CHAPTER 3 Thyroglossal Duct Cyst
Step 1: Surgical Anatomy
♦ Thyroglossal duct cyst traditionally manifests as a painless midline anterior cervical mass that often moves with swallowing (Fig. 3-1).
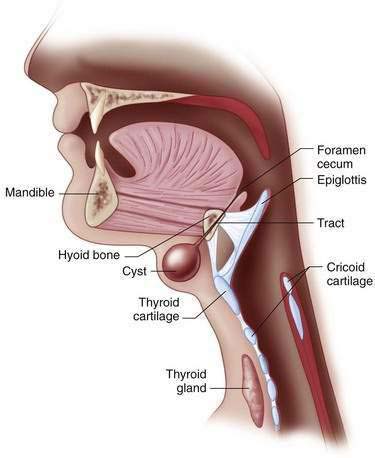
♦ The cyst occasionally communicates with the skin as a draining sinus, and its tract always extends through the center of the hyoid bone to terminate at the tongue base (Fig. 3-2). Operative extirpation of the entire cyst and sinus tract, including the involved portion of the hyoid bone, is critical to avoid a recurrence.
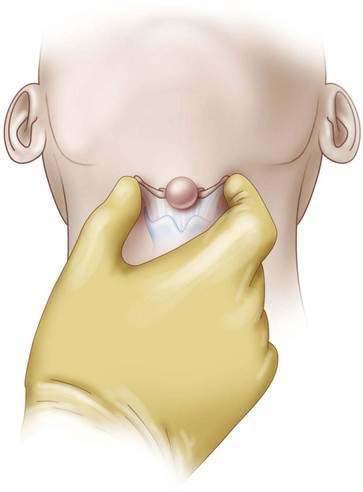
♦ The greater horns of the hyoid bone may be palpated bilaterally and moved side to side, which will result in cyst movement (Fig. 3-3) and help to ensure a proper anatomic resection and avoid injuring the larynx.

Step 2: Preoperative Considerations
♦ The diagnosis of thyroglossal duct cyst is made by a history and physical examination, although an ultrasound may help to differentiate this lesion from a dermoid cyst, epidermoid cyst, or median ectopic thyroid. An extensive radiographic and laboratory evaluation is unnecessary.
♦ Surgical excision is indicated on identification and is easiest in the absence of infection. Most infections can be treated with oral antibiotics targeting Haemophilus influenzae, Staphylococcus aureus, and Staphylococcus epidermidis, but occasionally the abscess is medically refractory and requires drainage. Elective resection is then best reserved for a time when the wound has healed and the inflammation is minimized.
Step 3: Operative Steps
Anesthetic Induction
♦ General endotracheal intubation is preferred for safe airway management. Because of the possibility of digital palpation of the tongue base during the operation (see next comment), the endotracheal tube should be secured in a reliable fashion.
♦ A laryngeal mask airway (LMA) may also be considered, although its use is discouraged. Because the origin of the cyst’s tract must be ligated, the anesthesiologist or an assistant may need to insert a finger into the mouth to reflect the tongue base anteriorly. This maneuver would disrupt the seal on the LMA and hinder ventilation if the patient is not breathing spontaneously.
Positioning
♦ The patient is placed supine with the neck extended. This is facilitated by placing a roll transversely behind the shoulders. The bed is then tilted into the reverse Trendelenburg position (Fig. 3-4).

Incision
♦ The Sistrunk procedure remains the operation of choice for the management of thyroglossal duct cysts.
♦ A transverse incision is made directly over the mass and along a natural skin crease for improved cosmesis. Care should be taken to avoid entering the wall of the cyst.
♦ If previous drainage was required for an infected cyst, the skin may be quite adherent to the cyst. Excising a bit of adherent skin may be helpful.
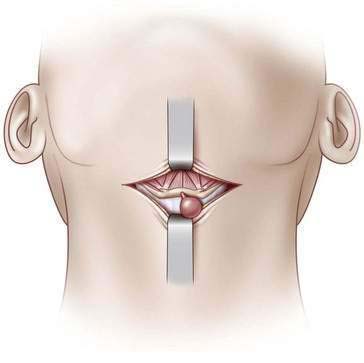
♦ The length of the incision is usually limited to the diameter of the mass, although this length can be increased if additional exposure is required (Fig. 3-5).
♦ Self-retaining retractors are generally not required and, if used, tend to necessitate a larger incision.
♦ The cyst is separated from the surrounding tissue nearly circumferentially, and the sinus tract to the hyoid bone is identified posteriorly and preserved (Fig. 3-6).
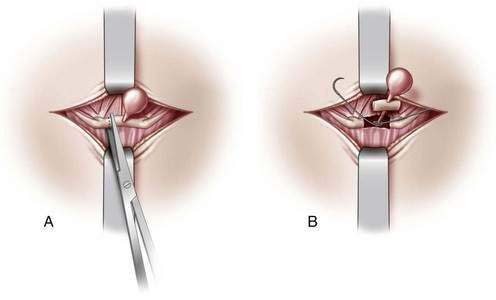
♦ The strap muscles are reflected off the body of the hyoid adjacent to where it is penetrated by the sinus tract. The hyoid is dissected circumferentially on both sides and then divided with scissors or bone cutters just lateral to the penetrating sinus tract (Fig. 3-7, A).
♦ Dissection of the tract is continued proximally and cephalad toward its origin at the foramen cecum, where it is suture ligated (Fig. 3-7, B). This facilitates a complete en bloc resection.

Closing
♦ The platysma muscle is reapproximated using interrupted absorbable sutures. The subcutaneous tissue and skin are then closed by the surgeon’s method of choice. For this I prefer subdermal sutures of 4-0 Vicryl followed by 5-0 Monocryl subcuticular closure. Finally, a dry, sterile occlusive dressing is applied.

Step 5: Pearls and Pitfalls
♦ Despite the low incidence of carcinoma and recurrence, every effort should be made to resect the entire thyroglossal duct cyst and tract to prevent the development of these occurrences.
♦ Recurrent disease is related to incomplete resection and postoperative infection and can be managed by secondary Sistrunk operation with limited base-of-tongue resection, central neck dissection with core resection of the tongue base, or suture-guided transhyoid pharyngotomy.
♦ Although surgeons dislike reporting this, inadvertent resection of a portion of the thyroid cartilage or tracheal ring is a serious complication that must be avoided. Meticulous attention to and identification of anatomic landmarks, particularly the greater horns of the hyoid bone, ensure that this complication is averted.
Kaselas C, Tsikopoulos G, Chortis C, Kaselas B. Thyroglossal duct cyst’s inflammation. When do we operate? Pediatr Surg Int. 2005;1:991-993.
Ostlie DJ, Burjonrappa SC, Snyder CL, et al. Thyroglossal duct infections and surgical outcomes. J Pediatr Surg. 2004;39:396-399.
Perkins JA, Inglis AF, Sie KC, Manning SC. Recurrent thyroglossal duct cysts: a 23-year experience and a new method for management. Ann Otol Rhinol Laryngol. 2006;115:850-856.
Tracy TFJr, Muratore CS. Management of common head and neck masses. Semin Pediatr Surg. 2007;16:3-13.