[level-membership-for-cardiovascular-category]
7 Tricuspid and Pulmonic Valve Disease 








Tricuspid Regurgitation
Scanning Issues
Required parameters to obtain from scanning include the following:




Scanning Notes
 There are problems with color Doppler “quantification” of TR, as there are for color Doppler flow-mapping of any lesions of insufficiency: TR flow-mapping is dependent on gain, angle, position, and jet shape and orientation.
There are problems with color Doppler “quantification” of TR, as there are for color Doppler flow-mapping of any lesions of insufficiency: TR flow-mapping is dependent on gain, angle, position, and jet shape and orientation.
 Retrograde hepatic venous systolic flow reliably establishes that TR is severe.
Retrograde hepatic venous systolic flow reliably establishes that TR is severe.


 Use zoom views liberally to identify the valve lesion responsible for TR.
Use zoom views liberally to identify the valve lesion responsible for TR.

Reporting Issues
 Describe the suspected cause of the TR (i.e., leaflet, annular or RV disease).
Describe the suspected cause of the TR (i.e., leaflet, annular or RV disease).
 Describe the severity of the TR.
Describe the severity of the TR.
 Describe the RV function and geometry.
Describe the RV function and geometry.
 Note that the right ventricular systolic pressure (RVSP) varies by 25% throughout a given day.
Note that the right ventricular systolic pressure (RVSP) varies by 25% throughout a given day.



 Avoid use of the term “trivial” for TR, as it is normal if the valve is structurally normal.
Avoid use of the term “trivial” for TR, as it is normal if the valve is structurally normal.

For any given size of tricuspid valve ERO, there is less regurgitant flow than with MR, as the usual RV–RA gradients are less than the usual left ventricular (LV)–left atrial (LA) gradients. Absence of hepatic venous flow reversal is associated with tricuspid valve EROs (<40 mm2) and therefore, in the final analysis, tricuspid valve–ERO generally adds little to hepatic flow profiling.1
Causes of Tricuspid Regurgitation


 “Functional” (i.e., intact leaflet/chordal/papillary components)
“Functional” (i.e., intact leaflet/chordal/papillary components)


 Myxomatous tricuspid valve disease/tricuspid valve prolapse
Myxomatous tricuspid valve disease/tricuspid valve prolapse
 RV papillary muscle rupture: post-infarction, post-trauma, post-biopsy, post–lead extraction
RV papillary muscle rupture: post-infarction, post-trauma, post-biopsy, post–lead extraction



Ebstein’s Anomaly
 Apical displacement of the septal and or posterior leaflets
Apical displacement of the septal and or posterior leaflets

 “Atrialization” of the right ventricle
“Atrialization” of the right ventricle
 “Tethering” of the anterior leaflet
“Tethering” of the anterior leaflet
 Smaller functional right ventricle
Smaller functional right ventricle
 The amount of TR is usually worst at birth as the PVR is highest
The amount of TR is usually worst at birth as the PVR is highest

Estimation of Right Ventricular Systolic Pressure
Potential problems in estimating the RVSP include the following:
 No TR from which to determine RV–RA gradient
No TR from which to determine RV–RA gradient
 Insufficient TR from which to determine maximum RV–RA gradient
Insufficient TR from which to determine maximum RV–RA gradient




 Inability to record the full TR profile due to inadequate signal
Inability to record the full TR profile due to inadequate signal
The correlation of RV:RA gradient is excellent (r = 0.95; SEE = 7 mm Hg)2 (r = 0.96; SEE = 7 mm Hg),3 but the correlation of jugular venous pressure estimate to catheter RAP is less good (r = 0.80; SEE = 2.3 mm Hg). Clearly, clinical estimate of jugular venous pressure overestimates lower RAPs (<8 cm) and underestimates higher RAPs—sometimes by 40% when the true RAP is 20 mm Hg.
More patients with an elevated RVSP have analyzable TR spectral profiles than do patients (half) with normal RVSP.3 However, an important minority subset of patients with severely elevated RVSP (approximately 20–25% of cases of primary pulmonary hypertension) may not have associated TR to yield an analyzable (complete) TR spectral profile. Overall, the correlation of echocardiographic RVSP to catheter RVSP is quite good (r = 0.93; SEE = 8 mm), but remains influenced by the vagaries of estimating jugular venous pressure and RAP.2
Indications for the management and intervention in tricuspid regurgitation are listed in Boxes 7-1 and 7-2.
Tricuspid Stenosis
Scanning Issues
Required parameters to obtain from scanning include the following:










