[level-membership-for-radiology-category] Epigastric hernias arise above umbilicus and below xiphoid process
Hypogastric hernias arise below umbilicus
• Incisional hernias develop at prior abdominal wall incision
• CT: Most accurate test for detection of ventral hernias
Defect in musculofascial layers of abdominal wall through which omentum ± bowel protrude anteriorly
PATHOLOGY
• Depending on hernia type, ventral hernias may be due to either acquired or congenital factors
Incisional hernias: Acquired hernias at the site of prior surgery, incision, or abdominal wall injury
– May be related to previous abdominal surgery, laparoscopy, peritoneal dialysis, or stab wound
Epigastric and hypogastric hernias: Possible congenital predisposition due to weakness of linea alba
– Acquired risk factors include obesity, increased intraabdominal pressures, and abdominal wall strains
CLINICAL ISSUES
• Incisional hernias usually occur during first 4 months after surgery, but can develop many years later
• Ventral hernias do not close spontaneously and almost always enlarge over time
• Incarceration and strangulation are common
• Some debate about treatment of asymptomatic ventral hernias, but in principle, surgical closure is recommended due to risk of incarceration and strangulation
Tension-free mesh repair is now gold standard
(Left) Axial CECT demonstrates a hernia containing small bowel arising in the midline above the umbilicus and below the xiphoid, characteristic of an epigastric hernia. The bowel within the hernia appears normal, without evidence of obstruction or ischemia.
(Right) Axial CECT in a younger woman with nausea and vomiting due to a strangulated hernia shows herniation of small bowel through a laparoscopy port with bowel obstruction. Bowel distal to the hernia is collapsed .
(Left) Axial CECT in a middle-aged woman with nausea and vomiting shows a ventral hernia with strangulated, obstructed small bowel as well as ascites , suggesting bowel ischemia.
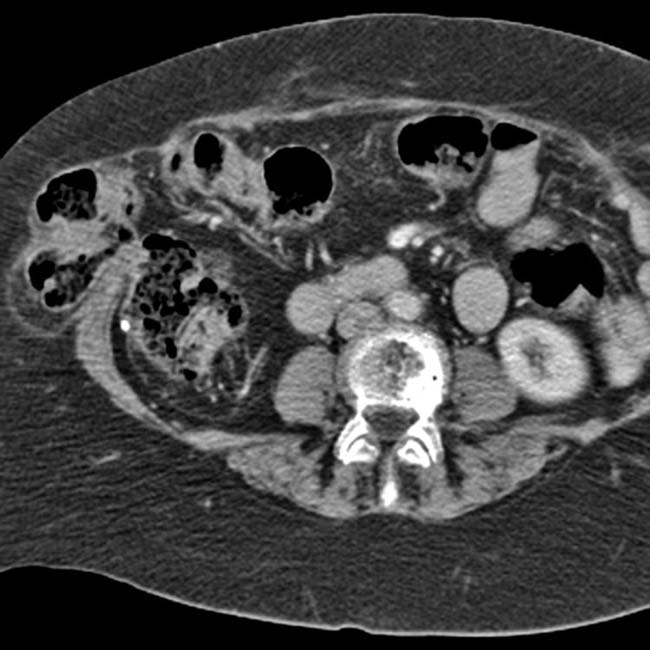
(Right) Axial CECT demonstrates a ventral hernia containing a markedly thickened, hypoenhancing loop of small bowel . The hernia was not reducible at clinical examination, and the bowel loop within the hernia sac was found to be ischemic at surgery.
Axial CECT shows herniation of small bowel through a wide ventral hernia at the site of a prior paramedian surgical incision.
Axial CECT shows ventral hernia containing ascites and varices in a patient with cirrhosis (umbilicus at a lower section).
Axial CECT shows a lateral ventral hernia.
Axial CECT shows a lateral incisional hernia containing colon.
