and less of a physical strain than conventional wheelchair propulsion.33
Basic Wheelchair Dimensions
Figure 17-6 shows the measurements that should be taken of the patient’s body for determining wheelchair dimensions. These dimensions are required not only for determining the correct manual (or power) wheelchair size, but also for determining seating system sizes (e.g., cushion, back supports, leg rest lengths).
Seat Height
The seat should be just high enough to accommodate leg length while leaving enough space under the foot rests (about 2 inches or so) to clear obstacles.3 Persons with longer legs often need angled or elevating leg rests that extend the legs slightly outward instead of straight down (knee angle of 90 degrees). This is needed to allow them to get their knees underneath tables. It is more difficult to do if the patient has tight hamstrings. The height of the seat should be adjusted so that the person has enough knee clearance to fit under tables, counters, and sinks at home, at work, at school, and in the community (the Americans with Disabilities Act mandates at least 27-inch-high knee clearance under tables and surfaces). Seat height is also an important consideration for persons who drive while seated in the wheelchair and need to be able to access the steering wheel or hand controls.
Seat Depth
The depth of the seat provides support for the thighs. A seat that is too shallow causes higher sitting pressures because less of the seat is in contact with the thighs. A seat that is too deep can cause excess pressure behind the knees and calves. There can also be a tendency for the pelvis to slide into a posterior tilt so that the back can be adequately supported by the backrest. A 1- to 2-inch gap between the popliteal area and front edge of the cushion is recommended, but might need to be more if the person propels with the feet.3
Back Height
The height of the back is determined by the amount of postural support the person needs. The backrest should be low enough to provide adequate support, but still allow the upper limbs access to as much of the pushrims as possible. Many practitioners use the inferior angle of the scapula as a basis for determining backrest height. The backrest height should be below the inferior angle so that it does not impede arm movements. There are various kinds of back supports (Table 17-2), and some have a tapered area that allows for greater freedom of scapular movement. Only the high-strength lightweight and ultralight wheelchairs permit the attachment of different kinds of back supports.
Manual Wheelchair Setup
Ultralight wheelchairs provide the highest degree of adjustability. This makes it possible to optimize the fit of the wheelchair to the user, which is likely to have a positive impact on propulsion mechanics. In addition to the basic adjustments that can be made on most other wheelchairs (e.g., footrests, armrests), ultralight wheelchair adjustments also allow for adjusting the seat and back angle, rear wheel camber, and rear axle position.
Rear Wheel Camber
Camber is the angle of rear wheel tilt. Zero degrees of camber implies that the rear wheels line up vertically and with the side of the wheelchair. Angling the rear wheels so the top is tilted inward and the bottom outward (see Figure 17-5) results in increased camber and distance between the rear wheels. Most wheelchairs generally have up to 8 degrees of camber. Although more camber is usually possible, it can impede the ability to enter and exit doors and openings. Box 17-2 lists the advantages and disadvantages of camber.
Horizontal Axle Position
Moving the axle forward moves the seat back relative to the rear wheels. This results in a shift of the user’s weight to over or slightly behind the rear axles.9 A more forward axle position requires less muscle effort because rolling resistance is lowered when more weight is distributed over the larger rear wheels than the smaller front casters.31 This position also facilitates “popping a wheelie,” negotiating obstacles, and ascending or descending curbs. In contrast, moving the axle forward can make the wheelchair more “tippy” and difficult to push up a ramp because of the tendency to tip backward. For this reason, wheelchairs are usually delivered with the axle in the most rearward position possible. This position usually needs to be changed, based on input from the patient and the practitioner. An antitipper (Figure 17-7) can help prevent rearward falls; but might also make it more difficult to negotiate a curb and pop a wheelie. Because of the effects on stability, the axle should be moved forward incrementally, provided the wheelchair user feels stable. Adding weight to the chair can also affect stability.27 This is why packages or backpacks ideally should be located underneath the seat of the chair.
Vertical Axle Position
Raising the axle has the effect of lowering the seat, while lowering the axle raises the seat. A lower seat position can improve propulsion biomechanics by increasing hand contact with the pushrim,5,44 lowering stroke frequency,5 and increasing mechanical efficiency.44 Lowering the seat height also increases the stability of the wheelchair. If the seat height is too low, however, the patient has to push with the arm abducted. This can increase the risk of shoulder impingement, another upper limb injury common among manual wheelchair users. The ideal seat height is the point at which the angle between the upper arm and forearm is between 100 and 120 degrees when the hand is resting on the top and center of the pushrim (Figure 17-8, A).5,44 An alternative method that can be used to approximate the same position and angle is to have the individual rest with their arms hanging at the side. The fingertips should be at the same level as the axle of the wheel. If the seat height is too high, less of the pushrim can be accessed and more strokes are needed to go the desired speed (Figure 17-8, B).
