[level-membership-for-dermatology-category]
15 Volumetric treatment of the brows
Summary and Key Features
• Orbits that are large, round, and hollow are associated with age, not youth
• Young orbits are almond shaped, the bone is not visible and there may be considerable fullness of the upper lid
• The same configurations that are seen in younger patients may be perceived as looking old in older ones
• Communication is difficult in the periorbital area. Many patients want the eye ‘lifted’ or skin and fat removed since that is what they have been told is done. Moreover, some patients like the hollow and defined look as it may look more dramatic and makeup can be used more liberally
• The author prefers using a trial of local anesthetic in the upper lid to demonstrate the visual effect of filling in the upper lids and brow. If the patient likes the look, the injection is done immediately; there is no need to wait. Local anesthetic provides a vasoconstricted environment. There is no better way of communicating the visual effect of the brow fill
• Putting in the local anesthetic and avoiding overfills and fluid blobs in the upper lid is difficult to do well and easily; some practice is involved. The area is massaged and a few minutes should elapse to let the local distribute before showing the patient
• Underfill is better than overfill. This is not a method to fill in an abundance of skin, though the fill does inflate some skin. Nor is it a method to lift brows, though the brow can elevate in a few patients. Someone with full heavy lids is not a candidate for this procedure
• The author favors non-cross-linked hyaluronic acid (HA) products in the brow as they have more projection
• One should expect at least 2 years’ duration in this location with HA products
• The injector should always be aware of the presence of the globe. Some upper orbits are very shallow and the globe is immediately adjacent to the bone
The ‘local preview’
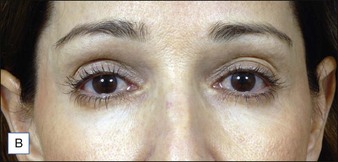
What has proved extremely useful is the ‘local preview’, as I have previously described (2009); a milliliter or two of  % epinephrine is injected into the brow with the intention of visualizing the effect of filling the area and also to make it numb and vasoconstricted (Fig. 15.1). With the use of an ice cube for the initial injections, this is almost painless.
% epinephrine is injected into the brow with the intention of visualizing the effect of filling the area and also to make it numb and vasoconstricted (Fig. 15.1). With the use of an ice cube for the initial injections, this is almost painless.


 –1 mL per side – than the actual product injection. The long-term result looks like the result at the end of the procedure and typically lasts 2–3 years. (A) Before and (B) after injection.
–1 mL per side – than the actual product injection. The long-term result looks like the result at the end of the procedure and typically lasts 2–3 years. (A) Before and (B) after injection.The injection
As illustrated in Figure 15.2, my preferred technique is to begin laterally and place three fanning longitudinal fills with a 30 g  -inch (6 mm) needle: high, middle, and low. The process is repeated across the brow. Tiny amounts are placed with each pass. If the thumb moves perceptibly then the volume is excessive. A small needle like the 30 g
-inch (6 mm) needle: high, middle, and low. The process is repeated across the brow. Tiny amounts are placed with each pass. If the thumb moves perceptibly then the volume is excessive. A small needle like the 30 g  inch is protective in avoiding overfills. Palpation is an excellent way to determine the evenness of the injection. Typically the injection should not go inferior to the border of the orbital bone laterally and centrally. Unless one is confident of the intention and results it is very easy to create irregularities or worse here. The expansion of the curve of the orbital bone suffices to improve the hollow of all but the most deep-set and hollow orbits. As one proceeds medially the injection might need to drop inferior to the level of the bone somewhat. Usually
inch is protective in avoiding overfills. Palpation is an excellent way to determine the evenness of the injection. Typically the injection should not go inferior to the border of the orbital bone laterally and centrally. Unless one is confident of the intention and results it is very easy to create irregularities or worse here. The expansion of the curve of the orbital bone suffices to improve the hollow of all but the most deep-set and hollow orbits. As one proceeds medially the injection might need to drop inferior to the level of the bone somewhat. Usually  mL per side is injected. For economic reasons, this seems a good place to start and in fact most brows and the expressive qualities of the face are improvable by even this small amount, even if undercorrected. I am always amazed by the ability of such a small amount of filler to create as much difference as it does. With experience, it is obvious where the product needs to be placed.
mL per side is injected. For economic reasons, this seems a good place to start and in fact most brows and the expressive qualities of the face are improvable by even this small amount, even if undercorrected. I am always amazed by the ability of such a small amount of filler to create as much difference as it does. With experience, it is obvious where the product needs to be placed.

