CHAPTER 5 Wedge Resection and Brachytherapy for Lung Cancer – video 5
Introduction
Compared with a lobectomy, wedge resection carries a three to five times greater risk of local recurrence and has a lower survival rate.1 The standard of practice for the surgical treatment of lung cancer is a lobectomy, but because some patients cannot physiologically tolerate a lobectomy, an alternative is needed. Traditional external beam radiation can have the same negative impact on pulmonary function as a lobectomy. Wedge resection with localized radiation (i.e., brachytherapy) has been developed as better alternatives. Because preliminary series have shown very good results, an intergroup, randomized trial (ACOSOG Z4032) has been undertaken to evaluate the long-term benefits of brachytherapy for reducing the risk of local recurrence.
Santos and colleagues described one approach to brachytherapy. They embedded iodine 125 sutures in a Vicryl mesh that was subsequently secured to the surface of the lung at the margin of the resection.2 This provided a radiation dose of 100 Gy to a depth of 5 mm. The brachytherapy group had a lower local recurrence rate (19% versus 2%, P = .0001).2 There were no adverse effects related to the placement of the brachytherapy mesh, including no radiation pneumonitis, no implant migration or implant-related morbidity, and no compromise of pulmonary function when comparing preoperative and postoperative values. A concern regarding that approach is the radiation exposure for intraoperative personnel and for the patient’s visitors. An alternative approach with afterload catheters appears to have similar results.3 Both approaches are described in this chapter.
Approach to Wedge Resection and Brachytherapy
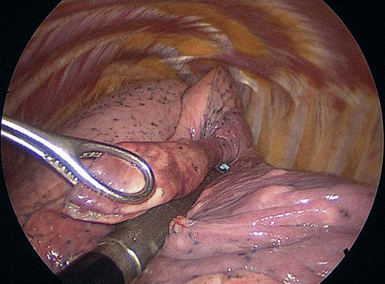
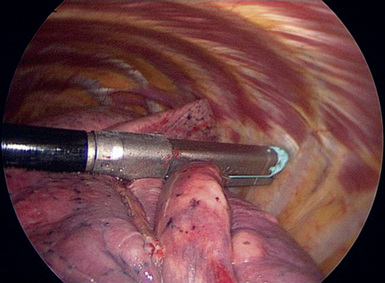
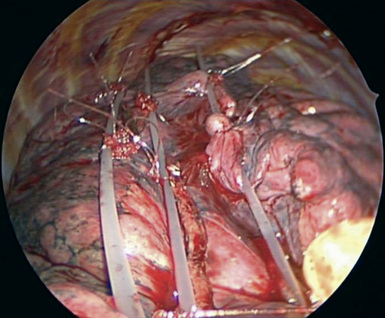
Step 2. Wedge Resection
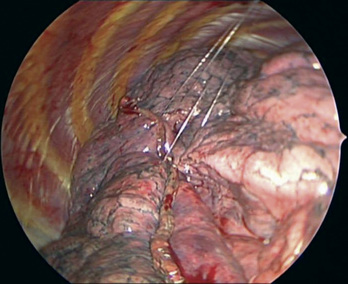
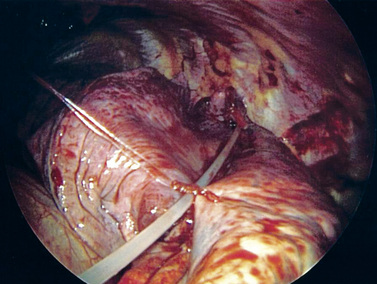
Step 3. Afterload Catheters




Alternative Approach to Wedge Resection and Brachytherapy
Step 2. Mesh with Iodine 125
Radiation Safety After Iodine 125 Seed Implantation
Intraoperative Considerations (Not Afterload Catheter Method)
1 Ginsberg R.J., Rubinstein L.V. Randomized trial of lobectomy versus limited resection for T1N0 lung cancer. Ann Thorac Surg. 1995;60:615-621.
2 Santos R., Colonias A., Parda D., et al. Comparison between sublobar resection and 125 I brachytherapy following sublobar resection in high risk patients with stage 1 non-small cell lung cancer. Surgery. 2003;134:691-697.
3 McKenna R.J.Jr., Mahtabifard A., Yap J., et al. Wedge resection and brachytherapy for lung cancer in patients with poor pulmonary function. Ann Thorac Surg. 2008;85:S733-S736.






