[level-membership-for-basic-science-category]
Chapter 9 The reproductive system
Development of the indifferent gonad
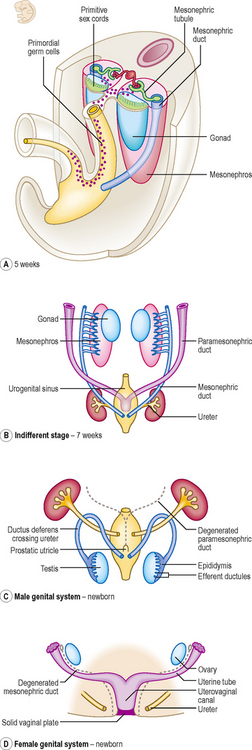
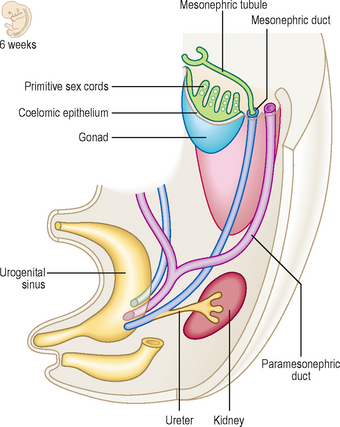
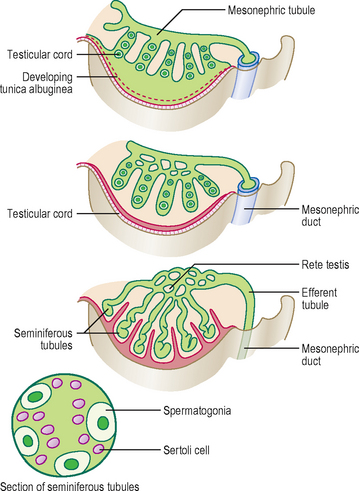
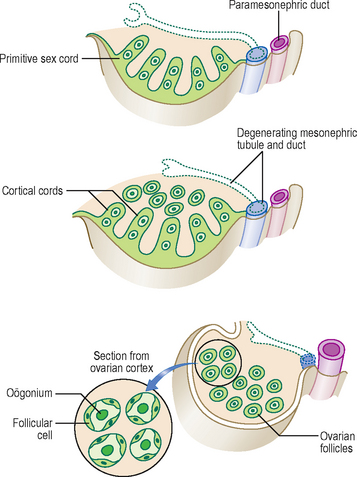
The gonads develop from the intermediate mesoderm that is situated in the paired longitudinal urogenital ridges, the more medial part of these ridges being the gonadal ridges. In the sixth week primordial germ cells migrate from the wall of the yolk sac via the dorsal mesentery of the hindgut to occupy the gonadal ridges. The arrival of these cells induces the cells in the ridges to form primitive sex cords (derived from the mesonephros and overlying coelomic epithelium) (Fig. 9.1A). At this stage the gonad is indifferent or uncommitted (Fig. 9.2), and consists of an outer cortex and an inner medulla. During the next week the male and female gonads begin to differentiate (Fig. 9.1B-D). If germ cells fail to migrate to the gonadal ridges the gonads do not develop.
Genital ducts
Initially, two pairs of genital ducts arise in both male and female: the mesonephric and paramesonephric ducts (Fig. 9.1B–D).
In the male, the mesonephric duct loses its urinary function once the mesonephros is superseded by the metanephros. The mesonephric duct becomes the ductus deferens and the epididymis (the main genital ducts in the male), opening into the urogenital sinus (the anterior part of the cloaca) (Fig. 9.1). The secretion of testosterone by the interstitial Leydig cells from week 8 stimulates the mesonephric ducts to differentiate into their adult derivatives. Each seminal vesicle buds out from the distal mesonephric duct. The prostate arises as a bud from the urethra (Fig. 9.5). The regression of the paramesonephric ducts in the male is stimulated by the anti-mullerian hormone, secreted by the Sertoli cells. The old name for the paramesonephric duct was mullerian duct; the old name for the mesonephric duct was wolffian duct.
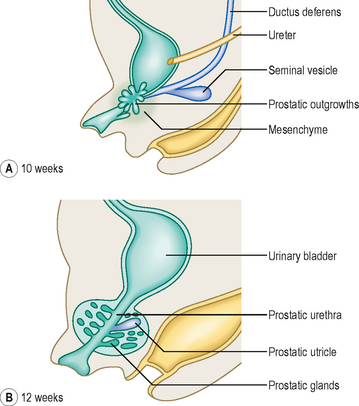
Fig. 9.5 Development of the accessory glands of the male genital system at 10 weeks (A) and 12 weeks (B).
