[level-membership-for-pathology-category]
CHAPTER 6 TUMORS AND TUMOR-LIKE LESIONS
PEDIATRIC ‘BLASTOMAS’ / ‘SMALL ROUND CELL’ TUMORS
INTRODUCTION

HANDLING OF PEDIATRIC TUMOR SPECIMENS










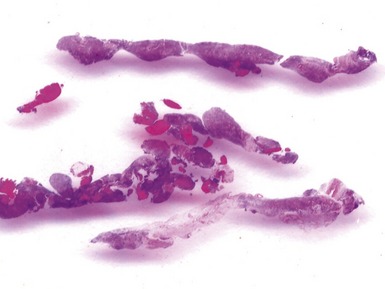
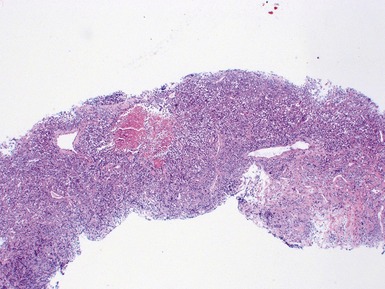
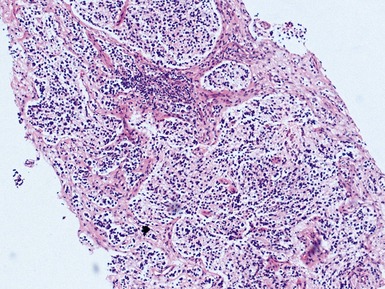
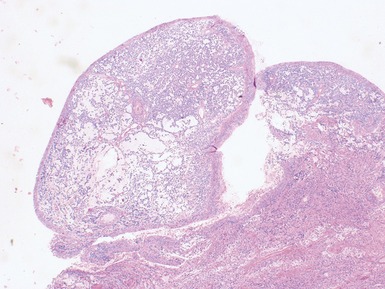
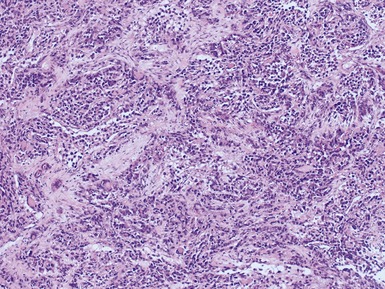
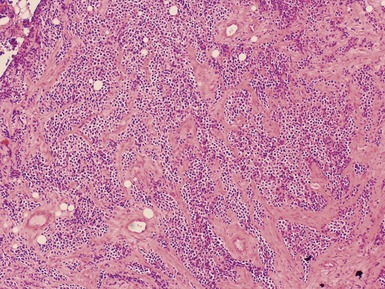
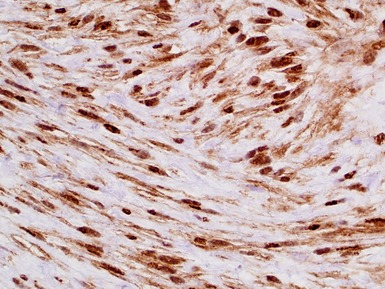
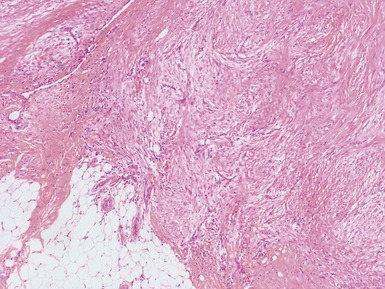
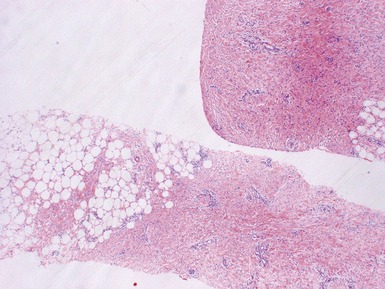
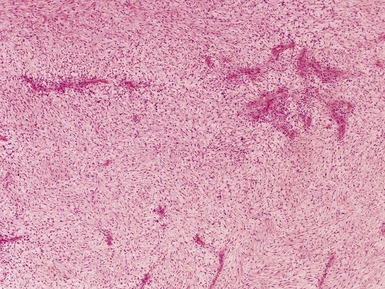
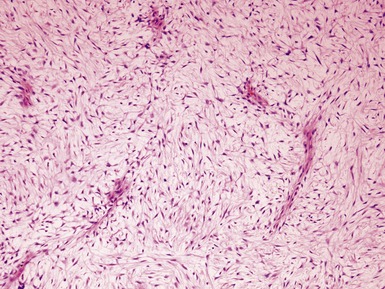
Issues specific to needle core biopsy specimen interpretation in pediatric tumor diagnosis (Figs 6.1, 6.2)





