[level-membership-for-internal-medicine-category]Chapter 4
The Physical Examination
Don’t touch the patient—state first what you see; cultivate your powers of observation.
Sir William Osler (1849–1919)
The Basic Procedures
In the previous chapters, the general rules for mastering the art of taking the history are discussed. The specific skills necessary to perform a proper physical examination are discussed in this chapter. The four principles of physical examination are as follows:
To achieve competence in these procedures, the student must, in the words of Sir William Osler, “teach the eye to see, the finger to feel, and the ear to hear.” The ability to coordinate all this sensory input is learned with time and practice.
Even though examiners do not use all these techniques for every organ system, they should think of these four skills before moving on to the next area to be evaluated.
Inspection
Inspection can yield an enormous amount of information. Proper technique requires more than just a glance. Examiners must train themselves to look at the body by using a systematic approach. All too often, the novice examiner rushes to use the ophthalmoscope, stethoscope, or otoscope before the naked eyes have been used for inspection.
An example of what is meant by “teaching the eye to see” can be demonstrated in the following exercise. Read the sentence in the box. Then count the number of “f’s” in the sentence.
How many did you count? The answer is given in a footnote at the end of this chapter. This example clearly shows that eyes have to be trained to see.1
While taking the history, the examiner should observe the following aspects of the patient:
The general appearance includes the state of consciousness and personal grooming. Does the patient look well or sick? Is he or she comfortable in bed, or does he or she appear in distress? Is the patient alert, or is he or she groggy? Does he or she look acutely or chronically ill? The answer to this last question is sometimes difficult to determine from inspection, but there are some useful signs to aid the examiner. Poor nutrition, sunken eyes, temporal wasting, and loose skin are associated with chronic disease. Does the patient appear clean? Although the patient is ill, he or she does not have to appear unkempt. Is his or her hair combed? Does he or she bite fingernails? The answers to these questions may provide useful information about the patient’s self-esteem and mental status.
Inspection can evaluate the state of nutrition. Does the patient appear thin and frail? Is the patient obese? Most individuals with chronic disease are not overweight; they are cachectic. Long-standing ailments such as cancer, hyperthyroidism, or heart disease can result in a markedly wasted appearance. See Chapter 29, Assessment of Nutritional Status, available online.
The body habitus is useful to observe, because certain disease states are more common in different body builds. The asthenic, or ectomorphic, patient is thin, has poor muscle development and small bone structure, and appears malnourished. The sthenic, or mesomorphic, patient is the athletic type with excellent development of the muscles and a large bone structure. The hypersthenic, or endomorphic, patient is a short, round individual with good muscle development but frequently has a weight problem.
Because the outward appearance of the body is symmetric, any asymmetry should be noted. Many systemic diseases provide clues that can be uncovered on inspection. For example, an obvious unilateral supraclavicular swelling or a less obvious unilateral miotic pupil is a clue that can aid the examiner in reaching a final diagnosis. A left supraclavicular swelling in a 61-year-old man may represent an enlarged supraclavicular lymph node and could be the only sign of gastric carcinoma. A miotic pupil in a 43-year-old woman may be a manifestation of interruption of the cervical sympathetic chain by a tumor of the apex of the lung. The recent onset of a left-sided varicocele in a 46-year-old man could be related to a left hypernephroma.
The patient is usually in bed when introduced to the examiner. If the patient were walking about, the examiner could use this time to observe the patient’s posture and gait. The ability to walk normally involves coordination of the nervous and musculoskeletal systems. Does the patient drag a foot? Is there a shuffling gait? Does the patient limp? Are the steps normal?
The examiner can learn much about the patient from his or her speech patterns. Is the speech slurred? Does the patient use words appropriately? Is the patient hoarse? Is the voice unusually high or low in pitch? Is the patient moving his or her face normally when speaking? If not, this could provide clues to some cranial nerve problems.