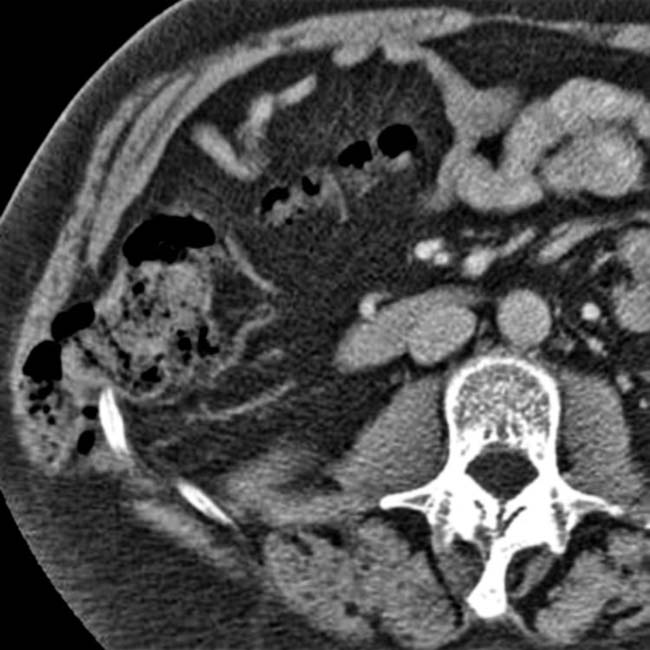
Axial CECT in an older, obese woman, with a bulge that increases with straining, shows a large defect in the anterior abdominal wall containing nonobstructed bowel.
Axial CECT shows a ventral incisional hernia with bowel obstruction. Axial CECT shows a “knuckle” of small bowel herniated through a defect in the anterior abdominal wall.
Axial CECT in the same patient shows that the small intestine proximal to the herniated segment is dilated , while that which is distal to the hernia is collapsed , indicating that the herniated bowel is obstructed.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Epigastric hernias arise above umbilicus and below xiphoid process
Hypogastric hernias arise below umbilicus
• Incisional hernias develop at prior abdominal wall incision
• CT: Most accurate test for detection of ventral hernias
Defect in musculofascial layers of abdominal wall through which omentum ± bowel protrude anteriorly
PATHOLOGY
• Depending on hernia type, ventral hernias may be due to either acquired or congenital factors
Incisional hernias: Acquired hernias at the site of prior surgery, incision, or abdominal wall injury
– May be related to previous abdominal surgery, laparoscopy, peritoneal dialysis, or stab wound
Epigastric and hypogastric hernias: Possible congenital predisposition due to weakness of linea alba
– Acquired risk factors include obesity, increased intraabdominal pressures, and abdominal wall strains
CLINICAL ISSUES
• Incisional hernias usually occur during first 4 months after surgery, but can develop many years later
• Ventral hernias do not close spontaneously and almost always enlarge over time
•
Buy Membership for Radiology Category to continue reading. Learn more here





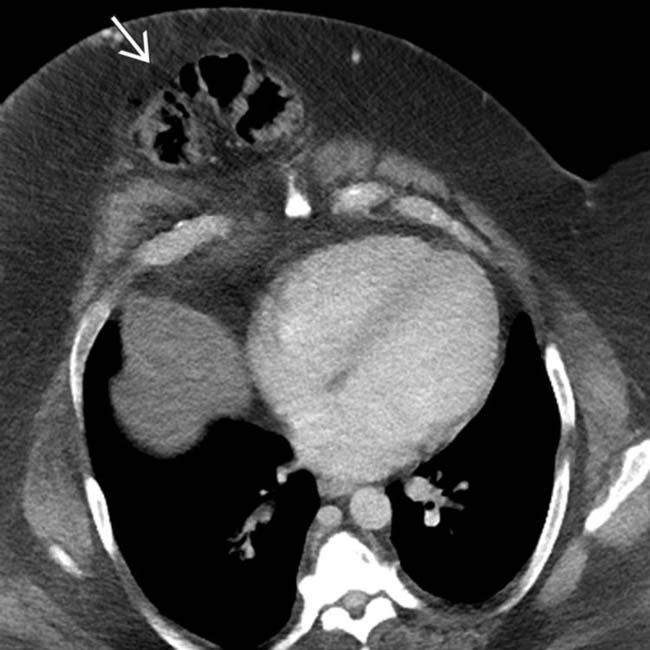
 containing small bowel arising in the midline above the umbilicus and below the xiphoid, characteristic of an epigastric hernia. The bowel within the hernia appears normal, without evidence of obstruction or ischemia.
containing small bowel arising in the midline above the umbilicus and below the xiphoid, characteristic of an epigastric hernia. The bowel within the hernia appears normal, without evidence of obstruction or ischemia.
 with bowel obstruction. Bowel distal to the hernia is collapsed
with bowel obstruction. Bowel distal to the hernia is collapsed  .