PERIPHERAL NEUROBLASTIC TUMORS (NTS)







NEUROBLASTOMA
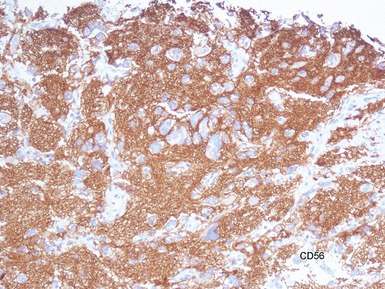
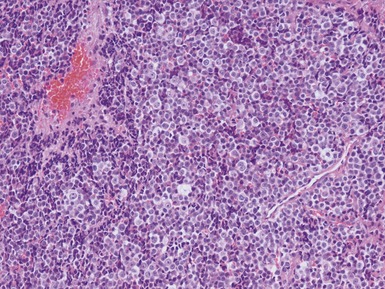
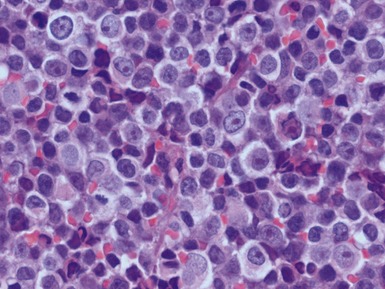
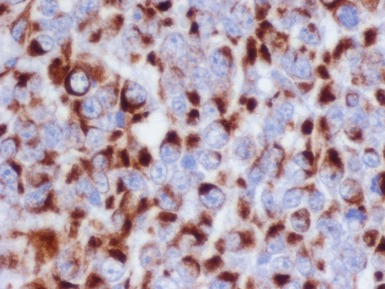
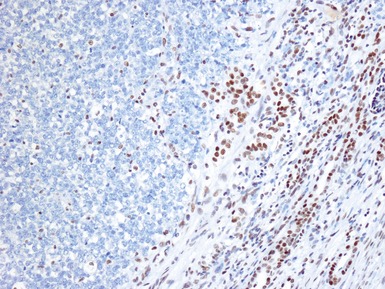
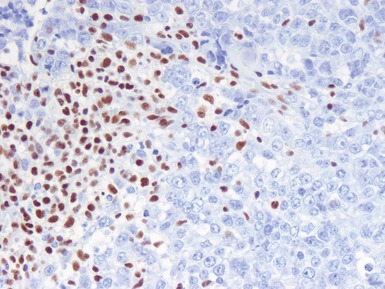
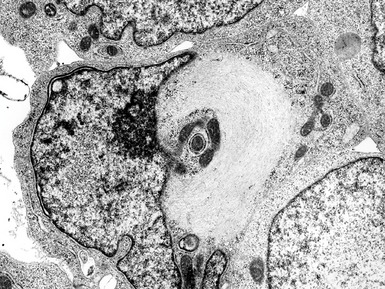
Histopathological features (Figs 6.3–6.8)





