[level-membership-for-orthopaedics-category]
Chapter 28 What Is the Best Treatment for Femoral Fractures?
Pediatric femoral shaft fractures are among the most common injuries treated by the orthopedic surgeon. These fractures represent 1.6% of all bony injuries in children,1–3 with the majority healing without any long-term sequelae. A review of recent literature illustrates that abuse and falls represent the most common mechanisms of injury for femoral fractures in children 4 years of age and younger. In children older than 11 years, the femoral shaft is much stronger, so fracture is more often caused by high-energy injuries, such as motor vehicle accidents or gunshot wounds.2,4–6
Initial evaluation includes a comprehensive history and physical examination evaluating for the presence of swelling, instability, and/or tenderness. Imaging begins with anteroposterior and lateral radiographs of the entire femur, as well as views of the hip and knee. Rarely, a bone scan or magnetic resonance imaging is valuable, such as in the diagnosis of stress fractures.7
OVERVIEW
Femoral fractures are often separated into three broad categories according to the geographic location of the fracture, which include proximal femur fractures, femoral shaft fractures, and supracondylar femur fractures. The character of the fracture can also be classified based on its appearance: (1) transverse, spiral, or oblique; (2) comminuted or noncomminuted; and (3) open or closed.7 The nature of the injury, the character of the fracture, the child’s age, and the amount of soft-tissue involvement are important factors that ultimately influence treatment options.
Treatment options may be divided into traction/casting versus operative fixation management with the decision ultimately based on the child’s age, weight, and fracture stability. Closed reduction and casting is the treatment of choice in younger children, whereas fixation is used for older patients (Table 28-1).
TABLE 28-1 Treatment Options for Pediatric Femoral Shaft Fractures
| AGE | TREATMENT |
|---|---|
| Younger than 6 months |
In infants (birth to 6 months old), a stable proximal or midshaft femoral fracture can be treated with a simple splint or Pavlik harness. An infant with an unstable femoral fracture may need a Pavlik harness with a splint around the thigh to provide extra support. Immediate spica casting may be required in infants who present with femoral fractures of excessive shortening or angulation.7 A Pavlik harness facilitates skin care but does not offer the pain relief of full immobilization in a spica cast.
For children 6 months to 4 years of age, immediate (or early) spica casting is the method of choice for femoral fractures with less than 2 cm of initial shortening. Children in this age group with greater than 2 cm of initial shortening may require 3 to 10 days of skeletal traction followed by spica casting.7 In rare cases, external fixation and flexible intramedullary nailing (FIN) are used in this age group.
For children 4 to 11 years old, many treatment methods can be used, based on the surgeons’ preference, fracture type, and family’s wishes. Treatment options include early spica casting, skeletal traction followed by spica casting, FIN, plate fixation, solid antegrade nailing, and external fixation.7 The optimal treatment for femur fractures in this 4- to 11-year-old age group is based on the nature of the injury, the character of the fracture, the skeletal maturity, the patient’s weight, and the experience and skill of the surgeon with a given treatment method.