Wheelchair Propulsion
Wheelchair Weight
The weight of the wheelchair is an important consideration, especially when prescribing manual wheelchairs. Less propulsive force is needed to push a lighter wheelchair. Ultralight wheelchairs have frames and components made with materials having high strength-to-weight ratios, so less material is needed. One study directly compared ultralight and standard wheelchairs, and found that ultralight wheelchair users pushed at faster speeds, traveled further distances, and used less energy.4 The reduction of force is even more important on inclines where gravitational forces add to the rolling resistance. A light wheelchair is also easier to load into and out of a vehicle.
Quality of the Wheelchair and Setup
Ultralight wheelchairs have better components and are less likely to become misaligned with use, which helps minimize rolling resistance. Keeping the chair in good alignment might require other adjustments, such as to the brakes or caster alignment or height. Axle tubes on rigid ultralight frames can eliminate many of these problems. As discussed previously, a wheelchair that fits the user and is optimized for propulsion by adjusting the axle position makes it easier to push the wheelchair. Lowering stroke frequency and forces through a combination of propulsion training, wheelchair setup, and proper choice of wheelchair can protect the median nerve from injury.7 Instrumented wheels used in prior research15,36 are now available commercially for clinicians to use to objectively evaluate the quality of wheelchair setup and propulsion techniques.
Propulsion Technique
The propulsion techniques of manual wheelchair users have been examined in detail.6,38,40,46 Propulsive strokes are generally described in two phases: when the hand is in contact with the pushrim applying forces (push phase), and when the hand is off the rim and preparing for the next stroke (recovery phase). Four distinct propulsion patterns have been identified, which are defined by the path the hand takes during the recovery phase: arc, semicircular, single-looping over, and double-looping over (Figure 17-9). The single-looping over form of propulsion, which consists of having the hand above the pushrim during recovery, is the most prevalent pattern in individuals with paraplegia.6 However, the semicircular pattern, in which the user’s hand drops below the pushrim during recovery, has better biomechanics (see Figure 17-9, A). The semicircular pattern has been associated with lower stroke frequency and greater time spent in the push phase relative to the recovery phase.6 The semicircular pattern is preferred because the hand follows an elliptical pattern, with no abrupt changes in direction and no extra hand movements. By applying forces to the pushrim in smooth, long strokes, the same amount of energy is imparted to the rim without high peak forces or a high rate of force loading. For example, a long stroke (see Figure 17-9, A), as opposed to a short stroke (see Figure 17-9, B), is likely to minimize the number of strokes needed to push at a desired speed.
Manual Wheelchair Transportability
There are basically two types of manual wheelchair frames: folding and rigid. Folding frames allow the wheelchair to collapse for storage (see Figure 17-1). Rigid frames are mainly available for ultralight wheelchairs (see Figure 17-2) and for wheelchairs with special positioning aids (e.g., tilt or custom seating systems). Rigid frames tend to be more durable than folding because there are fewer moving parts. Fewer moving parts also mean that rigid frame wheelchairs tend to be lighter. The backrests on rigid frames are designed to fold down for improved compactness. A “quick-release” axle allows for easy removal of the wheels on rigid frames and certain folding frames. This option is not available on standard and some lightweight wheelchair models.
Manual Wheelchair Components and Accessories
Refer also to the discussion on seating and positioning.
Wheels and Tires
There are several factors to consider when choosing the most suitable wheel and tire configuration for a wheelchair including type of indoor or outdoor terrain, activity level, maintenance, weight, and cost. Many standard and lightweight wheelchairs come equipped with either mag-style or spoked wheels (Figure 17-10). Mag wheels are made from composite plastics or metal (initially they were made from magnesium, hence the term mag). They are usually heavier than spoked wheels but are more durable and require less maintenance. Newer types of mag wheels are composed of high-strength lightweight materials and can even be lighter than spoked wheels, but are more costly. Spoked wheels have a tendency to get out of alignment (wheel wobbles when spun), requiring a trip to a bicycle shop or a wheelchair dealer for the wheels to be trued.
Grade Aids
Grade aids are devices that attach to the frame and are used for persons who have difficulty with slopes and have a tendency to roll backward down hills. These devices only prevent the wheelchair from rolling backward, and forward motion is unimpeded.
Pushrims
Pushrims are available in different sizes, shapes, and surface finishes. The pushrim most commonly found on wheelchairs is about ½ inch in diameter with a smooth surface finish and round cross-sectional area (see Figure 17-1). Persons who have limited gripping ability (e.g., low-level cervical injuries) might need a larger diameter pushrim or a high-friction surface finish (e.g., vinyl or foam), or both. Sometimes these individuals need a pushrim with vertical, horizontal, or angled projections (Figure 17-11, A) to be able to effectively propel their wheelchairs. New designs provide for greater surface area (Figure 17-11, B) and are also contoured for a more natural hand grip.