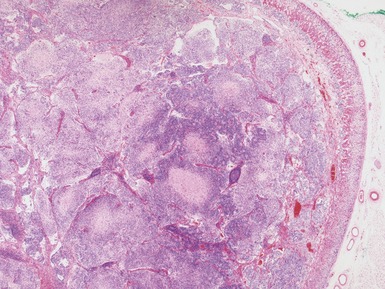
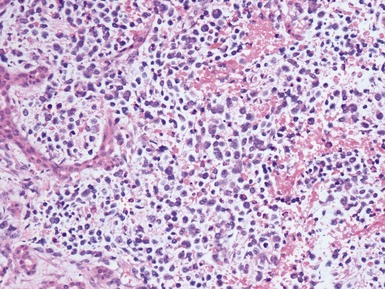
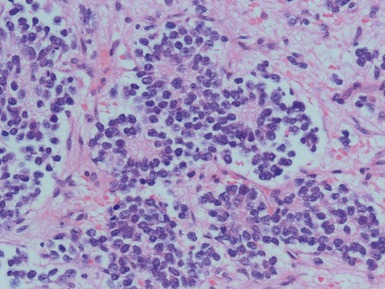
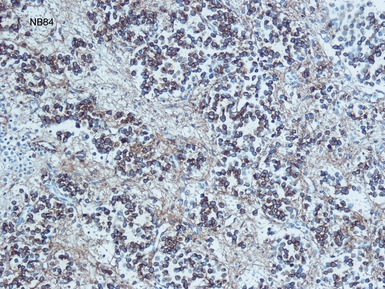
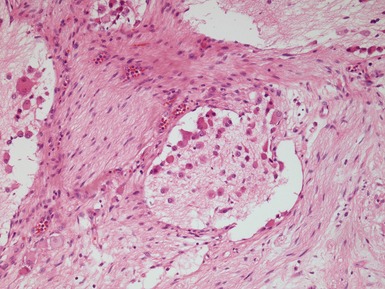
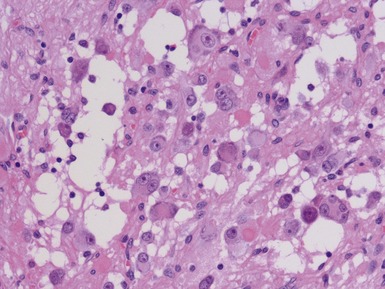
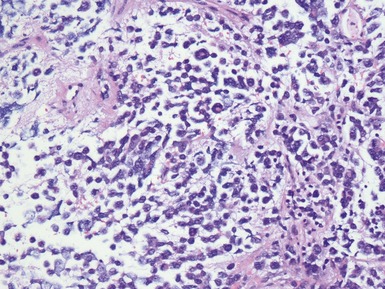
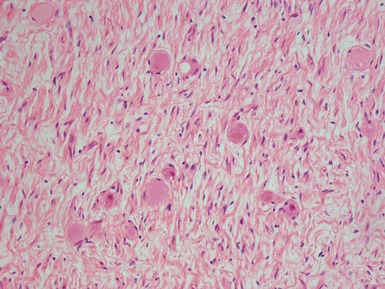
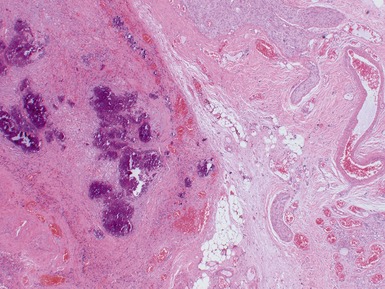
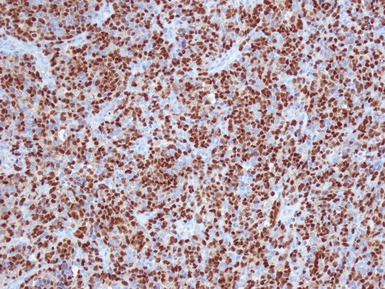
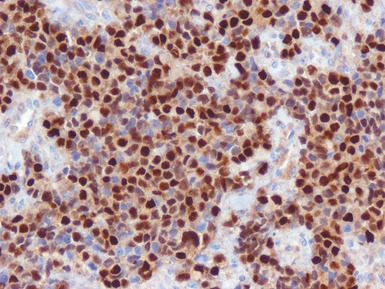
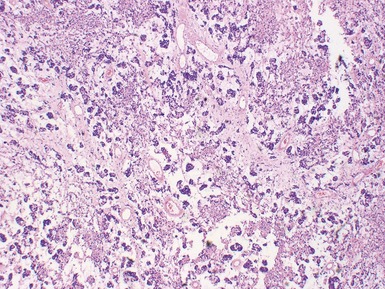
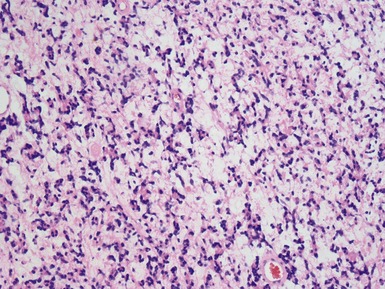
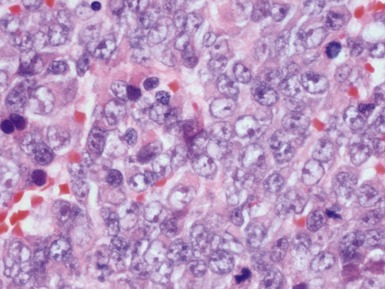
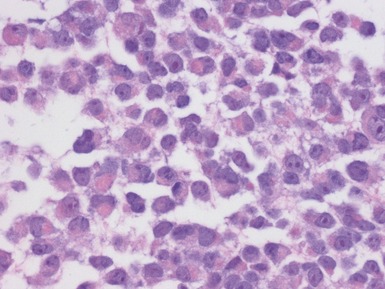
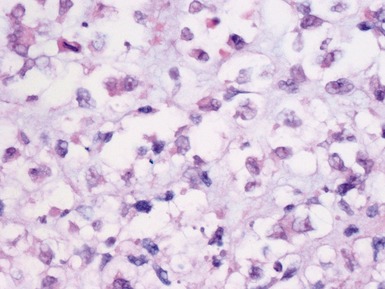
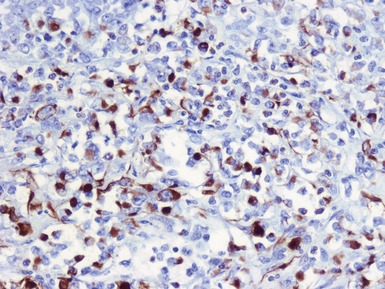
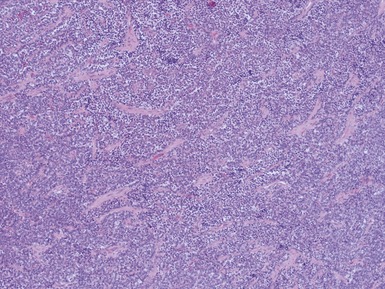
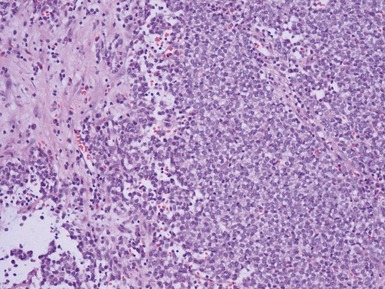
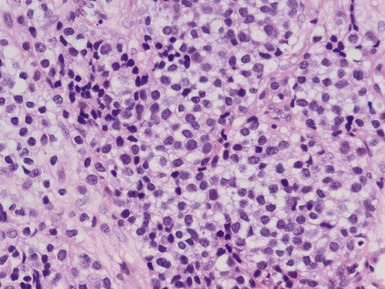
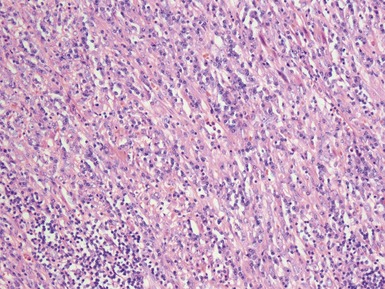
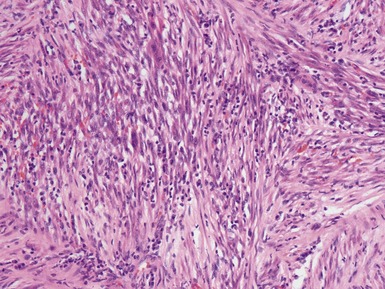
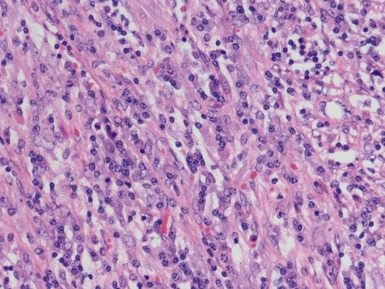
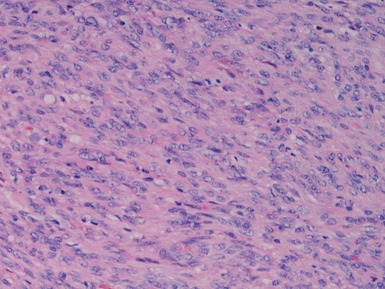
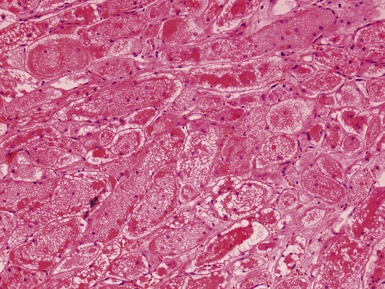
Figs 6.5–6.8 Photomicrographs of cases of neuroblastoma, demonstrating tumor composed of sheets and nests of small ovoid cells within a variably prominent neurofibrillary background.