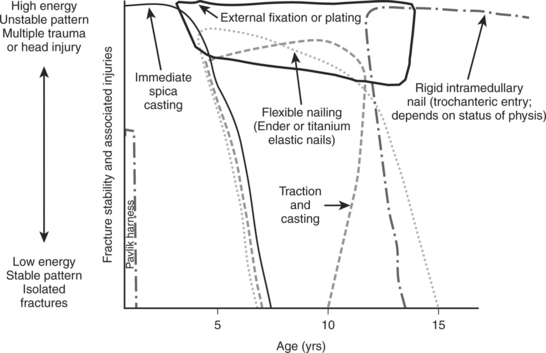
Children 11 years of age to skeletal maturity require maximum fixation strength whereas avoiding avascular necrosis or growth arrest. Treatment options include FIN, plating, locked intramedullary nails, and external fixation.7 Rigid, locked intramedullary nailing utilizes a trochanteric starting point and is popular particularly in those children who are closer to skeletal maturity. Submuscular plating is becoming increasingly popular for this age group. Traction followed by spica casting, which was a standard treatment in the 1990s, is rarely used for this age group today (Fig. 28-1).8
EVIDENCE
Six Months to 4 Years
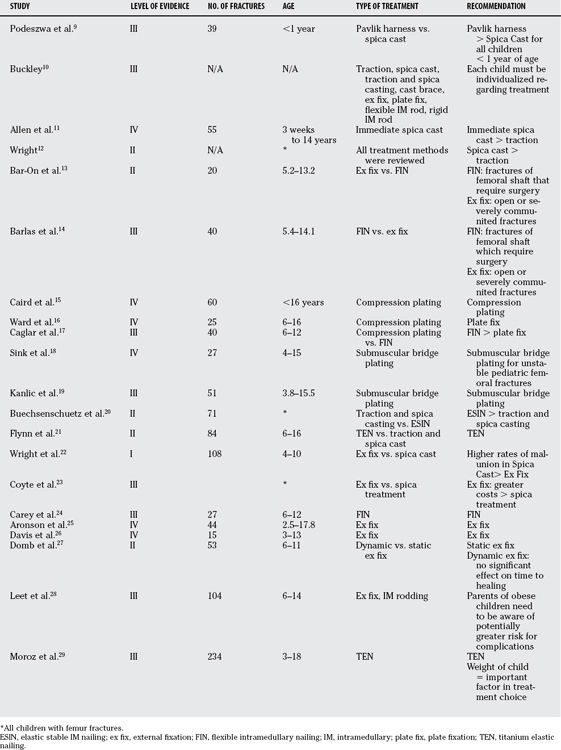
Several studies have shown that both the Pavlik harness (younger than 6 months) and spica casting (6 months to 4 years of age) are acceptable treatment options (Table 28-2). A retrospective study (Level III evidence) of 40 patients by Podeszwa and colleagues9 compared application of the Pavlik harness versus spica casting for the treatment of children younger than 1 year. No difference was found in radiographic outcomes, but approximately one third of all spica patients experienced development of a skin complication. The authors conclude that all children younger than 1 year with a femoral shaft fracture should be considered for treatment with a Pavlik harness.9 Buckley10 reports the current trends in the treatment of femoral shaft fractures in children and adolescents. By analyzing healthcare costs and the desire for early discharge, he concludes that immediate hip spica casting remains the optimum method of treatment for most children 4 years and younger (Level III evidence). Allen and colleagues11 likewise recommend immediate spica casting for femoral shaft fractures in infants and children. They reviewed 55 femoral shaft fractures in children treated by closed reduction and immediate application of a double hip spica cast, and showed satisfactory results in all cases (level IV evidence case series, but with uniform outcome).11 In a study comparing spica casting and skeletal traction, Wright12 shows that early application of a hip spica cast had lower costs and malunion rates than traction (Level II evidence).
