[level-membership-for-cardiovascular-category]
8 Transposition of the Great Arteries
d-TGA: Preoperative Imaging
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
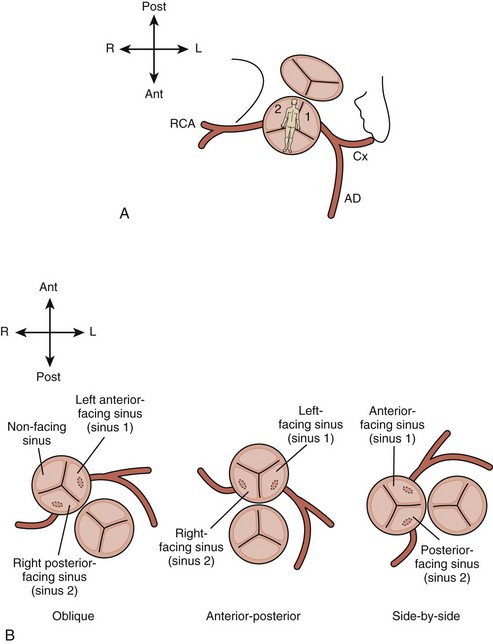
TABLE 8-1 ABBREVIATION CONVENTION USED IN THE LEIDEN CONVENTION FOR DESCRIBING CORONARY ARTERY ANATOMY
| Symbols used are as follows: |
| 1 = sinus 1 |
| 2 = sinus 2 |
| R = right coronary artery |
| L = left anterior descending coronary artery; also designated by some authors AD, as it may not arise from the left. |
| Cx = circumflex coronary artery |
| Comma = major branches originate from a common vessel |
| Semicolon = major branches originate separately |
| Supplemental terms may be used to describe epicardial course and unusual origins. |
| The series of assigned symbols for any given anatomy are enclosed in parentheses. For example: “normal” or “usual” coronary arteries for d-TGA are designated (1L, Cx; 2R), meaning the left anterior descending and circumflex originate from a common vessel from sinus 1, whereas the right coronary artery arises separately from sinus 2. |
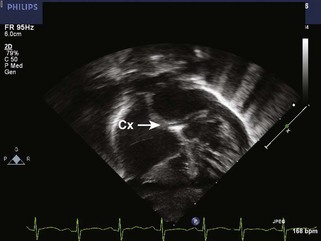
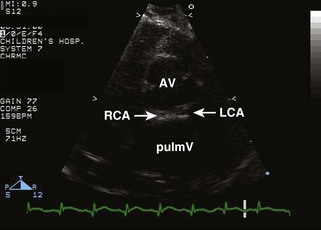
Figure 8-8 As demonstrated in Figure 8-6, when the Cx arises from the RCA (1L; 2R, Cx, or Cx from right coronary artery [RCA]), it reaches the left atrioventricular groove by a retropulmonary course. This may be difficult to see from the parasternal short axis view, but is usually readily evident from the subcostal frontal (shown here) or apical view.
Analysis
Pitfalls
Physiologic Data
Acquisition

Alternate Approaches
Key Points
Transposition of the Great Arteries: Status Post Arterial Switch Operation
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
Analysis
Physiologic Data
Acquisition
Alternate Approaches
Key Points
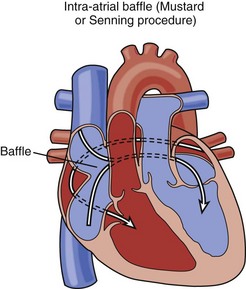
Transposition of the Great Arteries: Status Post Atrial Switch Operation (Senning/Mustard)
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
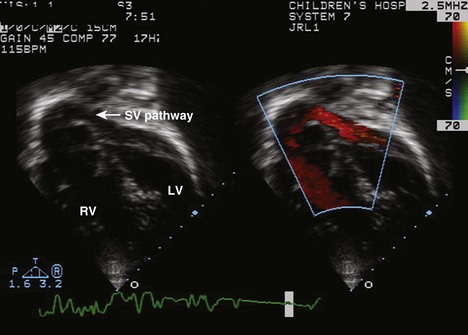
Figure 8-15 Apical view of the systemic venous pathway coursing toward the MV after a Mustard operation.