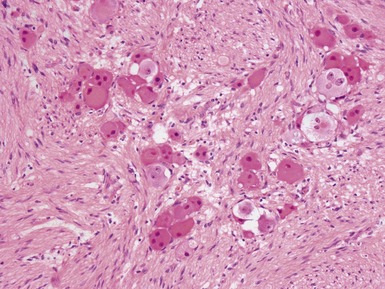
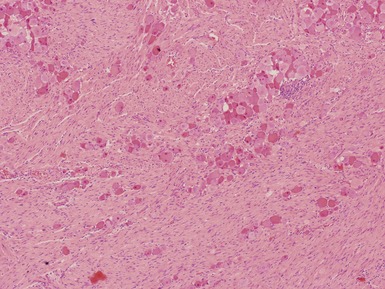
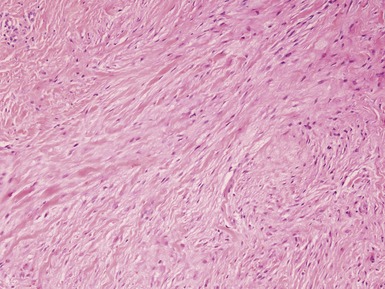
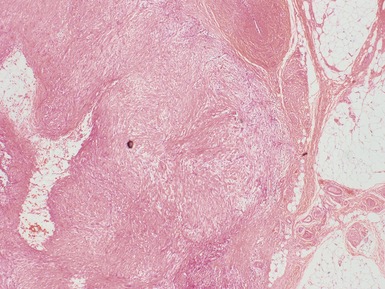
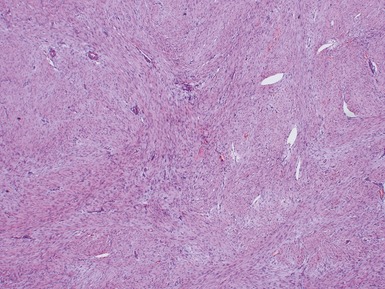
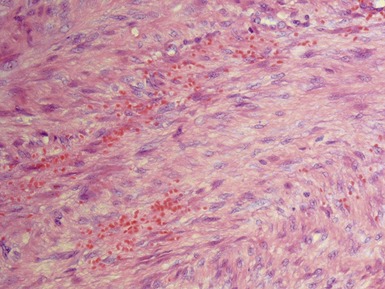
GANGLIONEUROBLASTOMA, INTERMIXED (Figs 6.11–6.14)