| STUDY | LEVEL OF EVIDENCE | GRADE OF RECOMMENDATION |
|---|---|---|
| Podeszwa et al.9 | III | B |
| Buckley10 | III | B |
| Allen et al.11 | IV | c |
| Wright12 | II | B |
| Bar-On et al.13 | II | B |
| Barlas et al.14 | III | B |
| Caird et al.15 | IV | C |
| Ward et al.16 | IV | C |
| Caglar et al.17 | III | B |
| Sink et al.18 | IV | B |
| Kanlic et al.19 | III | B |
| Buechsenschuetz et al.20 | II | B |
| Flynn et al.21 | II | B |
| Wright et al.22 | I | A |
| Coyte et al.23 | III | B |
| Carey et al.24 | III | B |
| Aronson et al.25 | IV | C |
| Davis et al.26 | IV | C |
| Domb et al.27 | II | B |
| Leet et al.28 | III | B |
| Moroz et al.29 | III | B |
Four to 11 Years
Femur fracture treatment for the 4- to 11-year-old age group has been the most frequently studied cohort. Bar-On and researchers13 prospectively reviewed external 1fixation versus FIN for the femoral shaft in 19 children aged 5.2 to 13.2 years with 20 fractures of the femoral shaft (Level II evidence). The FIN group showed much more callous formation, and the time to full weight bearing, full range of movement, and return to school were all shorter. Bar-On and researchers13 conclude, “External fixation should be reserved for open or severely comminuted fractures.” Barlas and Beg14 similarly reviewed external fixation and FIN in 40 children between 5.4 and 14.1 years of age. They also found an earlier return to function in the FIN group with minimal complications (Level III evidence). Their recommendations further support the efficacy of FIN over external fixation for patients in this age group.14
Other techniques in the 4- to 11-year-old age group including plating have also been evaluated. Caird and coauthors15 reviewed open compression plating and found 100% union rate in 60 children younger than 16 years with minimal complications (Level IV). Ward and coauthors16 likewise reviewed 25 children 6 to 16 years old treated with plate fixation, and found 23 of 25 fractures to heal in 11 weeks, on average, with leg length discrepancy not being a clinical problem (Level IV). Their indications for using this technique include a severe head injury or associated polytrauma. Caglar and colleagues17 compare compression plating and FIN in pediatric femoral shaft fractures. Their results illustrate that FIN provided a high union rate with a shorter operation time when compared with the patients treated with compression plating (Level III).
Sink and coworkers18 report the results of 27 patients treated with submuscular bridge plating for unstable femoral fractures (Level IV). No intraoperative or postoperative complications resulted. No instrumentation failure or loss of reduction was seen, whereas early callus was seen by 6 to 8 weeks and stable bony union by 12 weeks in all patients. Sink and coworkers18 conclude, “Submuscular plating is a reasonable option for operative stabilization of communited and unstable pediatric femoral fractures.” Kanlic and researchers19 similarly repor-ted the advantages of submuscular bridge plating. All 51 patients with an average age of 10 years had fractures united with excellent clinical results (Level IV). Kanlic and researchers19 conclude, “This technique offers the advantage of adequate stability for early functional treatment and predictable healing with maintenance of length and alignment for all pediatric femoral shaft fractures.”
Other groups have compared nonoperative versus operative management techniques. Buechsenschuetz and coworkers20 have examined traction and casting versus elastic stable intramedullary nailing. Cost analyses and a comparison of clinical/functional parameters were done. No difference existed between the two groups for standard clinical/functional criteria. Elastic stable intramedullary nailing was associated with a lower overall cost than traction and casting. The authors found that a lower cost and comparable clinical outcome make elastic stable intramedullary nailing a better option than the traditional traction and casting for patients with femoral fractures (Level II).20 Flynn and investigators21 have compared titanium elastic nailing with traction and a spica cast. By prospectively following 83 patients, the results illustrate that children treated with titanium elastic nailing had shorter hospitalization, walked with support sooner, walked independently sooner, and returned to school earlier. These differences were significant (P <0.0001) (Level II).
External fixation has also been compared with casting. Wright and coauthors22 performed a multicenter prospective study comparing malunion rates after external fixation and after early hip spica cast application. Their results illustrated that the rate of malunion was significantly greater in the spica group than in the external fixator group 2 years after fracture (Level I). Coyte and investigators,23 however, saw a greater expected total cost for patients and their families treated with external fixation as compared with those who were treated with an early hip spica cast (Level III). Fifty percent of this difference was attributable to the longer inpatient stays for patients treated with an external fixation device.
Other studies have focused on a single technique separately. Carey and Galpin24 conclude that FIN seems to be a safe and effective method of treatment of femoral fractures for patients between 6 and 12 years of age (Level IV). Aronson and Tursky,25 however, examined external fixation and found promising results with this technique. Most patients returned to school by 4 weeks, and all had full knee motion 6 weeks after fixator removal (Level IV). Davis and colleagues26 also conclude in their small cohort (n 5 14) that external fixation is an effective means of treating isolated femoral fractures in the pediatric population (Level IV). A major disadvantage of external fixation is stress-shielding and re-fracture. Domb and researchers27 hypothesize that the use of axial dynamization may improve the speed and strength of callus formation. Looking at dynamization versus static external fixation in 52 patients, the author provide results that there was no difference in healing or frequency of complications for dynamic versus static external fixation techniques (Level II) (Tables 28-3 and 28-4).
| STATEMENT | LEVEL OF EVIDENCE/GRADE OF RECOMMENDATION | REFERENCES |
|---|---|---|
Areas of Uncertainty
Larger and Older Children.
