141
Vascular malformations

Capillary malformations can involve segments of the skin.
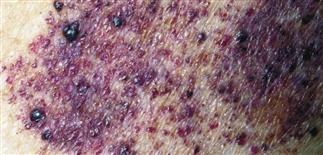
Capillary malformations develop a cobblestone appearance to the surface with age.

Laser treatment can be very effective to treat large segmental port-wine stains.

Children with port-wine stains involving the first division of the trigeminal nerve are at risk for central nervous system, ocular, and bony involvement (Sturge–Weber syndrome).
DESCRIPTION
Anomalies of blood and lymphatic vessels due to abnormal development and morphogenesis.
HISTORY
• Present at birth but might not become noticeable for months, sometimes years. • Classified by vessel type (capillary, venous, arterial, lymphatic, mixed (common), arteriovenous) and flow characteristics (slow or fast). • Increase in size in proportion to patient’s somatic growth. • Most sporadic, not inherited. Inherited types include multiple glomuvenous malformation, blue rubber bleb nevus syndrome (both autosomal dominant). • Ten percent of infants with large facial capillary malformations, especially involving trigeminal nerve V1 (forehead and upper eyelid), are at risk for underlying eye (glaucoma in 30–70%) and central nervous system (seizures in 70–80%) involvement (Sturge–Weber syndrome). • Large cervicofacial lymphatic malformations can compromise airway. • Arteriovenous malformations can cause cardiac failure due to shunting; head and neck arteriovenous malformations can cause seizures and focal neurologic deficits. • Capillary malformations can darken with age, develop a cobblestone appearance. • Extensive venous and arterial malformations can involve deeper structures (e.g. muscle) and be a source of local or disseminated coagulopathy. • Vascular malformations may cause alterations in underlying bone and soft tissue, resulting in functional disability. • Lymphatic malformations can be complicated by pain, swelling, intralesional bleeding, infection.
PHYSICAL FINDINGS
• Capillary malformations (slow flow). Macular staining occurs commonly on the eyelids (‘angel kiss’), forehead, and nuchal area (‘stork bite’). Capillary malformations can be more substantial and involve a segment and/or segments of skin innervated by the trigeminal nerve (V1–V3). • Venous malformations (slow flow). Blue and spongy-appearing. Enlarge with Valsalva maneuver. Can be painful. May contain hard calcified nodules called phleboliths. • Lymphatic malformation (slow flow). Small lymphatic channels (microcystic) or large channels (macrocystic) can be localized or diffuse. Lymphangioma circumscripta (microcystic) consists of small (1–5 mm) discrete, clear to blood-tinged papules that look like vesicles (‘frog spawn’). Cystic hygroma (macrocystic) commonly occurs in the cervicofacial region. • Arterial malformations (fast flow). Arterial malformations (aneurysm, stenosis, arteriovenous malformation) can cause minimal skin signs (pink stain), or they can produce massive swelling, ulceration, and necrosis. Arteriovenous malformations can be quiescent for years only to cause disability through blood shunting in puberty. Arteriovenous malformations most common in head and neck region.
TREATMENT
• Pulsed dye laser for capillary malformations. • Compression stockings, low molecular weight heparin, hydrotherapy, massage, and physical therapy for coagulopathies associated with venous malformations. • Laser surgery, surgical resection, embolization, and sclerosis are used alone or in combination to treat complicated vascular malformations.