Tricuspid Atresia




Concerns
 By definition, TS is present when there is a mean gradient of ≥5 mm Hg. The difference between normal tricuspid valve “gradient” by the modified equation (= 4 × V2, = 4 × 0.72 = 2 mm Hg), where V is peak diastolic velocity across the tricuspid valve, and what constitutes significant TS (≥5 mm Hg) is a small difference.
By definition, TS is present when there is a mean gradient of ≥5 mm Hg. The difference between normal tricuspid valve “gradient” by the modified equation (= 4 × V2, = 4 × 0.72 = 2 mm Hg), where V is peak diastolic velocity across the tricuspid valve, and what constitutes significant TS (≥5 mm Hg) is a small difference.


 It is proposed by some that 190/PHT be used for the assessment of TS.
It is proposed by some that 190/PHT be used for the assessment of TS.

Pulmonic Stenosis
The valvular diameter dimension is used to identify the optimal balloon size for dilation.

Indications for the evaluation of pulmonary stenosis are given in Box 7-3 and and indications for balloon valvulopathy are given in Box 7-4.
Summary
 TS requires fusion of at least two commissures.
TS requires fusion of at least two commissures.
 The 5-mm Hg gradient of significant TS is a problem for the modified Bernouilli equation.
The 5-mm Hg gradient of significant TS is a problem for the modified Bernouilli equation.
 Tricuspid insufficiency is readily detected by echocardiography, and its cause is usually apparent.
Tricuspid insufficiency is readily detected by echocardiography, and its cause is usually apparent.
 Alternate imaging modalities generally add little for the assessment of the tricuspid valve.
Alternate imaging modalities generally add little for the assessment of the tricuspid valve.

BOX 7-1 Management of Tricuspid Regurgitation: ACC/AHA 2006 Recommendations




Class III


From ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Am Coll Cardiol. 2006;48(3):e1–e148.
BOX 7-2 Indications for Intervention in Tricuspid Regurgitation: ACC/AHA 2006 Recommendations
Class I
1. Surgery for severe tricuspid regurgitation (TR) is recommended for adolescent and young adult patients with deteriorating exercise capacity (New York Heart Association [NYHA] functional class III or IV). (Level of evidence: C)
2. Surgery for severe TR is recommended for adolescent and young adult patients with progressive cyanosis and arterial saturation less than 80% at rest or with exercise. (Level of evidence: C)
3. Interventional catheterization closure of the atrial communication is recommended for the adolescent or young adult with TR who is hypoxemic at rest and with exercise intolerance due to increasing hypoxemia with exercise, when the tricuspid valve appears difficult to repair surgically. (Level of evidence: C)
Class IIa
1. Surgery for severe TR is reasonable in adolescent and young adult patients with NYHA functional class II symptoms if the valve appears to be repairable. (Level of evidence: C)
2. Surgery for severe TR is reasonable in adolescent and young adult patients with atrial fibrillation. (Level of evidence: C)
Class IIb
1. Surgery for severe TR may be considered in asymptomatic adolescent and young adult patients with increasing heart size and a cardiothoracic ratio of more than 65%. (Level of evidence: C)
2. Surgery for severe TR may be considered in asymptomatic adolescent and young adult patients with stable heart size and an arterial saturation of less than 85%, when the tricuspid valve appears repairable. (Level of evidence: C)
3. In adolescent and young adult patients with TR who are mildly cyanotic at rest but who become very hypoxemic with exercise, closure of the atrial communication by interventional catheterization may be considered when the valve does not appear amenable to repair. (Level of evidence: C)
4. If surgery for Ebstein’s anomaly is planned in adolescent and young adult patients (tricuspid valve repair or replacement), a preoperative electrophysiologic study may be considered to identify accessory pathways. If present, these may be considered for mapping and ablation either preoperatively or at the time of surgery. (Level of evidence: C)
From ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Am Coll Cardiol. 2006;48(3):e1–e148.
BOX 7-3 Evaluation of Pulmonic Stenosis in Adolescents and Young Adults: ACC/AHA 2006 Recommendations
Class I
1. An ECG is recommended for the initial evaluation of pulmonic stenosis in adolescent and young adult patients, and serially every 5–10 years for follow-up examinations. (Level of evidence: C)
2. Transthoracic Doppler echocardiography is recommended for the initial evaluation of pulmonic stenosis in adolescent and young adult patients, and serially every 5–10 years for follow-up examinations. (Level of evidence: C)
3. Cardiac catheterization is recommended in the adolescent or young adult with pulmonic stenosis for evaluation of the valvular gradient if the Doppler peak jet velocity is >3 m/sec (estimated peak gradient >36 mm Hg), and balloon dilation can be performed if indicated. (Level of evidence: C)
From ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Am Coll Cardiol. 2006;48(3):e1–e148.
BOX 7-4 Balloon Valvotomy in Pulmonic Stenosis: ACC/AHA 2006 Recommendations
Class I
1. Balloon valvotomy is recommended in adolescent and young adult patients with pulmonic stenosis who have exertional dyspnea, angina, syncope, or presyncope and an RV–to–pulmonary artery peak-to-peak gradient >30 mm Hg at catheterization. (Level of evidence: C)
2. Balloon valvotomy is recommended in asymptomatic adolescent and young adult patients with pulmonic stenosis and RV–to–pulmonary artery peak-to-peak gradient >40 mm Hg at catheterization. (Level of evidence: C)
From ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Am Coll Cardiol. 2006;48(3):e1–e148.
Transthoracic Echocardiography