Leet and coauthors28 illustrate that obese children have an increased rate of complications after surgical treatment of femoral shaft fractures as compared with children of normal body weight. Moroz and colleagues29 have conducted a multicenter study between 1996 and 2003 of 234 femur fractures treated by titanium elastic nailing. Although the outcome was excellent in the majority of the patients, 150 of 234 (65%) heavier children were more likely to have a poor outcome. In fact, a poor outcome was five times more likely in children who weighed more than 49 kg (Level II). Both studies illustrate that the child’s weight is an important criteria in choosing an appropriate treatment option.
Guidelines
For children 4 to 11 years old, length-stable fractures are best managed with elastic nailing in most cases. Some surgeons prefer submuscular plating for this group. Submuscular plates offer more stability, but the implants are harder to remove. For length-unstable fractures, submuscular plating and external fixation (depending on the surgeon’s preference and experience) are probably the best options in most cases. Elastic nailing can be used for length unstable fractures, especially in smaller, younger patients, but supplementary cast immobilization may be necessary for a short period, and the risk for malunion is somewhat greater. Solid antegrade nailing can also be used in this group and is usually reserved for the older, heavier children.
Skeletally mature adolescents are treated with solid antegrade or retrograde interlocking nails.
1 Fry K, Hoffer MM, Brink J. Femoral shaft fractures in brain-injured children. J Trauma. 1976;16:371-373.
2 Hedlund R, Lindgren U. The incidence of femoral shaft fractures in children and adolescents. J Pediatr Orthop. 1986;6:47-50.
3 Landin LA. Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950–1979. Acta Orthop Scand Suppl. 1983;202:1-109.
4 Blakemore LC, Loder RT, Hensinger RN. Role of intentional abuse in children 1 to 5 years old with isolated femoral shaft fractures. J Pediatr Orthop. 1996;16:585-588.
5 Daly KE, Calvert PT. Accidental femoral fracture in infants. Injury. 1991;22:337-338.
6 Loder RT. Pediatric polytrauma: Orthopaedic care and hospital course. J Orthop Trauma. 1987;1:48-54.
7 Beaty J, Kasser J. Rockwood and WIlkins’ Fractures in Children, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 2006.
8 Flynn JM, Schwend RM. Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg. 2004;12:347-359.
9 Podeszwa DA, Mooney JF3rd, Cramer KE, Mendelow MJ. Comparison of Pavlik harness application and immediate spica casting for femur fractures in infants. J Pediatr Orthop. 2004;24:460-462.
10 Buckley SL. Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop Relat Res.; 338; 1997; 60-73.
11 Allen BLJr, Schoch EP3rd, Emery FE. Immediate spica cast system for femoral shaft fractures in infants and children. South Med J. 1978;71:18-22.
12 Wright JG. The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg. 2000;43:180-189.
13 Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailing for femoral shaft fractures in children. A prospective, randomised study. J Bone Joint Surg Br. 1997;79:975-978.
14 Barlas K, Beg H. Flexible intramedullary nailing versus external fixation of paediatric femoral fractures. Acta Orthop Belg. 2006;72:159-163.
15 Caird MS, Mueller KA, Puryear A, Farley FA. Compression plating of pediatric femoral shaft fractures. J Pediatr Orthop. 2003;23:448-452.
16 Ward WT, Levy J, Kaye A. Compression plating for child and adolescent femur fractures. J Pediatr Orthop. 1992;12:626-632.
17 Caglar O, Aksoy MC, Yazici M, Surat A. Comparison of compression plate and flexible intramedullary nail fixation in pediatric femoral shaft fractures. J Pediatr Orthop B. 2006;15:210-214.