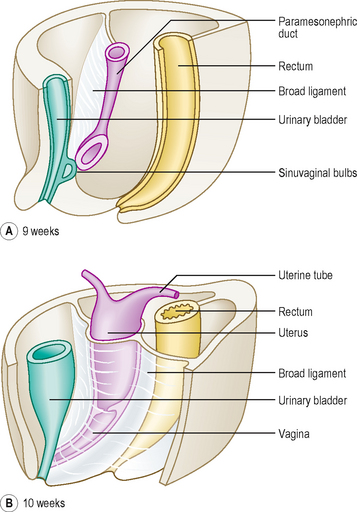
In the female, the mesonephric duct is not involved in genital duct formation. In the absence of anti-mullerian hormone and testosterone the mesonephric ducts regress in the female. The paramesonephric duct system arises as a pair of longitudinal invaginations (Figs 9.1 and 9.2) of the coelomic epithelium that overlies the urogenital ridges. The two ducts lie mainly lateral to the mesonephric ducts, though they cross the mesonephric ducts before entering the urogenital sinus. At their cranial ends the paramesonephric ducts open into the future peritoneal cavity as the future fimbriae of the uterine tubes. The caudal ends of the ducts meet in the midline and fuse to form the uterovaginal canal, from which the uterus and upper part of the vagina arises. The canal fuses with the sinuvaginal bulb, a swelling on the urogenital sinus (Fig. 9.6). As the paramesonephric ducts fuse in the midline they bring together two peritoneal folds, thus forming the right and left broad ligaments. The upper part of the vagina forms from the fused paramesonephric ducts. The lower part of the vagina arises from the urogenital sinus, from the sinuvaginal bulb or later the vaginal plate, initially as a solid tube, later canalizing to form the vaginal lumen (Fig. 9.6).
Descent of the testis and development of the inguinal canal
In both sexes the descent of the gonad to its adult position is by the guidance of the fibrous strand called the gubernaculum. The descent is towards the labioscrotal swellings (that form either the labia majora or the scrotum) (Fig. 9.7). In the female the descent of the gonad is as far as the pelvic cavity, on the posterior aspect of the broad ligament. The part of the gubernaculum remaining between the ovary and the uterus is the ovarian ligament; the part between the uterus and the labia is the round ligament of the uterus. Subsequently in the male, an outpouching of the future peritoneum of the coelomic cavity protrudes into the labioscrotal swellings, into the space created by the gubernaculum. This outpouching is known as the processus vaginalis, and it precedes the future testis into the scrotum (Fig. 9.7). As the processus vaginalis pushes through the three layers of the abdominal wall it forms the inguinal canal, which is actually a series of slits or apertures in the aponeuroses of the inferomedial parts of the anterolateral abdominal wall musculature.
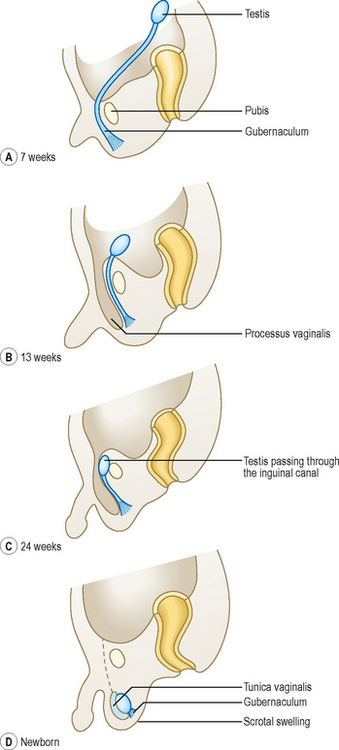
The factors related to the descent of the testis include, firstly, the elongation of the trunk of the fetus, and secondly an increase in intra-abdominal pressure arising because of the increasing size of intra-abdominal organs and the regression of the extra-abdominal part of the gubernaculum. As a consequence of the initial development of the testis high on the future posterior abdominal wall, the testis acquires its blood supply from the abdominal aorta, close to the origin of the renal arteries. Thus, the blood supply also migrates inferiorly, resulting in long, thin testicular arteries which pass through the inguinal canals.
