Chapter 23 What Is the Optimal Rehabilitative Approach to Post-Traumatic Elbow Stiffness?
CHALLENGES IN IMPLEMENTING EVIDENCE-BASED PRACTICE IN THIS CASE
Evidence-based practice dictates that we use best available evidence when making clinical decisions. In this regard, the question posed in this chapter presents a number of challenges:
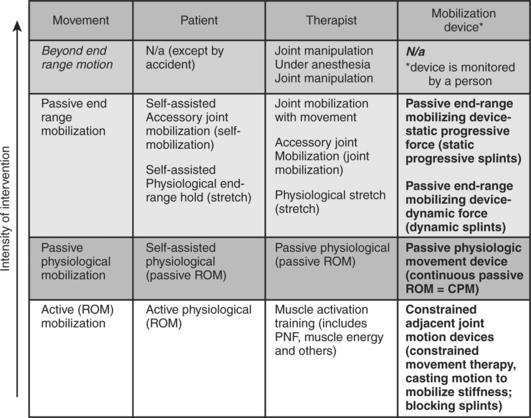
DEFINING THE COMPOSITION AND INTENSITY OF JOINT MOBILITY INTERVENTIONS (FIGURE 1)
Number of repetitions per application or set
Number of sets or applications per day
Figure 1 describes some common mobilization interventions using their common names and categories: active, passive, and manipulation. These fall on a continuum of increasingly intense mobility interventions. The common names are associated with the more specific terminology defined below to define the different delivery/control methods (patient, therapist, mobilization device).
DEFINING AN ANSWERABLE QUESTION
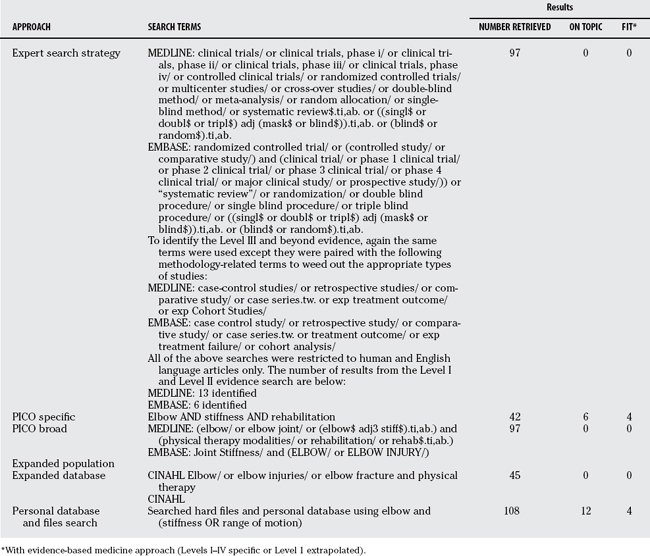
Finding the Evidence
We used several typical database searches (Table 23-1). The classic PICO approach had to be modified due to paucity of evidence.
Appraising and Extracting the Evidence
Systematic Reviews.
Michlovitz and colleagues1 conducted an SR on conservative interventions to improve mobility after upper extremity musculoskeletal trauma. Medline, CINAHL, PEDRO, PubMed, and Cochrane were searched. Two reviewers performed abstract selection and critical appraisal (n = 26 studies; 24-item critical appraisal and level of evidence). The primary outcome considered was ROM measurement. Overall, the quantity and quality of evidence were moderate to low. Level IIb, III, and IV evidence supported the use of joint mobilization, a supervised exercise program, and splinting. No studies found examined techniques of physical agent or electrotherapeutic modalities. The authors conclude that future studies are needed to delineate selection of appropriate candidates for these techniques and effective dosage.
Evidence of Mobilizations
Active Mobilization
Mobilization Splinting
Evidence of Adjunctive Interventions.
Level II evidence exists that cryotherapy is effective in managing muscle stiffness and pain related to a bout of damage-inducing eccentric exercise (8 sets of 5 maximal reciprocal contractions at 0.58 rad × sec−1) of the elbow flexors on an isokinetic dynamometer (n = 15 female subjects). Subjects in the cryotherapy group immersed their exercised arm in cold water (15°C) for 15 minutes immediately after eccentric exercise and then every 12 hours for 15 minutes for a total of seven sessions. Relaxed elbow angle was greater and creatine kinase activity lower for the cryotherapy group than the control group on days 2 and 3 after the eccentric exercise.10
Level V (Expert Recommendations)
A variety of Level V recommendations were extracted from review articles.



 elbow extension and flexion should be performed in pronation (supination increases the radiocapitellar load).
elbow extension and flexion should be performed in pronation (supination increases the radiocapitellar load).













SUMMARY OF RECOMMENDATIONS
Fair evidence exists to suggest the following conclusions:
The preponderance of evidence supports a role for a progressive rehabilitation program, although the specifics of an optimal rehabilitation program cannot be defined on the basis of current exercise. Further research and consensus exercise around condition-specific restrictions and more consistent use of outcome measures would benefit the field. Table 23-2 provides a summary or recommendations for the treatment of post-traumatic elbow stiffness.
| STATEMENT | LEVEL OF EVIDENCE | REFERENCES |
|---|---|---|
ACKNOWLEDGMENT
J.C.M. was funded by a New Investigator Award, Canadian Institutes of Health Research.
1 Michlovitz SL, Harris BA, Watkins MP. Therapy interventions for improving joint range of motion: A systematic review. J Hand Ther. 2004;17:118-131.
2 Ross G, McDevitt ER, Chronister R, Ove PN. Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med. 1999;27:308-311.
3 Seradge H. Cubital tunnel release and medial epicondylectomy: Effect of timing of mobilization. J Hand Surg [Am]. 1997;22:863-866.
4 Schippinger G, Seibert FJ, Steinbock J, Kucharczyk M. Management of simple elbow dislocations. Does the period of immobilization affect the eventual results? Langenbecks Arch Surg. 1999;384:294-297.
5 Bonutti PM, Windau JE, Ables BA, Miller BG. Static progressive stretch to reestablish elbow range of motion. Clin Orthop Relat Res.; 303; 1994; 128-134.
6 Nuismer BA, Ekes AM, Holm MB. The use of low-load prolonged stretch devices in rehabilitation programs in the Pacific northwest. Am J Occup Ther. 1997;51:538-543.
7 Green DP, McCoy H. Turnbuckle orthotic correction of elbow flexion contractures after acute injuires. J Bone Joint Surg Am. 2007;61:1092-1095.
8 Lee MJ, LaStayo PC, von Kersburg AE. A supination splint worn distal to the elbow: A radiographic, electromyographic, and retrospective report. J Hand Ther. 2003;16:190-198.
9 Ippolito E, Formisano R, Caterini R, et al. Resection of elbow ossification and continuous passive motion in postcomatose patients. J Hand Surg [Am]. 1999;24:546-553.
10 Eston R, Peters D. Effects of cold water immersion on the symptoms of exercise-induced muscle damage. J Sports Sci. 1999;17:231-238.
11 Issack PS, Egol KA. Posttraumatic contracture of the elbow: Current management issues. Bull Hosp Jt Dis. 2006;63(3-4):129-136.
12 King GJ, Faber KJ. Posttraumatic elbow stiffness. Orthop Clin North Am. 2000;31:129-143.
13 Morrey BF. The posttraumatic stiff elbow. Clin Orthop Relat Res.; 431; 2005; 26-35.
14 Chinchalkar SJ, Szekeres M. Rehabilitation of elbow trauma. Hand Clin. 2004;20:363-374.