Transesophageal Echocardiography


Nuclear
ACCF/ASNC/AHA/ASE/SCCT/SCMR/SNM 2009 Appropriate Use Criteria for Cardiac Radionuclide Imaging7
Evaluation of LV Function
 Assessment of LV function with radionuclide angiography (ERNA or FP RNA)
Assessment of LV function with radionuclide angiography (ERNA or FP RNA)
In absence of recent reliable diagnostic information regarding ventricular function obtained with another imaging modality
Appropriateness criteria: A, appropriate; I, inappropriate; U, uncertain.
LV, left ventricular; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography.
TABLE 7-1 Utility of Different Imaging Modalities and Cardiac Catheterization in the Assessment of Tricuspid Valve Disease
| MODALITY | PROS | CONS/CAVEATS |
|---|---|---|
| Transthoracic Echocardiography |
CMR is the best test to follow right ventricular volumes and systolic function, and tricuspid valve regurgitant volumes and fraction. SSFP sequences will determine the total RV stroke volume, velocity-encoded phase contrast sequences will determine the net forward stroke volume; the difference is the TR volume.
CMR, cardiac magnetic resonance; NA, not applicable; RVEF, right ventricular ejection fraction; SSFP, steady-state free precession; TEE, transesophageal echocardiography; TR, tricuspid regurgitation; TS, tricuspid stenosis; TTE, transthoracic echocardiography.
TABLE 7-2 Utility of Different Imaging Modalities and Cardiac Catheterization in the Assessment of Pulmonic Valve Disease
| MODALITY | PROS | CONS/CAVEATS |
|---|---|---|
| Transthoracic Echocardiography | ||
| Transesophageal Echocardiography | ||
| Cardiac CT | ||
| Cardiac MRI | ||
| LGE sequences: NA | ||
| Nuclear | NA | |
| Chest Radiography | NA | |
| Cardiac Catheterization | NA |
CMR, cardiac magnetic resonance; ECG, electrocardiographic; LGE, late gadolinium enhancement; NA, not applicable; PI, pulmonary insufficiency; PS, pulmonary stenosis; RV, right ventricular; RVEF, right ventricular ejection fraction; RVOT, right ventricular outflow tract; SSFP, steady-state free precession; TEE, transesophageal echocardiography; TTE, transthoracic echocardiography; VEPC, velocity-encoded phase contrast.
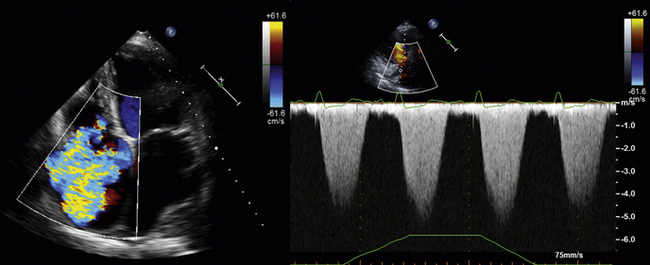
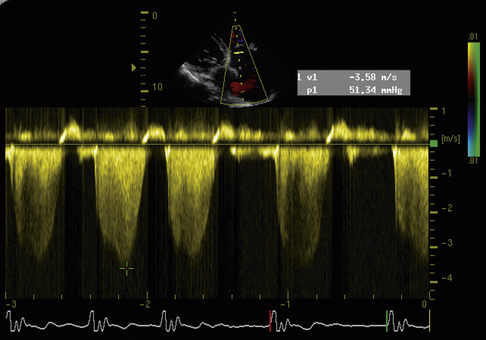
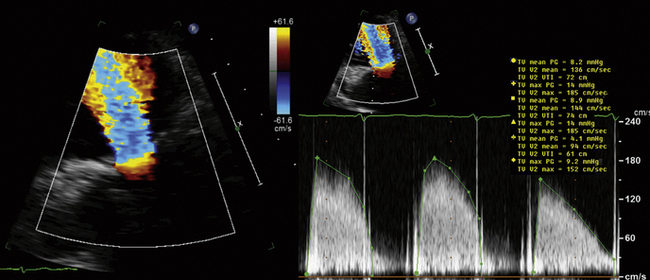
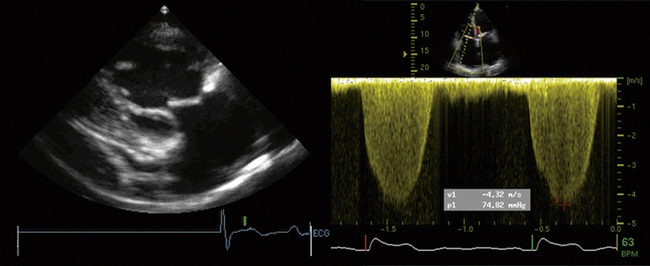
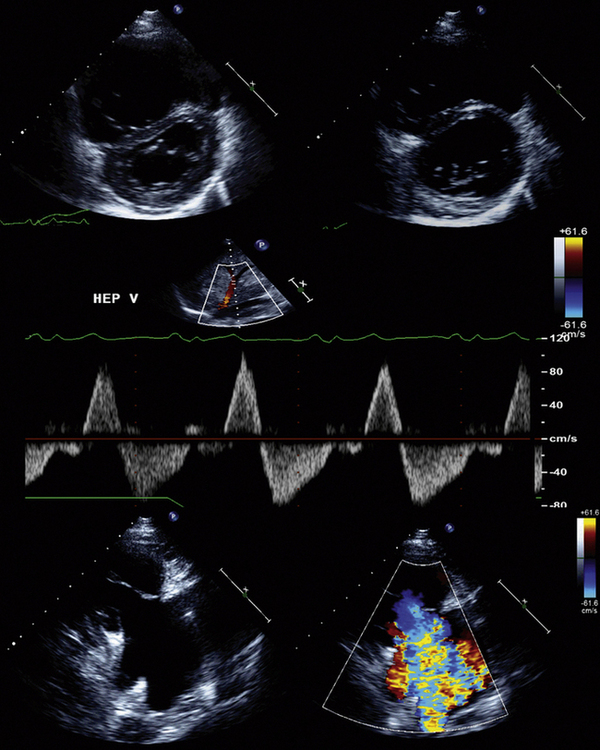
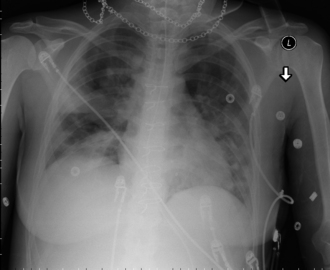