External genitalia
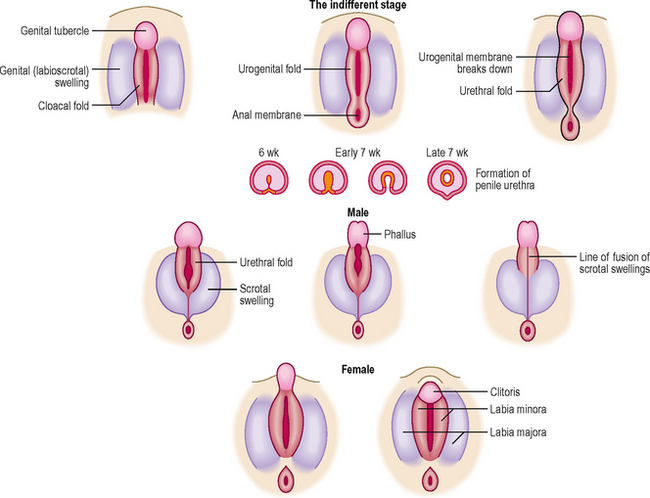
At the earliest stages there is no difference in the form of the external genitalia between the two sexes. At the fifth week a cloacal fold forms on either side of the cloacal membrane and these two folds meet in the midline, anteriorly, as the genital tubercle. Subsequently, and lying lateral to the cloacal folds, the genital swellings form (Fig. 9.8). The latter give rise to the labia majora in the female or to the scrotum in the male. Thus, the genital swellings fuse in the male but not in the female.
 Clinical box
Clinical boxHerniae and undescended testes (cryptorchidism)
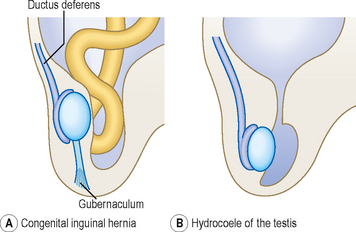
If the processus vaginalis remains in continuity with the peritoneal cavity (normally this connection is lost within the first year of life), then a congenital indirect hernia may develop. If the obliteration of the connection is incomplete with fluid-filled cystic structures remaining these are termed hydrocoeles, and may become inflamed or infected. Such structures may occur anywhere along the length of the spermatic cord, or be related to the testes themselves in the layer known as the tunica vaginalis, which is the persisting part of the original processus vaginalis. The abnormalities of the processus vaginalis are shown in Figure 9.9.
The genital tubercle elongates under hormonal influence to form the penis. The urethral folds are pulled anteriorly to unite by the end of the third month, forming the penile urethra. In females, the genital tubercle forms the clitoris, and the urethral folds remain separate to form the labia minora (Fig. 9.8).
















[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
Chapter 9 The reproductive system
Development of the indifferent gonad
The gonads develop from the intermediate mesoderm that is situated in the paired longitudinal urogenital ridges, the more medial part of these ridges being the gonadal ridges. In the sixth week primordial germ cells migrate from the wall of the yolk sac via the dorsal mesentery of the hindgut to occupy the gonadal ridges. The arrival of these cells induces the cells in the ridges to form primitive sex cords (derived from the mesonephros and overlying coelomic epithelium) (Fig. 9.1A). At this stage the gonad is indifferent or uncommitted (Fig. 9.2), and consists of an outer cortex and an inner medulla. During the next week the male and female gonads begin to differentiate (Fig. 9.1B-D). If germ cells fail to migrate to the gonadal ridges the gonads do not develop.
Genital ducts
Initially, two pairs of genital ducts arise in both male and female: the mesonephric and paramesonephric ducts (Fig. 9.1B–D).
In the male, the mesonephric duct loses its urinary function once the mesonephros is superseded by the metanephros. The mesonephric duct becomes the ductus deferens and the epididymis (the main genital ducts in the male), opening into the urogenital sinus (the anterior part of the cloaca) (Fig. 9.1). The secretion of testosterone by the interstitial Leydig cells from week 8 stimulates the mesonephric ducts to differentiate into their adult derivatives. Each seminal vesicle buds out from the distal mesonephric duct. The prostate arises as a bud from the urethra (Fig. 9.5). The regression of the paramesonephric ducts in the male is stimulated by the anti-mullerian hormone, secreted by the Sertoli cells. The old name for the paramesonephric duct was mullerian duct; the old name for the mesonephric duct was wolffian duct.
Fig. 9.5 Development of the accessory glands of the male genital system at 10 weeks (A) and 12 weeks (B).
In the female, the mesonephric duct is not involved in genital duct formation. In the absence of anti-mullerian hormone and testosterone the mesonephric ducts regress in the female. The paramesonephric duct system arises as a pair of longitudinal invaginations (Figs 9.1 and 9.2
[/not-level-membership-for-basic-science-category]