Is the patient oriented to person, place, and time? This can easily be evaluated by asking the patient, “Who are you?” “Where are you?” “What is the date, season, or month?” and “What is the name of the president of the United States?” These questions certainly do not have to be asked at the beginning, but they should be asked at some time during the interview and examination. These questions provide an insight into the mental status of the patient. The mental status examination is discussed further in Chapter 18, The Nervous System.
The examiner must be able to recognize the cardinal signs of inflammation: swelling, heat, redness, pain, and disturbance of function. Swelling results from edema or congestion in local tissues. Heat is the sensation resulting from an increased blood supply to the involved area. Redness is also a manifestation of the increased blood supply. Pain often results from the swelling, which exerts increased pressure on the nerve fibers. Because of the pain and swelling, a disturbance of function may occur.
Palpation
Palpation is the use of touch to determine the characteristics of an area of the body, such as skin elevation or depression, warmth, tenderness, pulses, crepitus, and sizes of organs or masses. For example, an abnormal impulse may be palpated in the right side of the chest and could be related to an ascending aortic aneurysm. A pulsatile mass palpated in the abdomen might be an abdominal aneurysm. An acutely tender mass palpated in the right upper quadrant of the abdomen that descends with inspiration is probably an inflamed gallbladder.
Percussion
Percussion relates to the tactile sensation and sound produced when a sharp blow is struck to an area being examined. One finger delivers a sharp tap to another finger of the other hand. This provides valuable information about the structure of the underlying organ or tissue. A difference from normal sensation may be related to fluid in an area that normally does not contain fluid. Collapse of a lung changes the percussion note, as does a solid mass in the abdomen. Percussion that produces a dull note in the midline of the lower abdomen in a man probably represents a distended urinary bladder.
Auscultation
Auscultation involves listening to sounds produced by internal organs. This technique furnishes information about an organ’s disease process. The examiner is urged to learn as much as possible from the other techniques before using the stethoscope. This instrument should corroborate the signs that were suggested by the other techniques. To examine the heart, chest, and abdomen, auscultation should be used, not alone, but together with inspection, percussion, and palpation. Listening for carotid, ophthalmic, or renal bruits can provide lifesaving information. The absence of normal bowel sounds could indicate a surgical emergency.
Preparation for the Examination
The physical examination usually begins after the history has been documented. You should have a portable case designed to contain all the necessary equipment, which includes the items listed in Table 4-1.
Table 4–1
Equipment for Physical Examination
| Required | Optional | Available in Most Patient Care Areas |
| Stethoscope | Nasal illuminator† | Sphygmomanometer |
| Otoscope and ophthalmoscope | Nasal speculum | Tongue blades |
| Penlight | Tuning fork: 512 Hz | Applicator sticks |
| Reflex hammer | Gauze pads | |
| Tuning fork: 128 Hz | Gloves | |
| Safety pins* | Lubricant gel | |
| Tape measure | Guaiac card for occult blood | |
| Pocket visual acuity card | Vaginal speculum |
* A new pin should be used for each patient as a precaution against transmission of the human immunodeficiency and hepatitis viruses. As an alternative, a broken wooden applicator stick may be used.
† Attachment for the otoscope handle.
Place the equipment on the patient’s night table or bed stand. By laying out all the tools, you are less likely to forget to perform a specific examination. Adjust the lighting; good lighting is important for good inspection! It is preferable to use daylight for illumination, if possible, because skin color changes may be masked by artificial light. The patient’s curtains should be closed for privacy at the start of the interview. Finally adjust the bed to a convenient height. If you have elevated the bed, make sure to lower it after completion of the examination.
Before examining the patient, wash your hands, preferably while the patient is watching. Washing with soap and water is an effective way to reduce the transmission of disease. Be sure to lather for 10 seconds or more. If soap and water is not available, it is also acceptable to use an alcohol-based hand hygiene product unless there is visible soiling.
The patient should be wearing a gown that opens at the front or back. Pajamas are also acceptable. It is most important to consider the comfort of the patient. You should allow the patient the use of pillows if requested. This is one of the few relationships in which individuals are willing to expose themselves to a stranger after only brief contact.