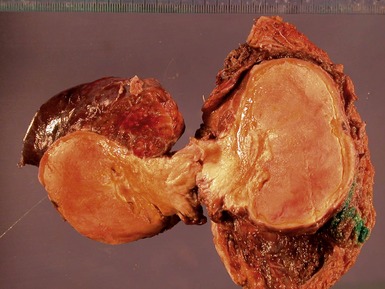
GANGLIONEUROBLASTOMA, NODULAR (Figs 6.15–6.17)





NEUROBLASTOMA (SCHWANNIAN STROMA POOR), NOS
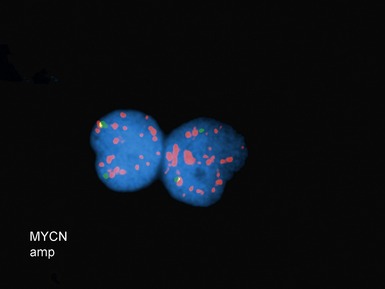
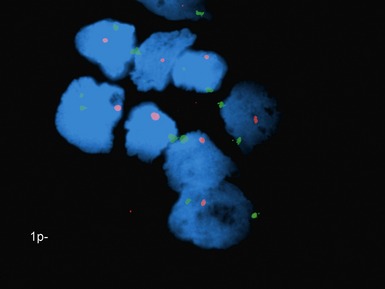
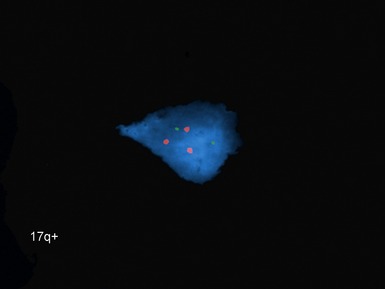
Additional investigations
















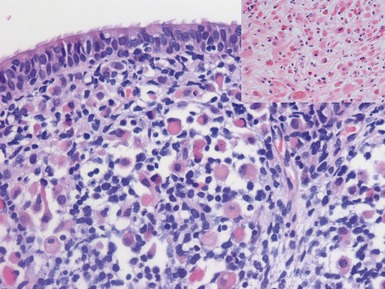
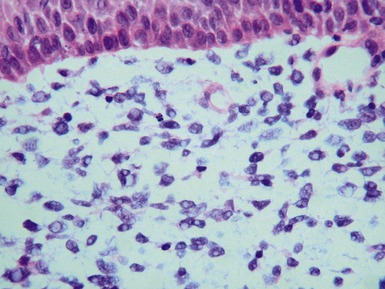
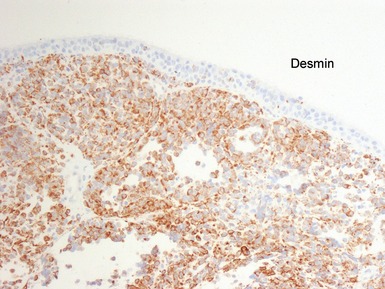
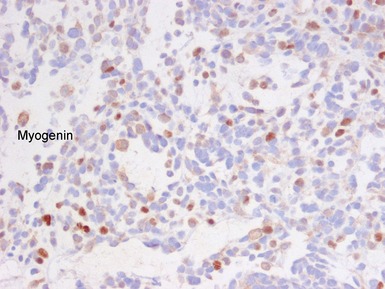
EMBRYONAL RHABDOMYOSARCOMA