Who is a candidate for brow volume treatments?
Brows that have deflated evenly (Figs 15.3–15.5) and brows where the medial supraorbital crease peaks medially are excellent candidates. This latter group is interesting in that a medial peak of the supraorbital crease gives people a look of anxiety or worry. A very small amount of filler in this location alters the emotional projection of the face (Fig. 15.6). Though actual elevation of the brows of a millimeter or two is sometimes seen with injection, we believe that the impression of elevation is largely illusory, based on greater light reflection from the now filled and rounder brow. In any event, trying to lift brows with volume may provide a slight elevation at the cost of an unnaturally overfilled eye.








Coleman SR. Hyaluronic acid fillers. Plastic and Reconstructive Surgery. 2006;117(2):661–665.
Goldwyn RM. The paraffin story. Plastic and Reconstructive Surgery. 1980;65(4):517–524.
Kolle FS. Plastic and cosmetic surgery. New York: Appelton; 1911.
Lambros VS. Observations on periorbital and midface aging. Plastic and Reconstructive Surgery. 2007;120(5):1367–1376. discussion 1377
Lambros V. Volumizing the brows with HA fillers. Aesthetic Surgery Journal. 2009;29:177–179.
Mancini R, Taban M, Lowinger A, et al. Use of hyaluronic acid gel in the management of paralytic lagophthalmos: the hyaluronic acid gel ‘gold weight’. Ophthalmic Plastic and Reconstructive Surgery. 2009;25:1.
[/level-membership-for-dermatology-category][not-level-membership-for-dermatology-category]
15 Volumetric treatment of the brows
Summary and Key Features
• Orbits that are large, round, and hollow are associated with age, not youth
• Young orbits are almond shaped, the bone is not visible and there may be considerable fullness of the upper lid
• The same configurations that are seen in younger patients may be perceived as looking old in older ones
• Communication is difficult in the periorbital area. Many patients want the eye ‘lifted’ or skin and fat removed since that is what they have been told is done. Moreover, some patients like the hollow and defined look as it may look more dramatic and makeup can be used more liberally
• The author prefers using a trial of local anesthetic in the upper lid to demonstrate the visual effect of filling in the upper lids and brow. If the patient likes the look, the injection is done immediately; there is no need to wait. Local anesthetic provides a vasoconstricted environment. There is no better way of communicating the visual effect of the brow fill
• Putting in the local anesthetic and avoiding overfills and fluid blobs in the upper lid is difficult to do well and easily; some practice is involved. The area is massaged and a few minutes should elapse to let the local distribute before showing the patient
• Underfill is better than overfill. This is not a method to fill in an abundance of skin, though the fill does inflate some skin. Nor is it a method to lift brows, though the brow can elevate in a few patients. Someone with full heavy lids is not a candidate for this procedure
• The author favors non-cross-linked hyaluronic acid (HA) products in the brow as they have more projection
• One should expect at least 2 years’ duration in this location with HA products
• The injector should always be aware of the presence of the globe. Some upper orbits are very shallow and the globe is immediately adjacent to the bone
The ‘local preview’
What has proved extremely useful is the ‘local preview’, as I have previously described (2009); a milliliter or two of % epinephrine is injected into the brow with the intention of visualizing the effect of filling the area and also to make it numb and vasoconstricted (Fig. 15.1). With the use of an ice cube for the initial injections, this is almost painless.
[/not-level-membership-for-dermatology-category]