It is important that you become skilled in each organ system examination. Incorporate the individual evaluations into the complete examination with the least amount of movement of the patient. Avoid unnecessary changes, if possible. Regardless of age, patients tire quickly when asked to “sit up,” “lie down,” “turn on your left side,” “sit up,” “lie down,” and so on. You should perform as much of the examination as possible with the patient in one position. It is also important that the patient never be asked to sit up in bed without support for any extended period. Although you are learning physical examination by systems, the physical examination is conducted by body regions, not by systems. When examining the head, for example, you will evaluate the skin, hair, eyes, nose, ears, throat, sinuses, and cranial nerves, even though these involve many “systems.”
By convention, the examiner stands to the right of the patient as the patient lies in bed. The examiner uses the right hand for most maneuvers of the examination. It is common practice that even left-handed individuals learn to perform the examination from the right side, using the right hand. Each of the subsequent chapters on organ systems discusses the placement of hands.
Although it is necessary for the patient to disrobe completely, the examination should be carried out by exposing only the areas that are being examined at that time, without undue exposure of other areas. When a woman’s breast is examined, for example, it is necessary to check for any asymmetry by inspecting both breasts at the same time. After inspection has been completed, you may use the patient’s gown to cover the breast not being examined. The examination of the abdomen may be done discreetly by placing a towel or the bed sheet over the genitalia. Examination of the heart with the patient in the supine position may be performed with the right breast covered. Respecting the patient’s privacy goes a long way in establishing a good doctor-patient relationship.
While performing the physical examination, you should continue speaking to the patient. You may wish to pursue various parts of the history, as well as tell the patient what is being done. You should refrain from comments such as “That’s good” or “That’s normal” or “That’s fine” in reference to any part of the examination. Although this is initially reassuring to the patient, if you fail to make such a statement during another part of the examination, the patient will automatically assume that there is something wrong or abnormal.
The following chapters discuss the individual organ system examinations. Chapter 19, Putting the Examination Together, then summarizes a method of combining all the individual evaluations into one smooth, continuous examination.
Health Care Infection Control Practices2
Any member of the health care delivery team who has exposure to patients has the potential for exposure to infections. It is important that the clinician be aware of the possible infections that may be transmitted and also how certain organisms can be transmitted from patient to patient. Infection control practices are aimed at prompt identification of individuals who harbor or are infected with transmissible agents; appropriate guidelines must be followed to protect both the patient and the clinician.
Several precautionary guidelines have been established by both the Centers for Disease Control and Prevention and the Occupational Safety and Health Administration. These guidelines should be followed routinely by all health care workers whenever exposure to potentially infectious materials such as blood or other body fluids is possible.
Universal precautions are infection control methods that treat all human blood and certain body fluids as if they are known to be infected with human immunodeficiency virus (HIV), hepatitis B virus, hepatitis C virus (HCV), and other blood-borne pathogens. Universal precautions recommend the use of gloves, masks, and gowns if blood or other potentially infectious materials are being handled. This applies to individuals in contact with the body fluids and especially any individuals performing procedures.
Other ways to reduce potential exposure to blood-borne pathogens include the use of protective eyewear as needed, the use of gloves with any exudative cutaneous lesions, and proper disposal of sharps.
Standard precautions are recommended for the care of all patients regardless of their disease status. These include handwashing and using the appropriate protective equipment as needed for handling body fluids.
Transmission-based precautions are additional guidelines recommended to decrease the transmission of pathogens throughout the hospital. There are several categories:
There are also circumstances in which more than one type of precaution is recommended. The appropriate signage should be indicated on the door of the patient’s room and all appropriate guidelines should be followed.
