Ovarian/Tubal Torsion
Synonyms/Description
Etiology
Ultrasound Findings
Differential Diagnosis
Clinical Aspects and Recommendations
Figures
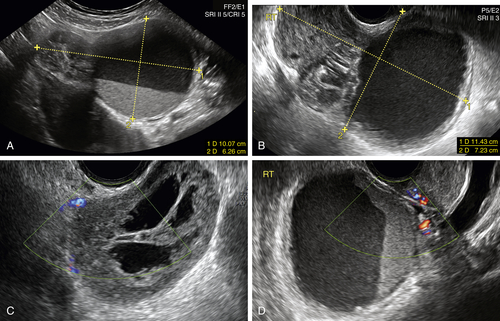
Figure O3-1 Adolescent girl with a 1-month history of pelvic pain. Endometriosis was the diagnosis initially given before referral. A shows a large pelvic mass seen anterior to the uterus on a transabdominal scan (calipers). B to D show various transvaginal views of the mass, which has both cystic and solid components. Note that there is complete absence of blood flow to the ovary. The diagnosis of torsion was made based on these findings, and the patient was taken to surgery.
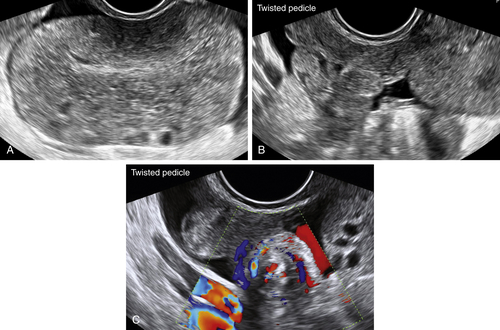
Figure O3-2 Young, reproductive-age woman with a 2-day history of acute pelvic pain. Local diagnosis of ovarian tumor was made. A shows the huge edematous ovary with a few peripheral follicles. B shows the edematous twisted pedicle. C shows color Doppler of the whirlpool sign of the twisted pedicle.
Videos
Suggested Reading
Boukaidi S.A., Delotte J., Steyaert H., Valla J.S., Sattonet C., Bouaziz J., Bongain A. Thirteen cases of isolated tubal torsions associated with hydrosalpinx in children and adolescents, proposal for conservative management: retrospective review and literature survey. J Pediatr Surg. 2011;46:1425–1431.
Huchon C., Fauconnier A. Adnexal torsion: a literature review. Eur J Obstet Gynecol Reprod Biol.. 2010:1508–1512.
Servaes S., Zurakowski D., Laufer M.R., Feins N., Chow J.S. Sonographic findings of ovarian torsion in children. Pediatr Radiol. 2007;37(5):446–451.
Valsky D.V., Esh-Broder E., Cohen S.M., Lipschuetz M., Yagel S. Added value of the gray-scale whirlpool sign in the diagnosis of adnexal torsion. Ultrasound Obstet Gynecol. 2010;36:630–634.
Vijayaraghavan S.B., Senthil S. Isolated torsion of the fallopian tube: the sonographic whirlpool sign. Ultrasound Med. 2009;28:657–662.
Wilkinson C., Sanderson A. Adnexal torsion—a multimodality imaging review. Clin Radiol. 2012;67:476–483.






