[level-membership-for-internal-medicine-category]
Vomiting
Vomiting is the forceful ejection of gastric contents through the mouth. It occurs when the vomiting centre in the medulla oblongata is stimulated. This may be due to direct stimulation of the centre (central vomiting) or via afferent fibres (reflex vomiting). Haematemesis (vomiting blood) is dealt with in a separate chapter on p. 195.
Causes
Central Vomiting
Reflex Vomiting
Gastrointestinal disease
Inflammation/irritation
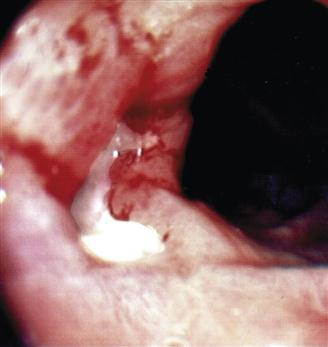
• Peptic ulceration/acute gastritis (Fig. 66)
• Viral
• Bacteria, e.g. Campylobacter, Salmonella spp
• Drugs, e.g. aspirin, NSAIDs, alcohol, iron, antibiotics
CNS causes
Psychogenic
History
General
Nature of the vomiting
Bright-red blood, e.g. bleeding peptic ulcer. Altered blood (coffee grounds). Bile (high small bowel obstruction), faeculent (low small or large bowel obstruction). Recently eaten food. Food several days old (pyloric stenosis), projectile vomiting (infantile pyloric stenosis).
Time of vomit
Soon after meal (gastric ulcer, gastric carcinoma). Early morning (pregnancy). Chronic chest infection (after bout of coughing).
Relief of pain by vomiting
Peptic ulcer disease.
Central vomiting
Take a careful drug history. It will be obvious if the patient is having chemotherapy. Acute infections in children will usually be obvious. Check for pregnancy. Endocrine and metabolic disorders will largely be determined by the result of blood tests.
Reflex vomiting
Gastrointestinal
There will usually be a clear history of a gastrointestinal problem, e.g. localised tenderness of peritonitis or colicky abdominal pain associated with obstruction. Take a careful drug history for irritant drugs, e.g. aspirin. Check for abuse of emetics, e.g. bulimia.
CNS
With raised intracranial pressure, there will usually be headache, drowsiness and fits in addition to vomiting. With labyrinthitis, there will be nausea, vomiting, vertigo and often a hearing defect. Ménière’s disease presents with vertigo, tinnitus and deafness. The tinnitus is usually constant but more severe before an attack. Tinnitus may precede other symptoms by many months. Attacks of Ménière’s disease may last from minutes to hours. Migraine will present with a visual aura with unilateral throbbing headache and sometimes photophobia. With motion sickness, the history is usually obvious.
Psychogenic
Bulimia is eating followed by self-induced vomiting. Vomiting may also occur in anorexia nervosa but failure to eat is usually the prominent feature. Hysteria may be responsible for vomiting. Full psychiatric assessment is recommended.
Others
For other causes, the history will usually be obvious. There will usually be severe chest pain in myocardial infarction, and severe pain associated with testicular torsion or trauma. A history of a fracture will be obvious. There may be a history of severe chest infection, e.g. bronchitis or bronchiectasis, associated with coughing bouts followed by vomiting. There may be a recent history of radiotherapy for malignant disease. Widespread malignant disease may cause vomiting.
Examination
Gastrointestinal
A full gastrointestinal examination should be carried out. Look for signs of localised tenderness or signs of intestinal obstruction.
CNS
With raised intracranial pressure, there will be listlessness, irritability, drowsiness, and the pulse rate will be low with a rising blood pressure. Check for papilloedema. Ultimately, coma and irregular breathing will occur. With acute labyrinthitis, there may be nystagmus to the opposite side from the lesion. The fistula test will be positive (pressure on the tragus causes vertigo or eye deviation by reducing movement of the perilymph). Sensorineural deafness may occur in purulent labyrinthitis. With Ménière’s, there will be rotatory nystagmus and unsteadiness of stance and gait during an attack, together with past-pointing.
Psychogenic
In anorexia nervosa, a wasted hirsute female will present, often with anxious parents.
Others
With myocardial infarction, there may be signs of acute congestive cardiac failure. With causes of severe pain, attention will normally be drawn to the appropriate area, e.g. scrotum with testicular trauma or torsion. With irradiation, there may be skin signs of recent radiotherapy. With widespread malignant disease, the patient is often cachectic. A site of the primary may be obvious. With severe coughing, chest signs may be obvious.
General Investigations
■ FBC, ESR, CRP
Hb ↓ gastrointestinal disease. Malignancy. Anorexia nervosa. WCC ↑ abdominal inflammation. ESR ↑ inflammation. Tumour.
■ U&Es
Dehydration. Uraemia. Hyperkalaemia occurs in Addison’s disease.
■ Urinalysis
Glucose and ketones in diabetes; blood, white cells and protein suggest UTI, blood may indicate kidney stone.
■ CXR
Congestive cardiac failure – pulmonary oedema. Malignancy. Pneumonia. Bronchiectasis.
Specific Investigations
■ Blood glucose
Raised in diabetes. Low in Addison’s disease.
■ Serum calcium
Hyperparathyroidism and other causes of hypercalcaemia.
■ Toxicology screen
Drug causes of vomiting.
■ Barium enema
Malignancy. Diverticular disease.
■ Small bowel enema
Gastrointestinal disease, e.g. Crohn’s disease.
■ OGD
Peptic ulcer disease. Malignancy.
■ US
Gastrointestinal disease, e.g. gallstones.
■ CT
Abdominal malignancy. Cerebral haemorrhage.
■ MRI
Intracranial lesion associated with raised intracranial pressure.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]
Vomiting
Vomiting is the forceful ejection of gastric contents through the mouth. It occurs when the vomiting centre in the medulla oblongata is stimulated. This may be due to direct stimulation of the centre (central vomiting) or via afferent fibres (reflex vomiting). Haematemesis (vomiting blood) is dealt with in a separate chapter on p. 195.
Causes
Central Vomiting
Reflex Vomiting
Gastrointestinal disease
Inflammation/irritation
• Peptic ulceration/acute gastritis (Fig. 66)
• Viral
• Bacteria, e.g. Campylobacter, Salmonella spp
• Drugs, e.g. aspirin, NSAIDs, alcohol, iron, antibiotics
CNS causes
Psychogenic
Others
• Severe pain, e.g. testicular torsion, fractures
[/not-level-membership-for-internal-medicine-category]