Histopathological features (Figs 6.26–6.31)











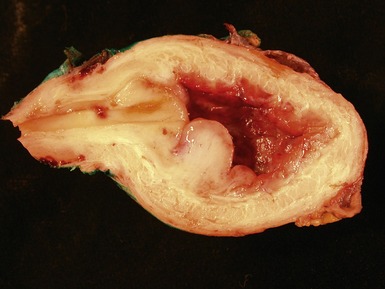

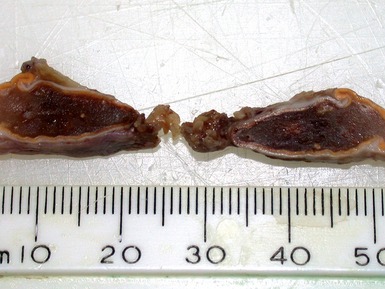
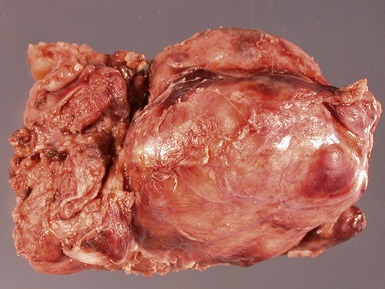
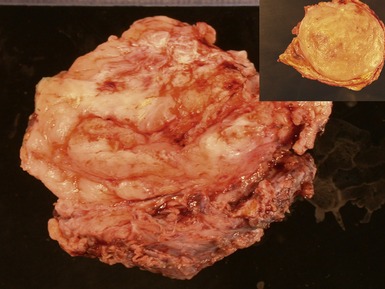
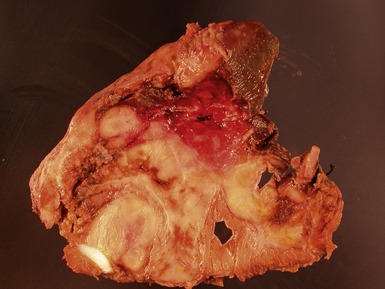
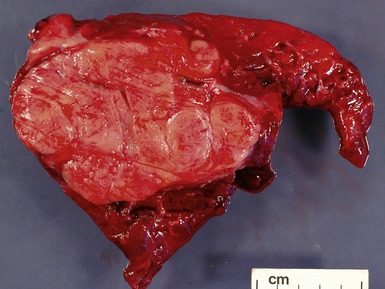
Figs 6.26–6.27 Macroscopic photographs of bladder and soft-tissue rhabdomyosarcomas, demonstrating poorly circumscribed, infiltrating lesions of viable cream-colored tumor.



Differential diagnosis and pitfalls






ALVEOLAR RHABDOMYOSARCOMA







Differential diagnoses and pitfalls



EXTRASKELETAL MYXOID CHONDROSARCOMA











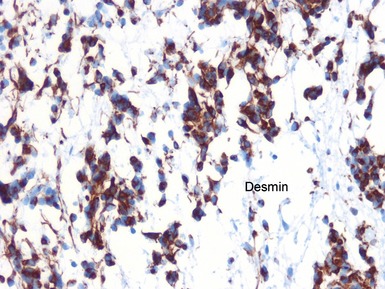
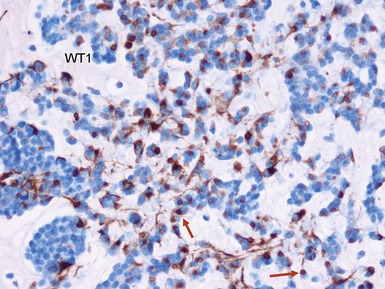
DESMOPLASTIC SMALL ROUND CELL TUMOR











EXTRARENAL MALIGNANT RHABDOID TUMOR

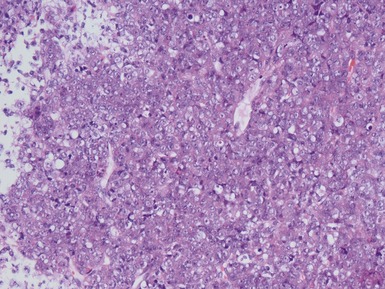
Histopathological features (Figs 6.44–6.49)



