Needlestick injuries can occur in accidental situations. When a needlestick injury occurs, the individual should promptly flush the affected area with water vigorously and seek guidance from the hospital’s needlestick coordinator. Every hospital has a protocol in place and an individual should be available at any time of day to answer questions. If appropriate, postexposure prophylaxis for HIV is available and should be administered as soon as possible. Hepatitis B serologic testing should also be considered as immunoglobulin can be considered in rare situations. Hepatitis C can likewise be spread via needlestick; however, there are no available vaccinations or guidelines for postexposure prophylaxis for HCV exposure.
All health care providers who have direct contact with patients should complete the hepatitis B vaccine series. In certain populations, testing for immunity before vaccination may be indicated. Typical pre-employment and student health service screening includes a purified protein derivative test for tuberculosis and various serologic testing, including testing for hepatitis B.
It is also the responsibility of all health care workers not to transmit disease to their patients. Workers who have a lesion on their hands should wear gloves; if they have a cold, they should cover their nose and mouth; if they are sick, they should consider deferring patient contact.
Goal of the Physical Examination
The goal of the physical examination is to obtain valid information concerning the health of the patient. The examiner must be able to identify, analyze, and synthesize the accumulated information into a comprehensive assessment.
The validity of a physical finding depends on many factors. Clinical experience and reliability of the examination techniques are most important. False-positive or false-negative results reduce the precision of the techniques. Variance can occur when techniques are performed by different examiners with different equipment on different patients. The concepts of validity and precision are discussed further in Chapter 24, Diagnostic Reasoning in Physical Diagnosis.
Unconscious bias is an important concept to understand. It is well known that unconscious bias in an examiner can influence the evaluation of a physical finding. For example, in patients with rapid atrial fibrillation, the ventricular rate is irregular and varies from 150 to 200 beats per minute. The radial pulse rate is significantly lower, owing to a pulse deficit (explained in Chapter 11, The Heart). If examiners record the apical heart rate first, they find that the rate varies from 150 to 200 beats per minute. If they then check the radial pulse, they detect a faster pulse rate than if they had measured the radial pulse first. The first observation, therefore, biases the second observation. Alternatively, if examiners determine the radial pulse first and the heart rate second, the apical heart rate appears slower, but the chance of bias is lower because observer error is less at the apex (Chalmers, 1981).
It is important to review the concepts of sensitivity and specificity. Sensitivity is the frequency of a positive result of a test or technique in individuals with a disease or condition. Specificity is the frequency of a negative result of a test or technique in individuals without a disease or condition. Sensitivity and specificity refer to properties of the test or technique, whereas the health care provider is interested in properties or characteristics of the patient, which are characterized by the predictive values. The positive predictive value is the frequency of disease in patients with positive test results. The negative predictive value is the frequency of lack of disease in patients with negative test results. The question, “What is the possibility that a woman with a stony-hard breast mass has cancer?” addresses the positive predictive value. Predictive value depends on the prevalence of disease in the respective population, as well as the sensitivity and specificity of the test. In an individual from a population with a low prevalence of disease, a positive test result still yields a low positive predictive value.
For example, eliciting the presence of shifting dullness is a highly sensitive technique for detecting ascites. Thus an examiner who does not detect shifting dullness in a patient’s abdomen can be reasonably sure that this negative finding rules out ascites. In contrast, the finding of microaneurysms in the macular area of the retina is a highly specific finding for diabetes. Thus an examiner who finds microaneurysms at the macula can be reasonably confident that this finding confirms diabetes because normal individuals without diabetes do not have macular microaneurysms; that is, the finding of microaneurysms at the macula has a high degree of specificity. Unfortunately, a technique is rarely both very sensitive and very specific. Several techniques must be applied together to make an appropriate assessment.
In summary:
These concepts are discussed in more detail in Chapter 24, Diagnostic Reasoning in Physical Diagnosis.
There are six “f’s” in the sentence in the box. Go back and count them. Most individuals count only three, neglecting to include the “f’s” in the three instances of “of.”
The bibliography for this chapter is available at studentconsult.com.
