[level-membership-for-obstetrics-gynecology-category]
Metastatic Tumor to the Ovary
Synonyms/Description
Etiology
Ultrasound Findings
Differential Diagnosis
Clinical Aspects and Recommendations
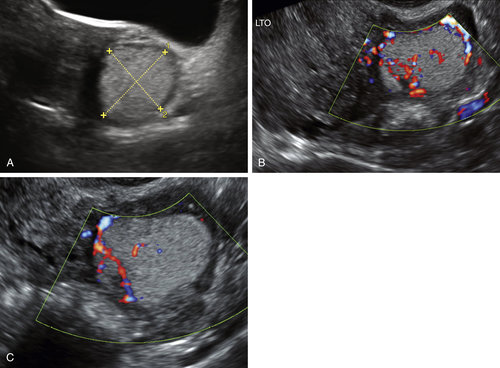
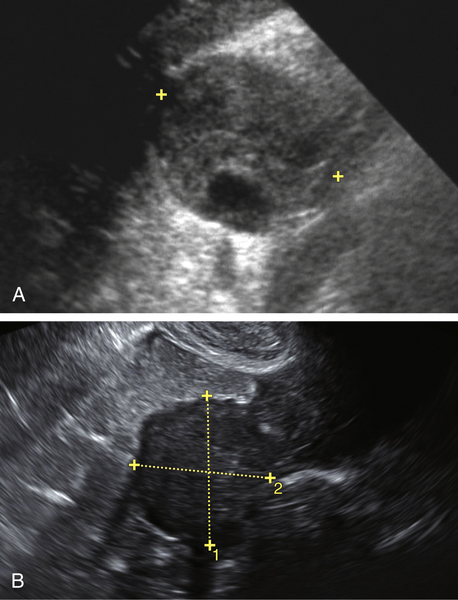
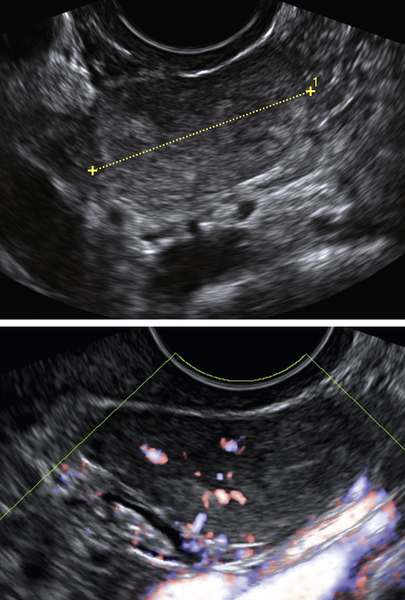
Figures
Suggested Reading
Guzel A.B., Gulec U.K., Paydas S., Khatib G., Gumurdulu D., Vardar M.A., Altintas A. Preoperative evaluation, clinical characteristics, and prognostic factors of nongenital metastatic ovarian tumors: review of 48 patients. Eur J Gynaecol Oncol. 2012;33(5):493–497.
Jain V., Guptay K., Kudvay R., Rodrigues G.S. A case of ovarian metastasis of gall bladder carcinoma simulating primary ovarian neoplasm: diagnostic pitfalls and review of literature. Int J Gynecol Cancer. 2006;16(suppl. 1):319–321.
Koyama T., Mikami Y., Saga T., Tamai K., Togashi K. Secondary ovarian tumors: spectrum of CT and MR features with pathologic correlation. Abdom Imaging. 2007;32:784–795.
Loke T.K.L., Lo S.S., Chan C.S. Case report: Krukenberg tumours arising from a primary duodenojejunal adenocarcinoma. Clin Radiol. 1997;52:154–155.
Yada-Hashimoto N., Yamamoto T., Kamiura S., Seino H., Ohira H., Sawai K., Kimura T., Saji F. Metastatic ovarian tumors: a review of 64 cases. Gynecol Oncol. 2003;89:314–317.
[/level-membership-for-obstetrics-gynecology-category][not-level-membership-for-obstetrics-gynecology-category]
Metastatic Tumor to the Ovary
Synonyms/Description
Etiology
Ultrasound Findings
Differential Diagnosis
[/not-level-membership-for-obstetrics-gynecology-category]