.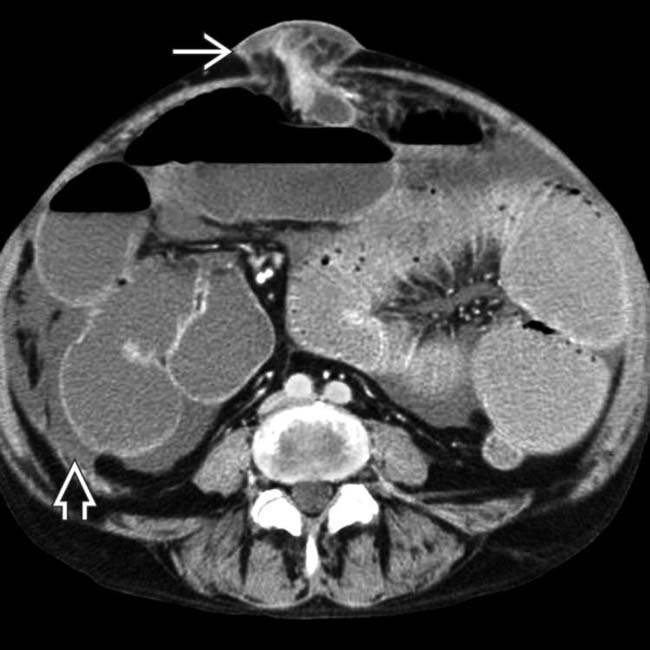
 with strangulated, obstructed small bowel as well as ascites
with strangulated, obstructed small bowel as well as ascites  , suggesting bowel ischemia.
, suggesting bowel ischemia.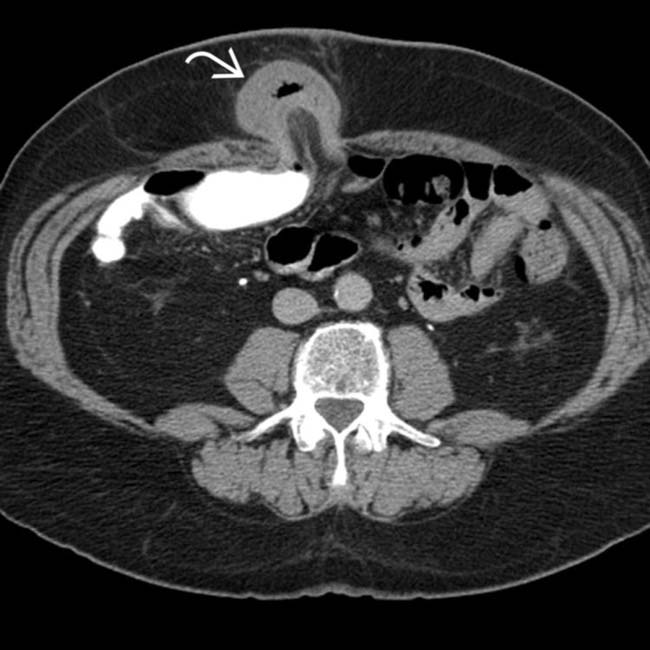
 . The hernia was not reducible at clinical examination, and the bowel loop within the hernia sac was found to be ischemic at surgery.
. The hernia was not reducible at clinical examination, and the bowel loop within the hernia sac was found to be ischemic at surgery.


 containing nonobstructed bowel.
containing nonobstructed bowel.
 in the anterior abdominal wall.
in the anterior abdominal wall.
 , while that which is distal to the hernia is collapsed
, while that which is distal to the hernia is collapsed  , indicating that the herniated bowel is obstructed.
, indicating that the herniated bowel is obstructed.