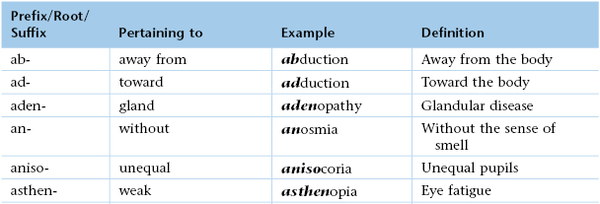
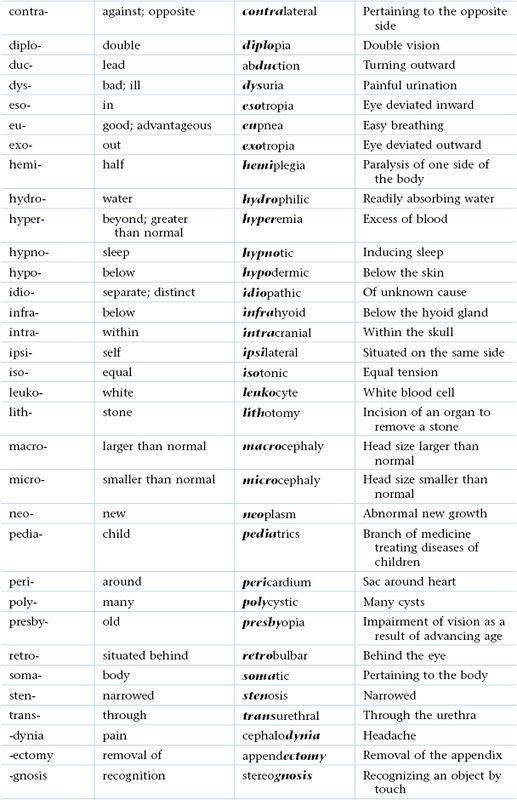
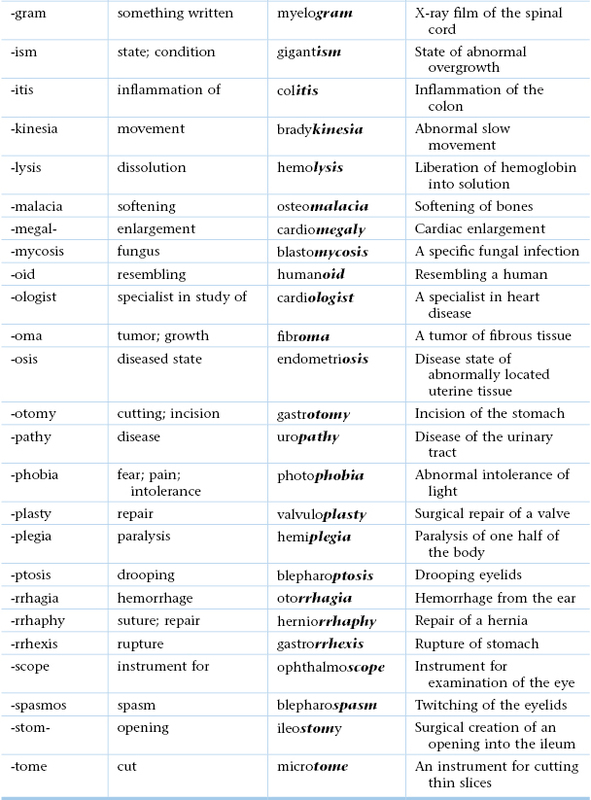
Useful Vocabulary
The vocabulary of medicine is difficult and broad. Memorizing a term is less useful than being able to determine the meaning by understanding its etymology, or roots. When etymology is understood, the spelling of terms will also be easier.
This box lists some general prefixes, roots, and suffixes that are important to understand. At the end of each chapter in Section 2 is a list of terminology for that area of the body. The following list should not be memorized at this time. It should be referred to in conjunction with the lists in subsequent chapters.
Bibliography
Advisory Committee on Immunization Practices. Recommended immunization schedule: United States, October 2007–September 2008. Ann Intern Med. 2007;147:725.