18 Sink EL, Hedequist D, Morgan SJ, Hresko T. Results and technique of unstable pediatric femoral fractures treated with submuscular bridge plating. J Pediatr Orthop. 2006;26:177-181.
19 Kanlic EM, Anglen JO, Smith DG, et al. Advantages of submuscular bridge plating for complex pediatric femur fractures. Clin Orthop Relat Res. 2004;426:244-251.
20 Buechsenschuetz KE, Mehlman CT, Shaw KJ, et al. Femoral shaft fractures in children: Traction and casting versus elastic stable intramedullary nailing. J Trauma. 2002;53:914-921.
21 Flynn JM, Luedtke LM, Ganley TJ, et al. Comparison of titanium elastic nails with traction and a spica cast to treat femoral fractures in children. J Bone Joint Surg Am. 2004;86-A:770-777.
22 Wright JG, Wang EE, Owen JL, et al. Treatments for paediatric femoral fractures: A randomised trial. Lancet. 2005;365:1153-1158.
23 Coyte PC, Bronskill SE, Hirji ZZ, et al. Economic evaluation of 2 treatments for pediatric femoral shaft fractures. Clin Orthop Relat Res.; 336; 1997; 205-215.
24 Carey TP, Galpin RD. Flexible intramedullary nail fixation of pediatric femoral fractures. Clin Orthop Relat Res. 1996;332:110-118.
25 Aronson J, Tursky EA. External fixation of femur fractures in children. J Pediatr Orthop. 1992;12:157-163.
26 Davis TJ, Topping RE, Blanco JS. External fixation of pediatric femoral fractures. Clin Orthop Relat Res.; 318; 1995; 191-198.
27 Domb BG, Sponseller PD, Ain M, Miller NH. Comparison of dynamic versus static external fixation for pediatric femur fractures. J Pediatr Orthop. 2002;22:428-430.
28 Leet AI, Pichard CP, Ain MC. Surgical treatment of femoral fractures in obese children: Does excessive body weight increase the rate of complications? J Bone Joint Surg Am. 2005;87:2609-2613.
29 Moroz LA, Launay F, Kocher MS, et al. Titanium elastic nailing of fractures of the femur in children. Predictors of complications and poor outcome. J Bone Joint Surg Br. 2006;88:1361-1366.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
Chapter 28 What Is the Best Treatment for Femoral Fractures?
Pediatric femoral shaft fractures are among the most common injuries treated by the orthopedic surgeon. These fractures represent 1.6% of all bony injuries in children,1–3 with the majority healing without any long-term sequelae. A review of recent literature illustrates that abuse and falls represent the most common mechanisms of injury for femoral fractures in children 4 years of age and younger. In children older than 11 years, the femoral shaft is much stronger, so fracture is more often caused by high-energy injuries, such as motor vehicle accidents or gunshot wounds.2,4–6
Initial evaluation includes a comprehensive history and physical examination evaluating for the presence of swelling, instability, and/or tenderness. Imaging begins with anteroposterior and lateral radiographs of the entire femur, as well as views of the hip and knee. Rarely, a bone scan or magnetic resonance imaging is valuable, such as in the diagnosis of stress fractures.7
OVERVIEW
Femoral fractures are often separated into three broad categories according to the geographic location of the fracture, which include proximal femur fractures, femoral shaft fractures, and supracondylar femur fractures. The character of the fracture can also be classified based on its appearance: (1) transverse, spiral, or oblique; (2) comminuted or noncomminuted; and (3) open or closed.7 The nature of the injury, the character of the fracture, the child’s age, and the amount of soft-tissue involvement are important factors that ultimately influence treatment options.
Treatment options may be divided into traction/casting versus operative fixation management with the decision ultimately based on the child’s age, weight, and fracture stability. Closed reduction and casting is the treatment of choice in younger children, whereas fixation is used for older patients (Table 28-1).