Figure 7-11 Same patient as in Figure 7-10. The sternotomy wires are obvious, and the bioprosthesis stent wires can be seen. There is extensive patchy consolidation due to septic embolization of tricuspid valve vegetations into the lungs.
1. Tribouilloy C.M., Enriquez-Sarano M., Capps M.A., et al. Contrasting effect of similar effective regurgitant orifice area in mitral and tricuspid regurgitation: a quantitative Doppler echocardiographic study. J Am Soc Echocardiogr. 2002;15(9):958-965.
2. Yock P.G., Popp R.L. Noninvasive estimation of right ventricular systolic pressure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation. 1984;70(4):657-662.
3. Currie P.J., Seward J.B., Chan K.L., et al. Continuous wave Doppler determination of right ventricular pressure: a simultaneous Doppler-catheterization study in 127 patients. J Am Coll Cardiol. 1985;6(4):750-756.
4. Bonow R.O., Carabello B.A., Chatterjee K., et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. J Am Coll Cardiol. 2006;48(3):e1-e148.
5. Douglas P.S., Garcia M.J., Haines D.E., et al. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 appropriate use criteria for echocardiography. J Am Coll Cardiol. 2011;57(9):1126-1166.
6. Taylor A.J., Cerqueira M., Hodgson J.M., et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. J Am Coll Cardiol. 2010;56(22):1864-1894.
7. Hendel R.C., Berman D.S., Di Carli M.F., et al. ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 appropriate use criteria for cardiac radionuclide imaging. J Am Coll Cardiol. 2009;53(23):2201-2229.
8. Nishimura R.A., Carabello B.A., Faxon D.P., et al. ACC/AHA 2008 guideline update on valvular heart disease: focused update on infective endocarditis. J Am Coll Cardiol. 2008;52(8):676-685.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
7 Tricuspid and Pulmonic Valve Disease
Tricuspid Regurgitation
Scanning Issues
Required parameters to obtain from scanning include the following:
Scanning Notes
There are problems with color Doppler “quantification” of TR, as there are for color Doppler flow-mapping of any lesions of insufficiency: TR flow-mapping is dependent on gain, angle, position, and jet shape and orientation.
Retrograde hepatic venous systolic flow reliably establishes that TR is severe.
Use zoom views liberally to identify the valve lesion responsible for TR.
Reporting Issues
Describe the suspected cause of the TR (i.e., leaflet, annular or RV disease).
Describe the severity of the TR.
Describe the RV function and geometry.