Centers for Disease Control and Protection. Recommended immunizations for adults—United States, 2011. MMWR Morb Mortal Wkly Rep. 2011;60(04):1 http://www.cdc.gov/vaccines/schedules/downloads/adult/adult-schedule-easy-read.pdf.
Centers for Disease Control and Protection. Standard precautions: guidelines for isolation precautions: preventing transmission of infectious agent in healthcare settings 2007. [Updates October 2007. Available at] http://www.cdc.gov/hicpac/pdf/isolation/Isolation2007.pdf [Accessed January 27, 2013] .
Centers for Disease Control and Protection. Standard precautions: guide to infection prevention in outpatient settings. Minimum expectations for safe care. [May 2011. Available at] http://www.cdc.gov/HAI/pdfs/guidelines/ambulatory-care-checklist-07-2011.pdf [Accessed August 1, 2013] .
Chalmers TC. The clinical trial. Milbank Mem Fund Q. 1981;59:324.
Koh HK. A 2020 vision for healthy people. N Engl J Med. 2010;362:1653.
Panlilio AL, et al. Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and recommendations for postexposure prophylaxis. MMWR Morb Mort Wkly Rep. 2005;54(RR-9):1.
Siegel JD, et al. guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. [June 2007. Available at] http://www.cdc.gov/ncidod/dhqp/pdf/isolation2007.pdf; 2007 [Accessed January 27, 2013] .
U.S. Preventative Services Task Force. Guide to clinical preventative services 2012. Recommendations of the U.S. Preventative Services Task Force. [October 2001. Available at] http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/guide/index.html [Accessed August 1, 2013] .
1 This test has been circulated widely in the medical community. The original writer is unknown.
2 This section was written in collaboration with Talia H. Swartz, MD, PhD, Instructor in the Division of Infectious Diseases, Department of Medicine at the Mount Sinai Medical Center, New York.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]Chapter 4
The Physical Examination
Don’t touch the patient—state first what you see; cultivate your powers of observation.
Sir William Osler (1849–1919)
The Basic Procedures
In the previous chapters, the general rules for mastering the art of taking the history are discussed. The specific skills necessary to perform a proper physical examination are discussed in this chapter. The four principles of physical examination are as follows:
To achieve competence in these procedures, the student must, in the words of Sir William Osler, “teach the eye to see, the finger to feel, and the ear to hear.” The ability to coordinate all this sensory input is learned with time and practice.
Even though examiners do not use all these techniques for every organ system, they should think of these four skills before moving on to the next area to be evaluated.
Inspection
Inspection can yield an enormous amount of information. Proper technique requires more than just a glance. Examiners must train themselves to look at the body by using a systematic approach. All too often, the novice examiner rushes to use the ophthalmoscope, stethoscope, or otoscope before the naked eyes have been used for inspection.
An example of what is meant by “teaching the eye to see” can be demonstrated in the following exercise. Read the sentence in the box. Then count the number of “f’s” in the sentence.
How many did you count? The answer is given in a footnote at the end of this chapter. This example clearly shows that eyes have to be trained to see.1
While taking the history, the examiner should observe the following aspects of the patient:
The general appearance includes the state of consciousness and personal grooming. Does the patient look well or sick? Is he or she comfortable in bed, or does he or she appear in distress? Is the patient alert, or is he or she groggy? Does he or she look acutely or chronically ill? The answer to this last question is sometimes difficult to determine from inspection, but there are some useful signs to aid the examiner. Poor nutrition, sunken eyes, temporal wasting, and loose skin are associated with chronic disease. Does the patient appear clean? Although the patient is ill, he or she does not have to appear unkempt. Is his or her hair combed? Does he or she bite fingernails? The answers to these questions may provide useful information about the patient’s self-esteem and mental status.
Inspection can evaluate the state of nutrition. Does the patient appear thin and frail? Is the patient obese? Most individuals with chronic disease are not overweight; they are cachectic. Long-standing ailments such as cancer, hyperthyroidism, or heart disease can result in a markedly wasted appearance. See Chapter 29, Assessment of Nutritional Status, available online.