TABLE 28-1 Treatment Options for Pediatric Femoral Shaft Fractures
| AGE | TREATMENT |
|---|---|
| Younger than 6 months |
In infants (birth to 6 months old), a stable proximal or midshaft femoral fracture can be treated with a simple splint or Pavlik harness. An infant with an unstable femoral fracture may need a Pavlik harness with a splint around the thigh to provide extra support. Immediate spica casting may be required in infants who present with femoral fractures of excessive shortening or angulation.7 A Pavlik harness facilitates skin care but does not offer the pain relief of full immobilization in a spica cast.
For children 6 months to 4 years of age, immediate (or early) spica casting is the method of choice for femoral fractures with less than 2 cm of initial shortening. Children in this age group with greater than 2 cm of initial shortening may require 3 to 10 days of skeletal traction followed by spica casting.7 In rare cases, external fixation and flexible intramedullary nailing (FIN) are used in this age group.
For children 4 to 11 years old, many treatment methods can be used, based on the surgeons’ preference, fracture type, and family’s wishes. Treatment options include early spica casting, skeletal traction followed by spica casting, FIN, plate fixation, solid antegrade nailing, and external fixation.7 The optimal treatment for femur fractures in this 4- to 11-year-old age group is based on the nature of the injury, the character of the fracture, the skeletal maturity, the patient’s weight, and the experience and skill of the surgeon with a given treatment method.
Children 11 years of age to skeletal maturity require maximum fixation strength whereas avoiding avascular necrosis or growth arrest. Treatment options include FIN, plating, locked intramedullary nails, and external fixation.7 Rigid, locked intramedullary nailing utilizes a trochanteric starting point and is popular particularly in those children who are closer to skeletal maturity. Submuscular plating is becoming increasingly popular for this age group. Traction followed by spica casting, which was a standard treatment in the 1990s, is rarely used for this age group today (Fig. 28-1).8
EVIDENCE
Six Months to 4 Years
Several studies have shown that both the Pavlik harness (younger than 6 months) and spica casting (6 months to 4 years of age) are acceptable treatment options (Table 28-2). A retrospective study (Level III evidence) of 40 patients by Podeszwa and colleagues9 compared application of the Pavlik harness versus spica casting for the treatment of children younger than 1 year. No difference was found in radiographic outcomes, but approximately one third of all spica patients experienced development of a skin complication. The authors conclude that all children younger than 1 year with a femoral shaft fracture should be considered for treatment with a Pavlik harness.9 Buckley10 reports the current trends in the treatment of femoral shaft fractures in children and adolescents. By analyzing healthcare costs and the desire for early discharge, he concludes that immediate hip spica casting remains the optimum method of treatment for most children 4 years and younger (Level III evidence). Allen and colleagues11 likewise recommend immediate spica casting for femoral shaft fractures in infants and children. They reviewed 55 femoral shaft fractures in children treated by closed reduction and immediate application of a double hip spica cast, and showed satisfactory results in all cases (level IV evidence case series, but with uniform outcome).11 In a study comparing spica casting and skeletal traction, Wright12 shows that early application of a hip spica cast had lower costs and malunion rates than traction (Level II evidence).
| STUDY | LEVEL OF EVIDENCE | GRADE OF RECOMMENDATION |
|---|---|---|
| Podeszwa et al.9 | III | B |
| Buckley10 | III | B |
| Allen et al.11 | IV | c |
| Wright12 | II | B |
| Bar-On et al.13 | II | B |
| Barlas et al.14 | III | B |
| Caird et al.15 | IV | C |
| Ward et al.16 | IV | C |
| Caglar et al.17 | III | B |
| Sink et al.18 | IV | B |
| Kanlic et al.19 | III | B |
| Buechsenschuetz et al.20 | II | B |
| Flynn et al.21 | II | B |
| Wright et al.22 | I | A |
| Coyte et al.23 | III | B |
| Carey et al.24 | III | B |
| Aronson et al.25 | IV | C |
| Davis et al.26 | IV | C |
| Domb et al.27 | II | B |
| Leet et al.28 | III | B |