LIPOMATOUS TUMORS
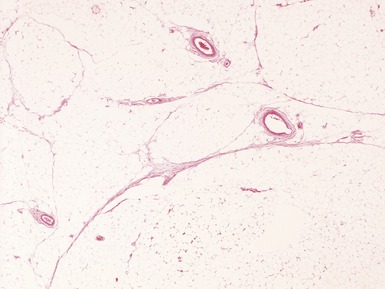
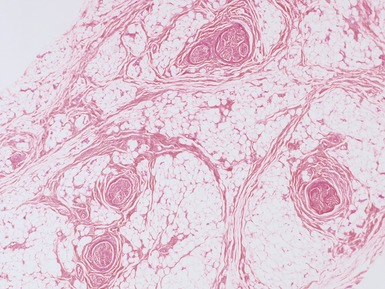
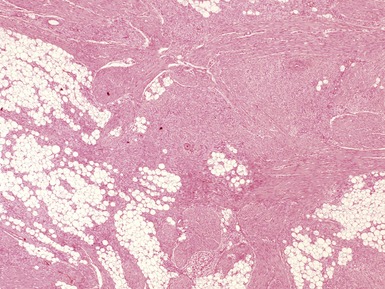
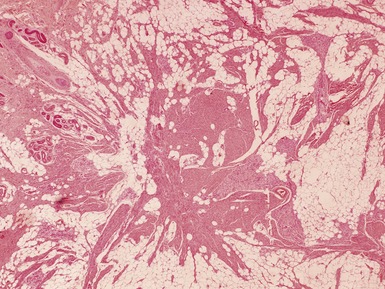
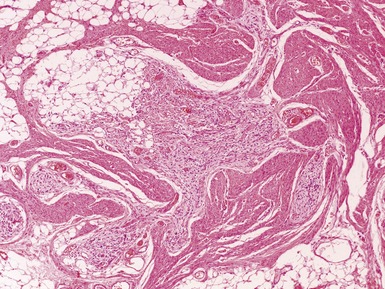
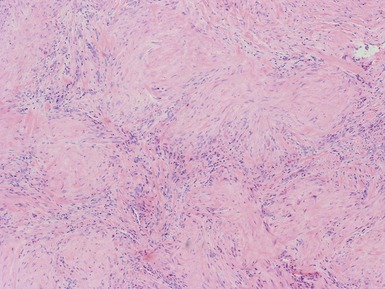
LIPOBLASTOMA / LIPOBLASTOMATOSIS








LIPOMA






























SPINDLE CELL TUMORS
NODULAR FASCIITIS






PROLIFERATIVE FASCIITIS / MYOSITIS




















MYOSITIS OSSIFICANS PROGRESSIVA / FIBRODYSPLASIA OSSIFICANS PROGRESSIVA




FIBROUS HAMARTOMA OF INFANCY






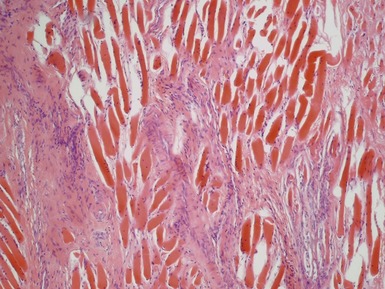
MYOFIBROMATOSIS

Clinical features












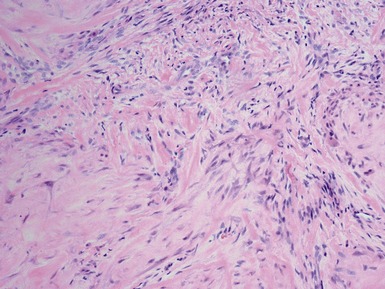


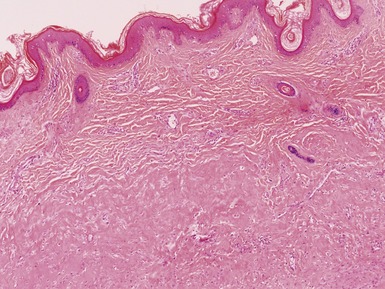
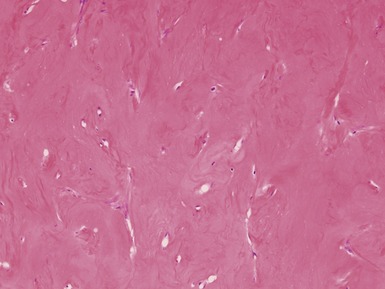
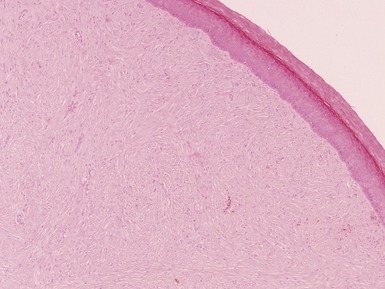
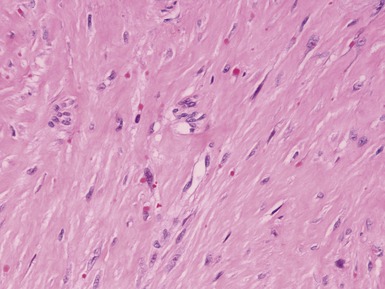
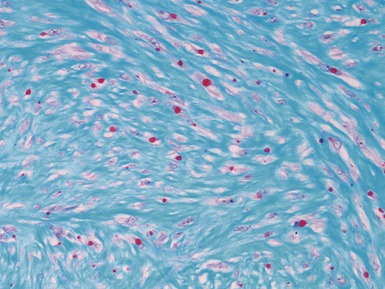
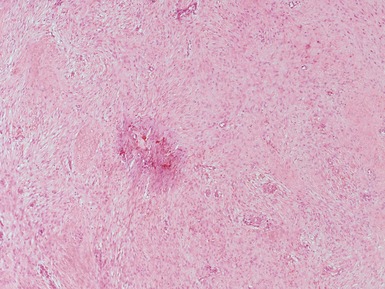
JUVENILE HYALINE FIBROMATOSIS