Lever Drives
Propelling the wheelchair using levers versus pushrims has proven to be more mechanically efficient. Dual-lever drive wheelchairs are more common in Europe, China, and other countries of the Far East. They are well suited for persons who frequently propel long distances and over outdoor terrain (e.g., dirt roadways). The drawbacks to using a lever drive system include difficulties with maneuvering in tight places, transfers, and transportability. Single-lever drive systems are quite popular in the United States and allow for the wheelchair to be propelled using one arm (Figure 17-12).
Antitippers
Antitippers are devices that attach to the rear of the wheelchair frame and usually have adjustable length tubes with small wheels at the end (see Figure 17-7). These devices protect the user from tipping the wheelchair backward, but can make it difficult for the user to ascend a curb or pop a wheelie. The tube length can be adjusted to allow the user to traverse over small obstacles while still providing some stability. All new manual wheelchairs generally come equipped with antitippers; however, high-end users often remove them after receiving the wheelchair.
Geared and Power-Assisted Wheelchairs
Geared and power-assist devices are appropriate for individuals who use or prefer their manual wheelchairs for mobility, but who need some assistance to reduce the physical effort required to self-propel. These devices are particularly likely to help those with muscle paralysis or weakness, overuse, and fatigue. They are also ideal for individuals who are apprehensive about transitioning to a fully powered wheelchair. This can be due to not wanting to be viewed by peers as being “more disabled,” having homes that do not accommodate the increased size, lacking the financial resources, or having difficulties with transportation. A geared wheelchair does not require batteries and works similar to a bicycle, allowing the user to shift into a lower gear when climbing hills or rolling over uneven or rough terrain. Power-assist devices include stand-alone powered units that are external to the wheelchair and that the wheelchair user holds on to. Another is a power add-on device that attaches to the wheelchair and has a steering mechanism or input device for controlling the wheelchair. Figure 17-13 shows a pushrim-activated system with motors in the wheelchair hubs. Geared and power-assist devices cost less than a fully powered wheelchair system, but require that the individual has a manual wheelchair that is compatible with the power-assist device.
Research has shown that using a geared or pushrim-activated wheelchair results in significant reductions in the physical and physiologic demands of propulsion compared with using a manual wheelchair.11,22 Power-assist devices can increase the width or length of the manual wheelchair base a few inches. Both geared and power-assist devices are more difficult to transport than manual wheelchairs, mainly because the equipment adds between 10 and 50 lb to the wheelchair. This is still considerably lighter, however, than a fully powered wheelchair.
Power Wheelchairs
People who do not have the strength or stamina to propel manual wheelchairs typically need power wheelchairs for mobility independence. Power wheelchairs can be grouped into four broad categories based on wheelchair features and their intended use: (1) conventional power wheelchairs; (2) folding and transport power wheelchairs; (3) combination indoor-outdoor power wheelchairs; and (4) heavy-duty indoor-outdoor power wheelchairs.19
Conventional Power Wheelchairs
Conventional power wheelchairs are not programmable (e.g., no adjustments in acceleration or deceleration, turning speed, joystick sensitivity) and have very basic seating with limited sizes available (Figure 17-14). They are low cost and low quality (see the duscussion of wheelchair standards). They are appropriate for limited indoor use for individuals with good trunk control who do not need specialized seating.
Folding and Transport Power Wheelchairs
Folding and transport power wheelchairs are designed for easy disassembling to facilitate transport (Figure 17-15). They are usually compact for indoor use and have a small footprint (i.e., area connecting the wheels) for greater maneuverability in confined spaces. They might not, however, have the stability or power to negotiate obstacles outdoors. The batteries are often housed in separate boxes having easy-to-separate electrical connectors. These wheelchairs are typically used by individuals with reasonably good trunk and upper body control.
Combination Indoor-Outdoor Power Wheelchairs
Combination indoor-outdoor power wheelchairs (Figure 17-16) are often purchased by people who wish to have mobility indoors (home, school, work) and in the community, but who stay on finished surfaces (e.g., sidewalks, driveways, flooring). These wheelchairs are equipped with standard proportional joysticks and standard programmable electronics (e.g., speed adjustment, tremor dampening, and acceleration control). They come with either standard seating (such as that shown in Figure 17-17) or rehabilitation seating (see Figure 17-16). Rehabilitation seating allows for the attachment of modular seating hardware (e.g., backrests, cushions, laterals, hip guides, and headrests).
Heavy-Duty Indoor-Outdoor Power Wheelchairs
Heavy-duty indoor-outdoor power wheelchairs (Figure 17-18) are for use by people who live in communities without finished surfaces. These wheelchairs usually have large-diameter drive wheels with heavily treaded tires or four-drive wheels for climbing obstacles and traversing rough terrains. Wheelchairs that can support persons who weigh more than 250 lb also fall under this category. These wheelchairs usually weigh 300 to 500 lb.
[/not-level-membership-for-physical-medicine-and-rehabilitation-category]