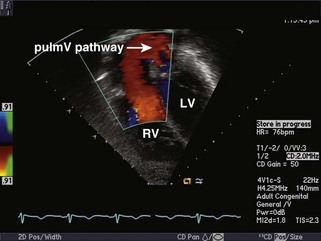
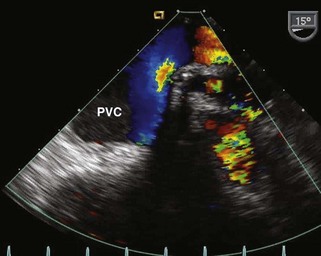
Figure 8-16 Apical view of the pulmonary venous pathway coursing toward the pulmV after a Mustard operation.
Analysis
Physiologic Data
Acquisition
Alternate Approaches
Key Points
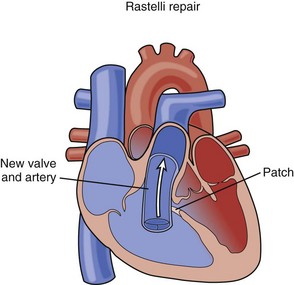
Transposition of the Great Arteries, Ventricular Septal Defect, and Pulmonary Stenosis: Status Post Rastelli or Nikaidoh Procedure
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
Physiologic Data
Acquisition
Alternate Approaches
Key Points
L-TGA (Congenitally Corrected TGA)
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
Physiologic Data
Acquisition
Alternate Approaches
Key Points
1 Earing MG, Ayers NA, Cetta F. Congenitally corrected transposition of the great arteries. In: Eidem BW, Cetta F, O’Leary PW, editors. Echocardiography in Pediatric and Adult Congenital Heart Disease. Philadelphia: Lippincott Williams & Wilkins, 2010.
2 Mahle WT, Marx GR, Anderson RH. Anatomy and echocardiography of discordant atrioventricular connections. Cardiol Young. 2006;16(suppl 3):65-71.
3 Mertens LL, Vogt MO, Marek J, Cohen MS. Transposition of the great arteries. In: Lai WW, Mertens LL, Cohen MS, Geva T, editors. Echocardiography in Pediatric and Congenital Heart Disease. Hoboken, NJ: Wiley-Blackwell, 2009.
4 Miller-Hance WC, Silverman NH. Transesophageal echocardiography in congenital heart disease with focus on the adult. Cardiol Clin. 2000;18(4):861-892.
5 Oechslin E. Physiologically “corrected” transposition of the great arteries. In: Lai WW, Mertens LL, Cohen MS, Geva T, editors. Echocardiography in Pediatric and Congenital Heart Disease. Hoboken, NJ: Wiley-Blackwell, 2009.
6 Pasquini L, Parness IA, Colan SD, et al. Diagnosis of intramural coronary artery in transposition of the great arteries using two-dimensional echocardiography. Circulation. 1993;88:1136-1141.
7 Schultz AH, Lewin MB. D-Transposition of the great arteries. In: Eidem BW, Cetta F, O’Leary PW, editors. Echocardiography in Pediatric and Adult Congenital Heart Disease. Philadelphia: Lippincott Williams & Wilkins, 2010.
[/level-membership-for-cardiovascular-category][not-level-membership-for-cardiovascular-category]
8 Transposition of the Great Arteries
d-TGA: Preoperative Imaging
Background
Overview of Echocardiographic Approach
Anatomic Imaging
Acquisition
TABLE 8-1 ABBREVIATION CONVENTION USED IN THE LEIDEN CONVENTION FOR DESCRIBING CORONARY ARTERY ANATOMY
| Symbols used are as follows: |
| 1 = sinus 1 |
| 2 = sinus 2 |
| R = right coronary artery |
| L = left anterior descending coronary artery; also designated by some authors AD, as it may not arise from the left. |
| Cx = circumflex coronary artery |
| Comma = major branches originate from a common vessel |
| Semicolon = major branches originate separately |
| Supplemental terms may be used to describe epicardial course and unusual origins. |
| The series of assigned symbols for any given anatomy are enclosed in parentheses. For example: “normal” or “usual” coronary arteries for d-TGA are designated (1L, Cx; 2R), meaning the left anterior descending and circumflex originate from a common vessel from sinus 1, whereas the right coronary artery arises separately from sinus 2. |
Figure 8-8 As demonstrated in Figure 8-6, when the Cx arises from the RCA (1L; 2R, Cx, or Cx from right coronary artery [RCA]), it reaches the left atrioventricular groove by a retropulmonary course. This may be difficult to see from the parasternal short axis view, but is usually readily evident from the subcostal frontal (shown here) or apical view.
Analysis
Pitfalls
Physiologic Data
Acquisition
Alternate Approaches
Key Points
[/not-level-membership-for-cardiovascular-category]
