CHAPTER 7 Thoracoscopic Repair of Esophageal Atresia with Tracheoesophageal Fistula
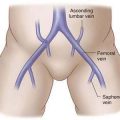
Step 1: Surgical Anatomy
Step 2: Preoperative Considerations
Step 3: Operative Steps
Anesthetic Induction
♦ If the anesthesiologist attempts to place the endotracheal tube past the fistula, care must be taken to avoid a right mainstem intubation, which can cause problems when the right-sided chest is insufflated and the right lung is collapsed.
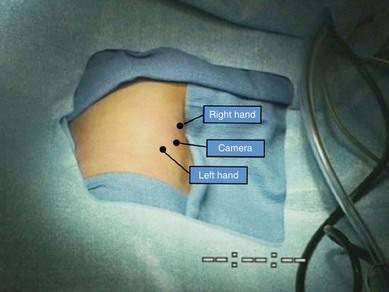
Positioning

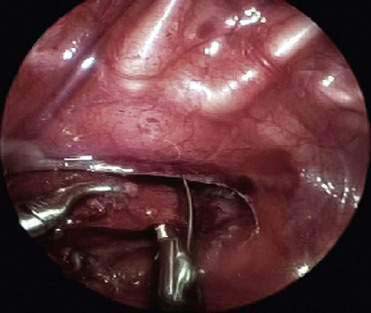
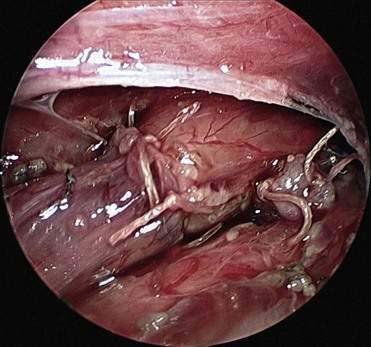
Dividing the Azygos Vein
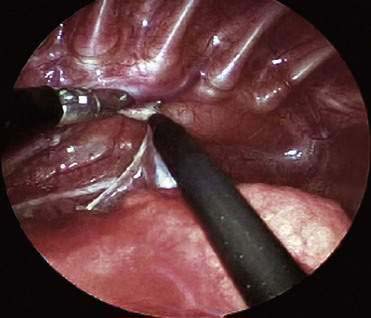
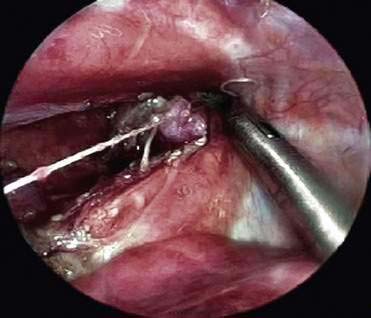
Dividing and Ligating the Fistula (Fig. 7-5)
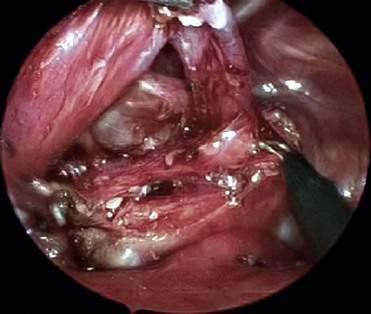
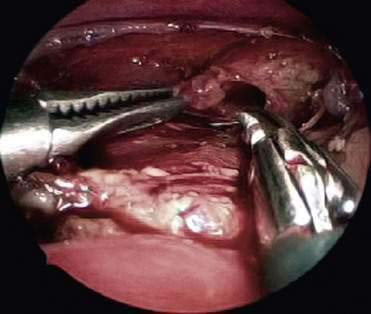
Mobilization of Upper Pouch
♦ The upper pouch is mobilized while anesthesia places gentle pressure on a tube in the pouch. This maneuver is used to determine whether there is adequate length to complete the anastomosis.
♦ An adequate enterotomy is made at the end of the pouch (Fig. 7-7). This often entails removing the tip of the pouch. There is a tendency to make an enterotomy that is too small if no tissue is removed, which may lead to stricture.
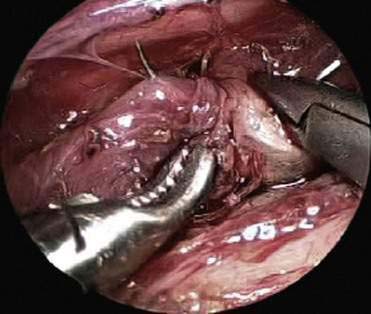
Anastomosis


♦ A small feeding tube is then passed transnasally or transorally by anesthesia through the anastomosis into the stomach (Fig. 7-9).
♦ The anterior (lateral wall) sutures are placed (usually three or four) with the knots tied outside the lumen (Fig. 7-10).




Step 5: Pearls and Pitfalls
Holcomb GW, Rothenberg SS, Bak K, et al. Thoracoscopic repair of esophageal atresia and tracheoesophageal fistula: a multi-institutional analysis. Ann Surg. 2005;242(3):422-428. discussion 428-430
Rothenberg SS. Thoracoscopic repair of esophageal atresia and tracheo-esophageal fistula. Semin Pediatr Surg. 2005;14(1):2-7.
van der Zee D, Bax NMA. Thoracoscopic repair of esophageal atresia with distal fistula. Surg Endosc. 2003;17(7):1065-1067.