74 Ulnar nerve palsy
Salient features
History
• Repeated trivial trauma to the elbow; the patient feels the ‘funny bone’
• Patient may be immobilized in the orthopaedic ward and use the elbows to shuffle in bed
• History of fracture of the upper arm in childhood (supracondylar fractures of humerus in childhood has an insidious course and can result in acute ulnar nerve palsy 20–30 years later: tardy-ulnar palsy).
Examination
• Generalized wasting of the small muscles of the hand.
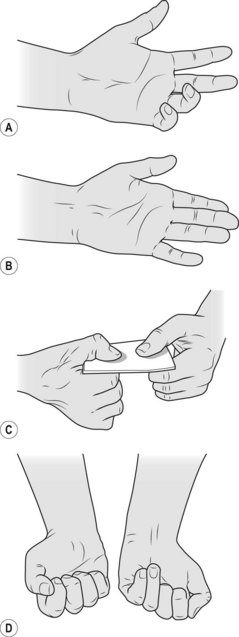
• There may be features of ulnar claw hand: hyperextension at the metacarpophalangeal joints and flexion at the interphalangeal joints of the fourth and fifth fingers (Fig. 74.1).
• There is weakness of movement of the fingers, except that of the thenar eminence.
• There is sensory loss over the medial one and half fingers.
Advanced-level questions
What are the muscles supplied by the ulnar nerve?
How would you test the adductor pollicis?
Ask the patient to grip a folded newspaper between the thumb and index finger of each hand so that the thumbs are uppermost—this causes the adductor to contract. When the muscle is paralysed, the thumb is incapable of adequate adduction and becomes flexed at the interphalangeal joint caused by contraction of the flexor pollicis longus (innervated by the median nerve). This is known as Froment’s sign (Fig. 74.1C).




