Ovarian Vein Thrombosis
Synonyms/Description
Etiology
Ultrasound Findings
Differential Diagnosis
Clinical Aspects and Recommendations
Figures
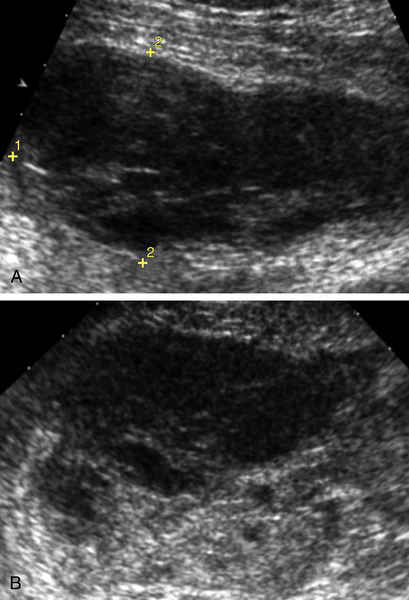
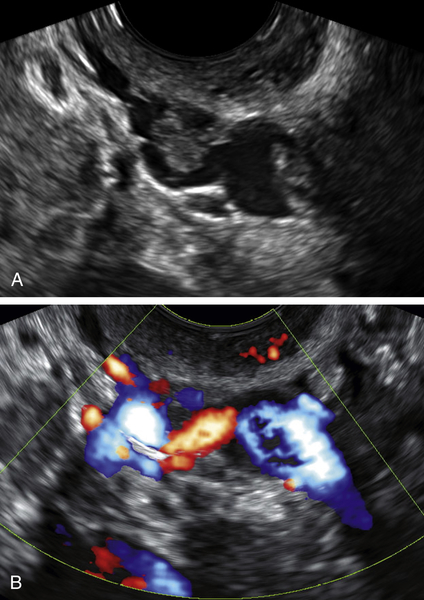
Figure O4-2 A and B, Longitudinal view of the right external iliac containing multiple clots incidentally noted on a gynecologic scan. B shows color Doppler of the vein in the same projection, showing defects within the color consistent with clot. The thrombosis was confirmed with contrast CT, and the patient was anticoagulated.
Suggested Reading
Bilgin M., Sevket O., Yildiz S., Sharifov R., Kocakoc E. Imaging of postpartum ovarian vein thrombosis. Case Rep Obstet Gynecol. 2012;2012:134603.
Dewdney S.B., Benn T., Rimel B.J., Gao F., Saad N., Vedantham S., Mutch D.G., Zighelboim I. Inferior vena cava filter placement in the gynecologic oncology patient: a 15-year institutional experience. Gynecol Oncol. 2011;121:344–346.
Sharma P., Abdi S. Ovarian vein thrombosis. Clin Radiol. 2012;67:893–898.
Stafford M., Fleming T., Khalil A. Idiopathic ovarian vein thrombosis: a rare cause of pelvic pain—case report and review of literature. Aust N Z J Obstet Gynaecol. 2010;50:299–301.