Thyroid pathophysiology
Introduction
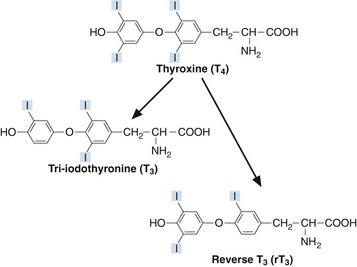
Thyroxine (T4) and tri-iodothyronine (T3) are together known as the ‘thyroid hormones’. They are synthesized in the thyroid gland by iodination and coupling of two tyrosine molecules whilst attached to a complex protein called thyroglobulin. T4 has four iodine atoms while T3 has three (Fig 44.1).
Goitre
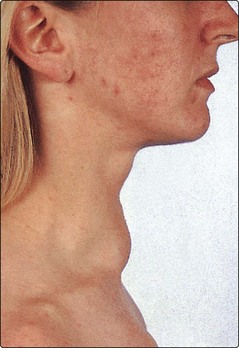
A goitre is an enlarged thyroid gland (Fig 44.2). This may be associated with hypothyroidism, hyperthyroidism or a euthyroid state. Globally, iodine deficiency is the commonest cause of goitre. The WHO estimates that approximately 2 billion people have an inadequate iodine intake making it the commonest preventable cause of neuro-developmental problems. In many developed countries this problem has been overcome by the addition of iodine to a staple food such as iodised salt.


Thyroid function tests
 TSH. Measurement of TSH is a good example of how better technology has helped in the diagnosis and monitoring of disease. Early assays for TSH were unable to measure low concentrations of the hormone – the detection limits of the radioimmunoassays overlapped significantly with concentrations of the low end of the reference interval in healthy subjects. Now, very sensitive TSH assays can detect much lower concentrations and it is possible to tell with a greater degree of certainty whether TSH secretion really is lower than normal.
TSH. Measurement of TSH is a good example of how better technology has helped in the diagnosis and monitoring of disease. Early assays for TSH were unable to measure low concentrations of the hormone – the detection limits of the radioimmunoassays overlapped significantly with concentrations of the low end of the reference interval in healthy subjects. Now, very sensitive TSH assays can detect much lower concentrations and it is possible to tell with a greater degree of certainty whether TSH secretion really is lower than normal.



Drugs and the thyroid
Various drugs affect thyroid function tests. The effects of some of these are summarized in Table 44.1.
Table 44.1
Drugs affecting thyroid function tests
| Drug | Mechanism | Major effects |
| Amiodarone | Reduced peripheral deiodination Amiodarone can also stimulate or inhibit release of thyroid hormones from thyroid |
↑T4,↓T3, transient ↑ in TSH Hyperthyroidism Hypothyroidism |
| Lithium | Reduced thyroid uptake of iodine Reduced release of thyroid hormone |
Goitre Hypothyroidism |
| Anticonvulsants (phenytoin, carbamazepine, phenobarbital) | Displace T4 and T3 from binding proteins | ↑ free T4, ↑ free T3 |
| Heparin | Releases lipoprotein lipase into plasma with resultant increase in free fatty acids. These displace T4 and T3 from binding proteins | ↑ free T4, ↑ free T3 |
| Aspirin | In high concentrations displaces T4 from transthyretin | ↑ free T4 |
 Clinical note
Clinical note
 insulin-dependent diabetes mellitus
insulin-dependent diabetes mellitus


 autoimmune destruction of the adrenal cortex causing Addison’s disease
autoimmune destruction of the adrenal cortex causing Addison’s disease


A combination of these is referred to as Autoimmune Polyglandular Syndrome.





