50 Tibial Nerve Block
The tibial nerve is the largest branch of the sciatic nerve and the largest nerve for the ankle block. It provides sensory innervation to the heel and to the sole of the foot. The tibial nerve divides into the medial calcaneal, medial plantar, and lateral plantar branches near the ankle.1 In some subjects the takeoff of the medial calcaneal branch from the tibial nerve can be imaged above the ankle joint.
Edema or infection often makes routine ankle block ineffective or contraindicated.2 However, tibial nerve imaging can be difficult in some surgical patients with peripheral vascular disease because vascular landmarks for the nerve are not present. Tibial nerve block in the leg avoids the footdrop that occurs with more proximal popliteal block of the sciatic nerve. This can be an advantage for ambulatory surgery patients.
Suggested Technique
Key Points
| Tibial Nerve Block | The Essentials |
|---|---|
| Anatomy | Two veins usually flank either side of the PTA. |
| The TN is about 4 mm in diameter. | |
| Image orientation | The TN lies on the heel side of the PTA in the leg. |
| Positioning | Externally rotate and support the leg. |
| The heel points toward the operator. | |
| Operator | Standing on the contralateral side of the table |
| Display | Across the table, on the ipsilateral side |
| Transducer | High-frequency linear, 23- to 25-mm footprint |
| Initial depth setting | 25 mm |
| Needle | 25 gauge, 38 mm in length |
| Anatomic location | Begin by scanning the medial aspect of mid-leg. |
| Optimal imaging of TN usually halfway between the gastrocnemius and malleoli. | |
| Approach | SAX view of TN, in-plane from the Achilles side |
| Place the needle tip between the TN and PTA. | |
| Sonographic assessment | Injection should track distally along the TN to MCB (SAX slide). |
| Anatomic variation | Some anatomic variation of the TN position with respect to the PTA. |
Clinical Pearls
• The ideal needle path is between the posterior tibial artery and the tibial nerve, so that the injection separates the two structures.
• Tibial nerve block with ultrasound can be used for outpatient heel surgery to avoid footdrop that occurs with more proximal popliteal block of the sciatic nerve.
• The medial calcaneal branch of the tibial nerve can sometimes be imaged, particularly after tibial nerve block in the leg.
• Be careful with long-axis assessments of local anesthetic distribution along peripheral nerves that lie close to arteries (e.g., the tibial nerve). Partial line-ups on the adjacent artery can appear similar to distributed fluid.
• The central aponeurosis of the tibialis posterior muscle lies deep to the tibial nerve in the leg. These two structures can have similar ultrasound appearance.
• When tibial nerve block is approached from the Achilles tendon side, position the patient with the leg elevated and slightly flexed.

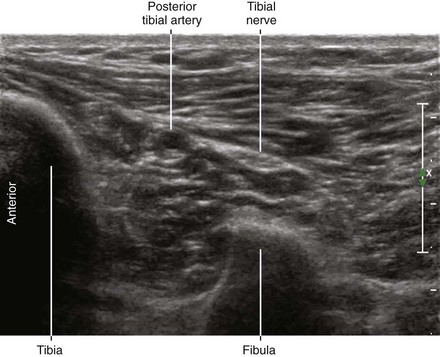
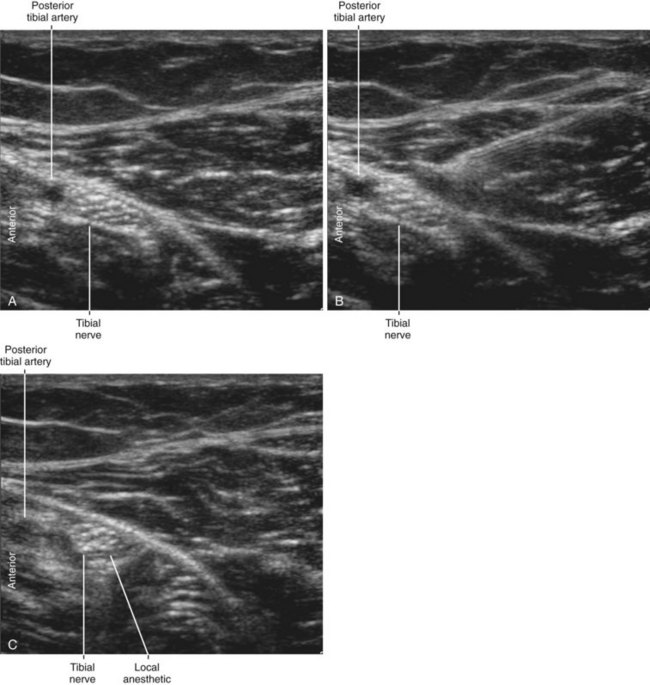
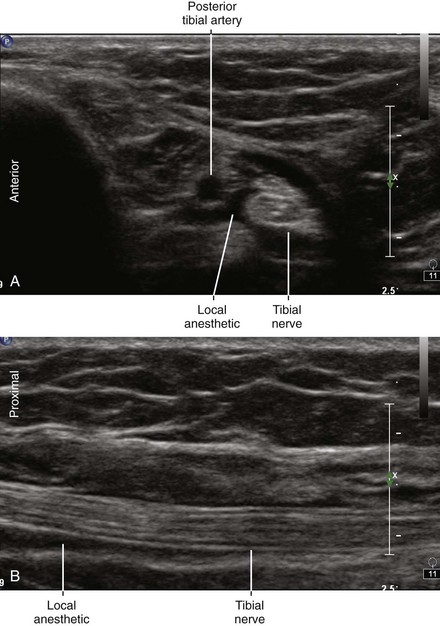
FIGURE 50-4 After injection, local anesthetic is distributed around the tibial nerve (A) and tracks along the nerve (B).
1 Bareither DJ, Genau JM, Massaro JC. Variation in the division of the tibial nerve: application to nerve blocks. J Foot Surg. 1990;29:581–583.
2 Redborg KE, Antonakakis JG, Beach ML, et al. Ultrasound improves the success rate of a tibial nerve block at the ankle. Reg Anesth Pain Med. 2009;34(3):256–260.