The body habitus is useful to observe, because certain disease states are more common in different body builds. The asthenic, or ectomorphic, patient is thin, has poor muscle development and small bone structure, and appears malnourished. The sthenic, or mesomorphic, patient is the athletic type with excellent development of the muscles and a large bone structure. The hypersthenic, or endomorphic, patient is a short, round individual with good muscle development but frequently has a weight problem.
Because the outward appearance of the body is symmetric, any asymmetry should be noted. Many systemic diseases provide clues that can be uncovered on inspection. For example, an obvious unilateral supraclavicular swelling or a less obvious unilateral miotic pupil is a clue that can aid the examiner in reaching a final diagnosis. A left supraclavicular swelling in a 61-year-old man may represent an enlarged supraclavicular lymph node and could be the only sign of gastric carcinoma. A miotic pupil in a 43-year-old woman may be a manifestation of interruption of the cervical sympathetic chain by a tumor of the apex of the lung. The recent onset of a left-sided varicocele in a 46-year-old man could be related to a left hypernephroma.
The patient is usually in bed when introduced to the examiner. If the patient were walking about, the examiner could use this time to observe the patient’s posture and gait. The ability to walk normally involves coordination of the nervous and musculoskeletal systems. Does the patient drag a foot? Is there a shuffling gait? Does the patient limp? Are the steps normal?
The examiner can learn much about the patient from his or her speech patterns. Is the speech slurred? Does the patient use words appropriately? Is the patient hoarse? Is the voice unusually high or low in pitch? Is the patient moving his or her face normally when speaking? If not, this could provide clues to some cranial nerve problems.
Is the patient oriented to person, place, and time? This can easily be evaluated by asking the patient, “Who are you?” “Where are you?” “What is the date, season, or month?” and “What is the name of the president of the United States?” These questions certainly do not have to be asked at the beginning, but they should be asked at some time during the interview and examination. These questions provide an insight into the mental status of the patient. The mental status examination is discussed further in Chapter 18, The Nervous System.
The examiner must be able to recognize the cardinal signs of inflammation: swelling, heat, redness, pain, and disturbance of function. Swelling results from edema or congestion in local tissues. Heat is the sensation resulting from an increased blood supply to the involved area. Redness is also a manifestation of the increased blood supply. Pain often results from the swelling, which exerts increased pressure on the nerve fibers. Because of the pain and swelling, a disturbance of function may occur.
Palpation
Palpation is the use of touch to determine the characteristics of an area of the body, such as skin elevation or depression, warmth, tenderness, pulses, crepitus, and sizes of organs or masses. For example, an abnormal impulse may be palpated in the right side of the chest and could be related to an ascending aortic aneurysm. A pulsatile mass palpated in the abdomen might be an abdominal aneurysm. An acutely tender mass palpated in the right upper quadrant of the abdomen that descends with inspiration is probably an inflamed gallbladder.
Percussion
Percussion relates to the tactile sensation and sound produced when a sharp blow is struck to an area being examined. One finger delivers a sharp tap to another finger of the other hand. This provides valuable information about the structure of the underlying organ or tissue. A difference from normal sensation may be related to fluid in an area that normally does not contain fluid. Collapse of a lung changes the percussion note, as does a solid mass in the abdomen. Percussion that produces a dull note in the midline of the lower abdomen in a man probably represents a distended urinary bladder.
Auscultation
Auscultation involves listening to sounds produced by internal organs. This technique furnishes information about an organ’s disease process. The examiner is urged to learn as much as possible from the other techniques before using the stethoscope. This instrument should corroborate the signs that were suggested by the other techniques. To examine the heart, chest, and abdomen, auscultation should be used, not alone, but together with inspection, percussion, and palpation. Listening for carotid, ophthalmic, or renal bruits can provide lifesaving information. The absence of normal bowel sounds could indicate a surgical emergency.
Preparation for the Examination
[/not-level-membership-for-internal-medicine-category]