INCLUSION BODY FIBROMATOSIS











CALCIFYING APONEUROTIC FIBROMA




ANGIOMYOFIBROBLASTOMA







SUPERFICIAL FIBROMATOSES
Clinical features




DESMOID-TYPE (AGGRESSIVE) FIBROMATOSIS









LIPOFIBROMATOSIS




GARDNER FIBROMA










INFLAMMATORY MYOFIBROBLASTIC TUMOR






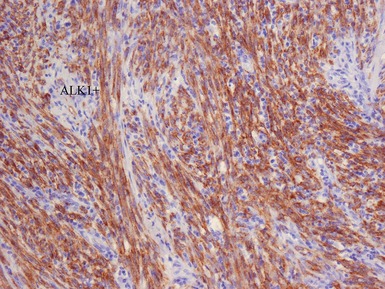
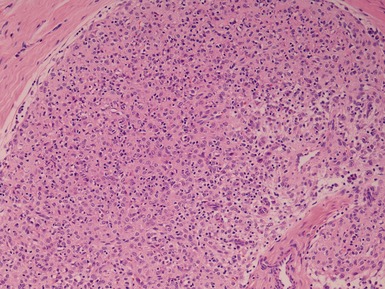
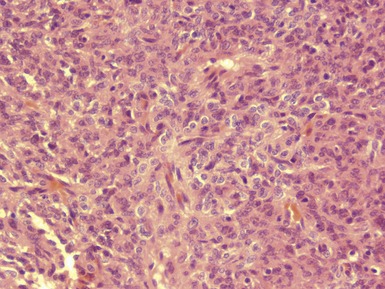
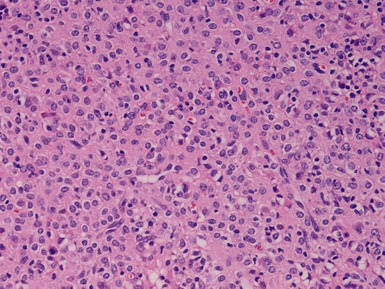
Histopathological features (Figs 6.87–6.91)










LOW GRADE MYOFIBROBLASTIC SARCOMA




CONGENITAL / INFANTILE FIBROSARCOMA













LOW GRADE FIBROMYXOID SARCOMA




































[/level-membership-for-pathology-category][not-level-membership-for-pathology-category]
CHAPTER 6 TUMORS AND TUMOR-LIKE LESIONS
PEDIATRIC ‘BLASTOMAS’ / ‘SMALL ROUND CELL’ TUMORS
INTRODUCTION
HANDLING OF PEDIATRIC TUMOR SPECIMENS
Issues specific to needle core biopsy specimen interpretation in pediatric tumor diagnosis (Figs 6.1, 6.2)
PERIPHERAL NEUROBLASTIC TUMORS (NTS)
NEUROBLASTOMA
Histopathological features (Figs 6.3–6.8)
Figs 6.5–6.8 Photomicrographs of cases of neuroblastoma, demonstrating tumor composed of sheets and nests of small ovoid cells within a variably prominent neurofibrillary background.
GANGLIONEUROBLASTOMA, INTERMIXED (Figs 6.11–6.14)
GANGLIONEUROBLASTOMA, NODULAR (Figs 6.15–6.17)
NEUROBLASTOMA (SCHWANNIAN STROMA POOR), NOS
Additional investigations
EMBRYONAL RHABDOMYOSARCOMA
Histopathological features (Figs 6.26–6.31)
Figs 6.26–6.27 Macroscopic photographs of bladder and soft-tissue rhabdomyosarcomas, demonstrating poorly circumscribed, infiltrating lesions of viable cream-colored tumor.
