Chapter 5 Ultrasound in emergency medicine
Emergency department ultrasound continues to be an area of rapidly expanding importance in the practice of emergency medicine. It is a safe and reliable technology that is relatively inexpensive and easily learned.
BASIC PHYSICAL PRINCIPLES
Piezoelectric effect
Artificially grown crystals are commonly used for modern transducers. These are treated with high temperatures and strong electric fields to produce the piezoelectric properties necessary to generate sound waves. These properties mean that, when a crystal in the ultrasound transducer has an applied voltage, the crystal is deformed and produces a pressure, i.e. the transducer sends an ultrasound. Conversely, an applied pressure received by the transducer deforms the crystal to produce a voltage. This voltage is then analysed by the system. In essence, the piezoelectric crystal acts as both speaker and microphone.
Most transducers use many small crystal elements for the formation of each pulse.
Image resolution
Interaction of sound with tissue
| Soft tissue/air interface | 99% reflected |
| Soft tissue/bone interface | 40% reflected |
| Liver/kidney interface | 2% reflected |
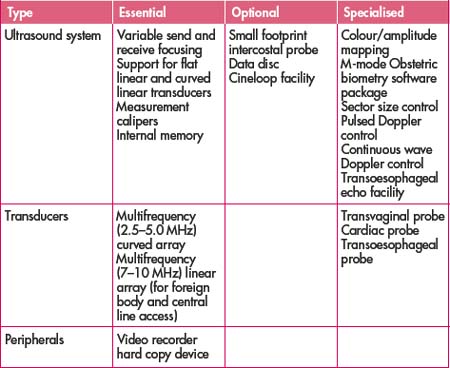
ULTRASOUND EQUIPMENT
Types of transducers
Linear and curved array transducers are most commonly used in general ultrasound.
Curved array transducer is also constructed with multiple small crystal elements, except that the face of the transducer is convex. This results in a wider field of view at the bottom of the image and narrower image in the near field of view.
COMMON APPLICATIONS IN THE EMERGENCY DEPARTMENT
Focused assessment for sonography in trauma (FAST)
In recent years the FAST scan has emerged as a useful diagnostic test in the evaluation of the patient with blunt abdominal trauma (see Figure 5.1). The aim of FAST is to detect fluid as represented by anechoic (black) areas, particularly haemopericardium, haemoperitoneum and haemothorax. Ideally the FAST examination is performed in 5 minutes or less.
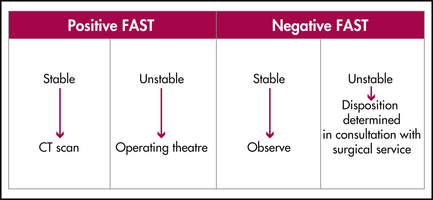
A review of 11 studies has shown FAST to be a highly specific tool, with specificity of 98%. The sensitivity in these studies was 89%. It has mostly eliminated the initial use of diagnostic peritoneal lavage in many trauma centres. The advantages and disadvantages of FAST are shown in Table 5.2.
Table 5.2 Advantages and disadvantages or limitations of FAST
| Advantages | Disadvantages |
|---|---|
FAST involves a minimum of four views.
Abdominal aortic scan
If an aneurysm is present several additional items need to be assessed, including:
OTHER APPLICATIONS
Table 5.3 Procedural applications for emergency department ultrasound
| Application | Strengths and uses | Limitations |
|---|---|---|
TRAINING, CREDENTIALLING AND QUALITY REVIEW
Initial training
Accurate training and experience are vital to accurate ultrasound examination. The format of courses instructing individuals in emergency department ultrasound depends on the number of primary applications being taught. A single day course has proved to be adequate for those learning basic physics, knobology and how to perform FAST and abdominal aorta assessment. Sessions should include live scanning with appropriate models such as chronic ambulatory peritoneal dialysis patients (to simulate haemoperitoneum) or stable patients with aortic aneurysms.
Credentialling process and maintenance of standards
Individual institutions can adopt or adapt these standards as determined by local needs.
Documentation
The results of emergency department ultrasound examinations that are used to facilitate patient care decisions should be documented in the patient’s clinical record.
The following are basic items that should be documented:
Findings incidental to the examination should also be documented and the patient informed of them.
ACEM Policy Document. Use of bedside ultrasound by emergency physicians. Online. Available: http://www.acem.org.au; July 1999.
ACEM Policy Document. Credentialing for ED ultrasonography. Online. Available: http://www.acem.org.au; July 2000.
ACEP Policy Statement. Use of ultrasound imaging by emergency physicians. Online. Available: http://www.acep.org; June 2001.
Australian Institute of Ultrasound. Ultrasound in emergency medicine handbook. Mermaid Beach, Queensland: Australian Institute of Ultrasound; 2001.
Eastern Association for Surgery of Trauma (FAST) Practice Management Guidelines Work Group. Evaluation of blunt abdominal trauma. Online. Available: http://www.east.org; 2001.