Note that the right ventricular systolic pressure (RVSP) varies by 25% throughout a given day.
Avoid use of the term “trivial” for TR, as it is normal if the valve is structurally normal.
For any given size of tricuspid valve ERO, there is less regurgitant flow than with MR, as the usual RV–RA gradients are less than the usual left ventricular (LV)–left atrial (LA) gradients. Absence of hepatic venous flow reversal is associated with tricuspid valve EROs (<40 mm2) and therefore, in the final analysis, tricuspid valve–ERO generally adds little to hepatic flow profiling.1
Causes of Tricuspid Regurgitation
“Functional” (i.e., intact leaflet/chordal/papillary components)
Myxomatous tricuspid valve disease/tricuspid valve prolapse
RV papillary muscle rupture: post-infarction, post-trauma, post-biopsy, post–lead extraction
Ebstein’s Anomaly
Apical displacement of the septal and or posterior leaflets
“Atrialization” of the right ventricle
“Tethering” of the anterior leaflet
Smaller functional right ventricle
The amount of TR is usually worst at birth as the PVR is highest
Estimation of Right Ventricular Systolic Pressure
Potential problems in estimating the RVSP include the following:
No TR from which to determine RV–RA gradient
Insufficient TR from which to determine maximum RV–RA gradient
Inability to record the full TR profile due to inadequate signal
The correlation of RV:RA gradient is excellent (r = 0.95; SEE = 7 mm Hg)2 (r = 0.96; SEE = 7 mm Hg),3 but the correlation of jugular venous pressure estimate to catheter RAP is less good (r = 0.80; SEE = 2.3 mm Hg). Clearly, clinical estimate of jugular venous pressure overestimates lower RAPs (<8 cm) and underestimates higher RAPs—sometimes by 40% when the true RAP is 20 mm Hg.
More patients with an elevated RVSP have analyzable TR spectral profiles than do patients (half) with normal RVSP.3 However, an important minority subset of patients with severely elevated RVSP (approximately 20–25% of cases of primary pulmonary hypertension) may not have associated TR to yield an analyzable (complete) TR spectral profile. Overall, the correlation of echocardiographic RVSP to catheter RVSP is quite good (r = 0.93; SEE = 8 mm), but remains influenced by the vagaries of estimating jugular venous pressure and RAP.2
Indications for the management and intervention in tricuspid regurgitation are listed in Boxes 7-1 and 7-2.
Tricuspid Stenosis
Scanning Issues
Required parameters to obtain from scanning include the following:
