[level-membership-for-internal-medicine-category]Chapter 18
The Nervous System
As the debility increases and the influence of the will over the muscles fades, the tremulous agitation becomes more vehement. It now seldom leaves him for a moment; but even when exhausted nature seizes a small portion of sleep, the motion becomes so violent as not only to shake the bed-hangings, but even the floor and sashes of the room. The chin is now almost immovably bent down upon the sternum. The slops with which he is attempted to be fed, with the saliva, are continually trickling from the mouth. The power of articulation is lost. The urine and faeces are passed involuntarily; and at the last, constant sleepiness, with slight delirium, and other marks of extreme exhaustion, announce the wished-for release.
James Parkinson (1755–1824)
General Considerations
By the second century CE, Galen had already described the cerebral ventricles, 7 of the 12 cranial nerves, and the cerebral convolutions. There was, however, little further interest in the anatomy and physiologic characteristics of the neurologic system until the sixteenth century. In 1543, Andreas Vesalius illustrated the basal ganglia, and in 1552, Bartolommeo Eustachius described the cerebellar peduncles and the pons.
In the seventeenth century, Thomas Willis published descriptions and illustrations of the cerebral circulation, the “striate body,” and the internal capsule. Caspar Bartholin and others thought that the function of the cerebral cortex was to protect the blood vessels, whereas other investigators believed that the cerebrum possessed higher functions. François Pourfour du Petit stressed that the cortex was responsible for motor activity. This concept lay dormant until the end of the nineteenth century.
Careful anatomic descriptions of the tracts, nuclei, and gyri were contained in the writings of scientists of the eighteenth and early nineteenth centuries. Johann Christian Reil and Karl Friedrich Burdach provided names for the many gross anatomic structures that had been illustrated by others in previous centuries. Reil has been credited with the naming of the insula, capsule, uncinate and cingulate fasciculi, and tapetum. The uncus, lenticular nucleus, pulvinar, and gyrus cinguli were named by Burdach. During this same period, Samuel von Soemmering, Felix Vicq d’Azyr, Franz Josef Gall, Louis Gratiolet, and Luigi Rolando made many detailed illustrations of the cerebral convolutional patterns.
The next instance was in a man wounded by the horn of an ox. The point entered under the angle of the jaw and came out before the ear. … He remains now a singular proof of the effects of the loss of function in the muscles of the face by this nerve being divided. The forehead of the corresponding side is without motion, the eyelids remain open, the nostril has no motion in breathing, and the mouth is drawn to the opposite side.
This is the classic description of facial nerve (seventh cranial nerve) palsy, also known as Bell’s palsy.
In the mid-nineteenth century, an interest in microscopic neuroanatomy developed. Jan Purkinje, Theodor Schwann, and Hermann von Helmholtz were a few of the many neuroanatomists who contributed valuable information about the intricacies of the nervous system. However, not until the late nineteenth century were specific staining techniques developed by Camillo Golgi, Vittorio Marchi, and Franz Nissl, which led to the current understanding of neuronal disease. The nerve cell had finally been discovered.
The twentieth century was a period of further progress in the description of the cerebral cortex, anterior commissure, thalamus, and hypothalamus. A major advance came from the work of Santiago Ramón y Cajal in 1904. His histologic exploration clarified the complexities of the neuron. Not until 1925 were the hypophysial-hypothalamic connections described, and even today, the function of the hypothalamus is not fully understood.
It has been suggested that more than 40% of patients who present to internists have symptoms referable to neurologic disease. The internist must be able to identify the early signs and symptoms of neurologic disease and initiate the appropriate therapy. All too often, subtle signs and symptoms may be ignored, and a diagnosis is not made until advanced disability is apparent.
Cerebrovascular disease is one of the most devastating diseases of our time. It remains the third leading cause of death in the United States. More than 700,000 Americans suffer a stroke yearly, and it is the number one cause of disability; more than 3 million Americans currently live with permanent brain damage caused by such an event. On average, someone in the United States suffers a stroke every 53 seconds, and every 3.3 minutes, someone dies of one. In 2011, there were 2,513,171 deaths from cardiovascular disease, including 128,931 deaths related to cerebrovascular disease. The number of noninstitutionalized adults who have ever had a stroke is 6.2 million people. The debilitating consequences of stroke and the economic effect on society are enormous.
The generalist or internist holds an important position because a patient with a neurologic problem usually seeks help from that physician first. A thorough knowledge of basic neuroanatomy and physiology is the cornerstone of neurologic diagnosis.
Structure and Physiologic Characteristics
The brain, which is enclosed in the cranium and surrounded by the meninges, is the center of the nervous system. The brain can be divided into paired cerebral hemispheres, basal ganglia, diencephalon (thalamus and hypothalamus), brain stem, and cerebellum.
The two cerebral hemispheres make up the largest portion of the brain. Each hemisphere can be subdivided into four major lobes named for the cranial bones that overlie them: frontal, parietal, occipital, and temporal. The fissures and sulci divide the cerebral surface. A deep midline, longitudinal fissure separates the two hemispheres. The convolutions, or gyri, lie between the sulci. A lateral view of the left cerebral hemisphere is pictured in Figure 18-1. Figure 18-2 is a medial view of the right cerebral hemisphere. A basal view of the cerebral hemispheres is pictured in Figure 18-3.
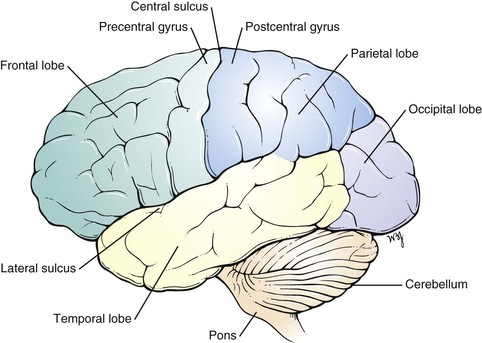
Figure 18–1 Lateral view of the left cerebral hemisphere.
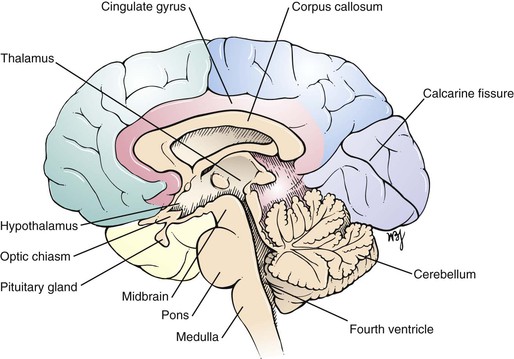
Figure 18–2 Medial view of the right cerebral hemisphere.
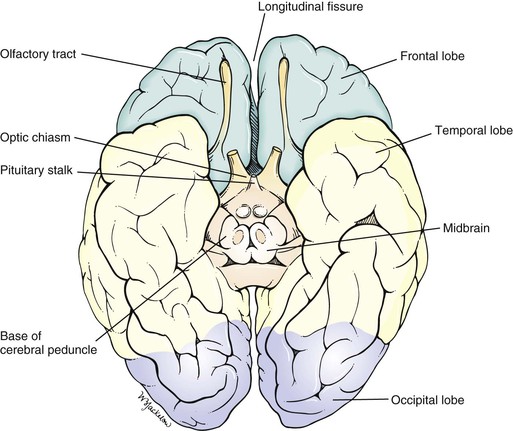
Figure 18–3 Basal view of the cerebral hemispheres.
The cerebrum is responsible for motor, sensory, associative, and higher mental functions. The primary motor cortex is located in the precentral gyrus. Neurons in this area control voluntary movements of the skeletal muscles on the opposite side of the body. An irritative lesion in this area may cause seizures or changes in consciousness. Destructive lesions in this area can produce contralateral flaccid paresis or paralysis.
The primary visual cortex is located in the occipital lobe along the calcarine fissure, which divides the cuneus from the lingual gyri. Irritative lesions in this area produce visual symptoms such as flashes of light or rainbows. Destructive lesions cause homonymous hemianopsia on the contralateral side. Central macular vision is spared.
The primary auditory cortex is located in the temporal lobe along the transverse temporal gyrus. Irritative lesions in this area produce a buzzing or ringing in the ears. Destructive lesions almost never produce deafness.
The basal ganglia are situated deep within the cerebral hemispheres. The structures constituting the basal ganglia include the caudate and lenticular nuclei, as well as the amygdala. The amygdala is part of the limbic system and is concerned with emotion. All other components are important structures in the extrapyramidal system, which is concerned with modulating voluntary body movements, postural changes, and autonomic integration. The basal ganglia are especially involved with fine movements of the extremities. Disturbances of the basal ganglia can result in tremors and rigid movements.
The thalamus is a large nuclear mass located on each side of the third ventricle. The thalamus is the chief sensory and motor integrating mechanism of the neuraxis. All sensory impulses, except olfactory ones, and the major output from systems that modulate and modify motor function (i.e., the cerebellum and corpus striatum) terminate in the thalamus, from which they are projected to specific areas of the cerebral cortex. The thalamus is involved in certain emotional connotations that accompany most sensory experiences. Through its connections with the hypothalamus and striatum, the thalamus can influence visceral and somatic effectors serving primarily affective reactions. Through its control of the electrical excitability of the cerebral cortex, the thalamus plays a dominant role in the maintenance and regulation of the state of consciousness, alertness, and attention. The thalamus may be the critical structure for pain perception and thermal sense, which remain after complete destruction of the primary sensory cortex. Thermal sense endows sensation with discriminative faculties and is not concerned with the recognition of crude sensory modalities.
The hypothalamus is located below the thalamus. It includes the optic chiasm and the neurohypophysis. The hypothalamus is responsible for many regulatory mechanisms, such as temperature regulation; neuroendocrine control of catecholamines, thyroid-stimulating hormone, adrenocorticotropic hormone, follicle-stimulating and luteinizing hormones, prolactin, and growth hormones; thirst; appetite; water balance; and sexual behavior.
The brain stem consists of the midbrain, pons, and medulla. Figure 18-4 shows the external anatomy of the brain stem. The brain stem is responsible for relaying all messages between the upper and lower levels of the central nervous system. Cranial nerves III to XII also arise from the brain stem. The brain stem contains the reticular formation, a network that provides for constant muscle stimulation to counteract the force of gravity. In addition to its antigravity effects, this area of the brain is essential for the control of consciousness. The neurons in the reticular activating system are capable of waking and arousing the entire brain.
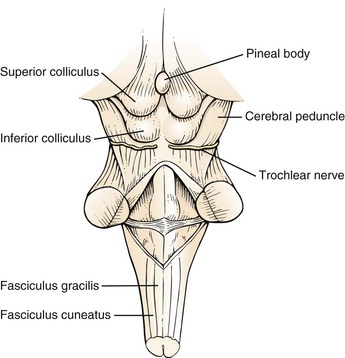
Figure 18–4 Anatomy of the brain stem.
The midbrain contains the superior and inferior colliculi, the cerebral peduncles, and the motor nuclei of the trochlear (cranial nerve IV) and oculomotor (cranial nerve III) nerves. The superior colliculi are associated with the visual system, and the inferior colliculi are associated with the auditory system. The cerebral peduncles converge from the inferior aspect of the cerebral hemispheres and enter the pons. A destructive lesion of the superior colliculi causes paralysis of upward gaze. Destructive lesions of the cranial nerve nuclei produce paralysis of the affected nerve. A destructive lesion of the cerebral peduncle gives rise to spastic paralysis on the other side of the body. Destruction of other tracts in the midbrain results in rigidity and involuntary movements.
The pons lies ventral to the cerebellum and rostral to the medulla. The abducens, facial, and acoustic (and vestibular) nuclei are found in the pons, and their nerves exit through a groove that divides the pons from the medulla. The motor and sensory nuclei of the trigeminal nerve are also located in the pons. At this level, the corticospinal tracts (also known as the pyramidal tracts) have not yet crossed, and a lesion at this level produces loss of voluntary movement on the opposite side. Destructive lesions of the pons may produce a variety of clinical syndromes, such as the following:
• Contralateral hemiplegia with ipsilateral facial palsy (Bell’s palsy)
The medulla is the portion of the brain stem between the pons and the spinal cord. The nuclei of the hypoglossal, vagus, glossopharyngeal, and spinal accessory nerves are located in the medulla. It is within the medulla that the majority of fibers in the corticospinal tracts cross to the opposite side. Destructive lesions in the medulla produce symptoms that are referable to the tracts interrupted by the lesion. Some clinical syndromes are as follows:
• Contralateral hemiplegia with ipsilateral hypoglossal palsy1
• Ipsilateral vagal palsy2 with contralateral loss of pain and temperature sense
• Ipsilateral vagal palsy with ipsilateral spinal accessory palsy3
• Ipsilateral vagal palsy with ipsilateral hypoglossal palsy
• Ipsilateral vagal palsy, ipsilateral spinal accessory palsy, and ipsilateral hypoglossal palsy
The cerebellum is located in the posterior fossa of the skull and is composed of a small midline vermis and two large lateral hemispheres. The cerebellum acts to keep the individual oriented in space and to halt or check motions. The cerebellum is also responsible for the fine movements of the hands. Essentially, the cerebellum coordinates and refines the action of muscle groups to produce steady and precise movements. Destructive lesions of the cerebellum cause swaying, staggering, intention tremors,4 and inability to change movements rapidly.
Of the blood supply to the brain, 80% is through the internal carotid arteries and 20% is through the vertebral basilar arteries. Each internal carotid artery terminates at the anterior cerebral and middle cerebral arteries. The posterior cerebral artery arises from the basilar artery, which joins with the posterior communicating artery, a branch of the internal carotid artery. The two anterior cerebral arteries are joined by the anterior communicating artery. This vascular network forms the circle of Willis, located at the base of the brain. This is illustrated in Figure 18-5.
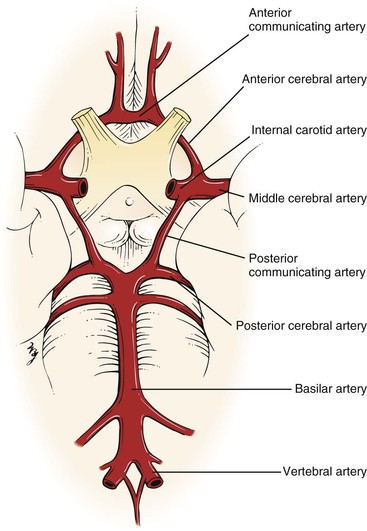
Figure 18–5 Circle of Willis.
Continuous with the medulla is the spinal cord, a cylindric mass of neuronal tissue measuring 40 to 50 cm in length in adults. Its distal end attaches to the first segment of the coccyx. The spinal cord is divided into two symmetric halves by the anterior median fissure and the posterior median sulcus. Each half contains white and gray matter, which can be further subdivided. This is illustrated in Figure 18-6.
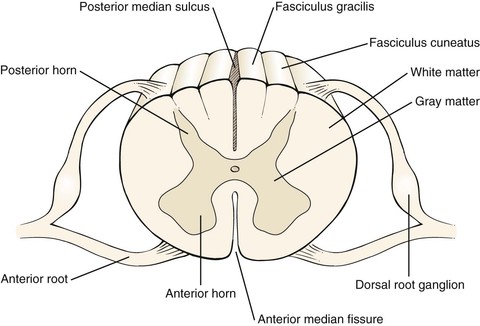
Figure 18–6 Cross-sectional view through the spinal cord.
The white matter of the spinal cord consists of tracts that link segments of the spinal cord and connect it to the brain. There are three main columns (funiculi). Between the anterior median fissure and the anterolateral sulcus is the anterior white column, which contains the descending fibers of the ventral corticospinal tract and the ascending fibers of the ventral spinothalamic tract. The ventral corticospinal tract is involved with voluntary motion, and the ventral spinothalamic tract carries impulses related to light touch.
The lateral white column is located between the anterolateral and posterolateral sulci and contains the descending fibers of the lateral corticospinal tract and the ascending spinocerebellar and lateral spinothalamic tracts. The lateral corticospinal tract is responsible for voluntary movement; the spinocerebellar tracts, for reflex proprioception; and the lateral spinothalamic tract, for pain and temperature sensation.
The posterior white column is located between the posterolateral and posterior median sulci. The most important fibers in this column are the ascending fibers of the fasciculus gracilis and fasciculus cuneatus. These tracts are involved with vibration sense, passive motion, joint position, and two-point discrimination.
There are 31 pairs of spinal nerves, each with a ventral (motor) and dorsal (sensory) root. The ventral root consists of efferent nerve fibers, which originate in the anterior and lateral gray matter (T1 to T2 only) and travel to the peripheral nerve and muscle, which constitute the motor root. The dorsal root consists of afferent nerve fibers whose cell bodies are in the dorsal root ganglion, which is the sensory root.
The spinal nerves are grouped into 8 cervical (C1 to C8), 12 thoracic (T1 to T12), 5 lumbar (L1 to L5), 5 sacral (S1 to S5), and 1 coccygeal nerve. These nerves are illustrated in Figure 18-7.
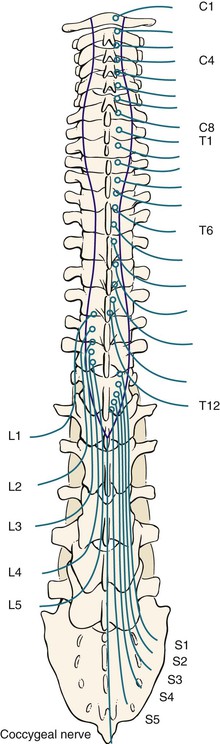
Figure 18–7 Spinal nerves.
A spinal reflex involves an afferent neuron and an efferent neuron at the same level in the spinal cord. The basis for this reflex arc is an intact sensory limb, functional synapses in the spinal cord, an intact motor limb, and a muscle capable of responding. The afferent and efferent limbs travel together in the same spinal nerve. When a stretched muscle is suddenly stretched further, the afferent sensory limb sends impulses through its spinal nerve that travel to the dorsal root of that nerve. After reaching a synapse in the gray matter of the spinal cord, the impulse is transmitted to the ventral nerve root. These impulses are then conducted through the ventral root to the neuromuscular junction, where a brisk contraction of the muscle completes the reflex arc. Figure 18-8 illustrates a reflex spinal arc.
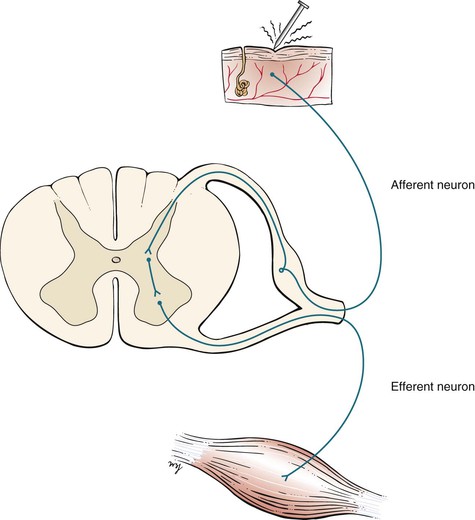
Figure 18–8 Reflex spinal arc.
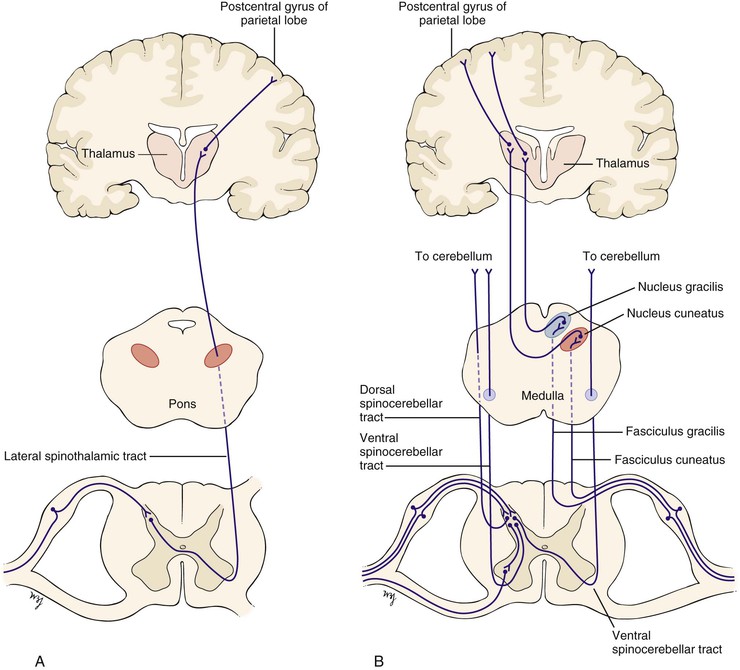
The afferent sensory limb is important not only in the reflex arc but also in the conscious appreciation of sensation. Nerve fibers carrying pain and temperature sensation enter the spinal cord and cross to the other side within one or two spinal segments. They ascend in the contralateral lateral spinothalamic tract, travel through the brain stem and the thalamus, and end in the postcentral gyrus of the parietal lobe, as illustrated in Figure 18-9A. Fibers carrying proprioceptive sensation from muscles, joints, and tendons enter the dorsal root and participate in the reflex arc. Other fibers carrying proprioceptive sensation pass directly into the posterior columns and ascend in the fasciculi gracilis and cuneatus to their ipsilateral nuclei, cross in the medial lemniscus, reach a synapse in the thalamus, and end in the postcentral gyrus of the parietal lobe. Still other proprioceptive fibers ascend crossed and uncrossed in the spinocerebellar tracts to the cerebellum. These additional pathways are illustrated in Figure 18-9B.
Review of Specific Symptoms
The most common symptoms of neurologic disease are as follows:
Headache
Headache is the most common neurologic symptom. It has been estimated that more than 35 million individuals in the United States suffer from recurrent headaches. Most of these patients have headaches that are related to migraine, muscle contraction, or tension. A headache pattern that is unchanged and has been present for several years is unlikely to be related to present illness of the patient. Several points must be clarified for any patient complaining of a recent change in the frequency or severity of headaches. Ask the following questions:
“How long have you been having headaches?”
“When did you notice a change in the pattern or severity of your headaches?”
“How has the pattern of your headaches changed?”
“How often do your headaches occur?”
“How long does each headache last?”
“Which part of your head aches?”
“What does the headache feel like?”
“How quickly does the headache reach its maximum?”
“When you get headaches, do you have any other symptoms?”
“Are you aware of anything that produces the headaches?”
“Are there any warning signs?”
Patients complaining of a sudden onset of headache usually have more serious illnesses than patients with headaches of chronic duration. A continuous headache can be related to muscle spasm, whereas a recurrent headache may be a migraine or cluster headache. A throbbing headache often has a vascular cause. Certain headaches are associated with visual phenomena, nausea, or vomiting. In patients with increased intracranial pressure, any maneuver that increases the pressure, such as coughing or bending, may worsen the headache. In any patient who experiences a severe, sudden headache, stroke should be suspected.
Migraine is a biphasic type of headache associated with a prodromal phase, called the aura, followed by the headache phase. During the aura, one or more physiologic events may occur. These include transient experiences of autonomic, visual, motor, or sensory phenomena. Common visual symptoms are photophobia, blurred vision, and scotomata. As the aura fades, the headache begins. It is usually unilateral and is often described as pulsating; it can last for hours to days. Migraine headaches are often triggered by stress, anxiety, the use of birth control pills, and hormonal changes. Many patients experience migraine headaches after a period of excitement. Other important triggers are hunger and the ingestion of certain foods such as chocolate, cheese, cured meats, and highly spiced foods. There is often a family history of migraine.
Cluster headaches are associated with oculosympathetic disturbances. The typical patient is a middle-aged man complaining of recurrent episodes of pain around the eye that last for up to 1 hour. Classically, cluster headaches awaken the patient from sleep on successive nights for 2 to 4 weeks. There is ipsilateral miosis, ptosis, conjunctival edema, tearing, and nasal stuffiness during the headache. It is thought that alcohol may precipitate such attacks.
Headache may be the result of referred pain from sinus infections, ocular disease, or dental disease. Systemic conditions such as viral infections, chronic obstructive pulmonary disease, and poisoning may produce headaches. Determine whether the patient is taking any medications that may be producing the head pain. (See Table 18-2, which provides an approach to patients with the symptom of headache.)
Loss of Consciousness
Loss of consciousness—syncope—may result from cardiovascular or neurologic causes. The cardiovascular causes are discussed in Chapter 11, The Heart, and Chapter 12, The Peripheral Vascular System. The term blackout is commonly used, but it may mean different conditions to the patient and the interviewer. Any patient who uses this term should be asked to clarify its meaning. The patient may be referring to an actual loss of consciousness, a dimming of vision, or a decreased awareness of the environment without an actual loss of consciousness.
A useful way to clarify the symptom of loss of consciousness is to ask the patient, “Have you ever lost consciousness, fainted, or felt that you were not aware of your surroundings?” If the patient answers in the affirmative, identify the cause of the loss of consciousness. Ask the following questions:
“Can you describe the attack to me—every event as it occurred until you lost consciousness?”
“Did anyone witness the attack?”5
“Were there any symptoms that preceded the attack?”
“Were you told that there were body movements?”
“Can you describe everything you remember after the attack until you felt completely normal?”
“Was there a period of sleepiness that followed?” If yes, “For how long did this period last?”
“How did you feel after the attack? Were you confused?”
“Did you notice afterward that you had urinated or had a bowel movement during the attack?”
Epileptic seizures may produce a loss of consciousness and are caused by the sudden, excessive, disorderly discharge of neurons. The first step in approaching the symptom of seizure is to identify its type. If the discharge is focal, the clinical seizure reflects the effect of the excessive discharge in that area of the body. For example, if the discharge is located in the inferior precentral gyrus, involved with hand and arm motion, the seizure is characterized by involuntary motion of the hand and arm. A generalized seizure results from a discharge in the subcortical structures, such as the thalamocortical radiations. These have widespread bilateral cortical connections. There are three main types of generalized seizures:
A petit mal seizure is characterized by a sudden attack of unconsciousness lasting only about 10 seconds, usually without any warning. During the petit mal seizure, the patient appears to be staring or daydreaming. There is no associated falling or involuntary limb motion. The patient rapidly returns to normal activity without being aware of the attack. These seizures are most common in children 5 to 15 years of age. On occasion, they may persist into adulthood.
A grand mal seizure is a generalized major motor convulsion. Affected patients lose consciousness, and many fall down rigidly. In 50% of patients with grand mal seizures, there is an aura of giddiness, involuntary twitching, change in mood, confusion, or epigastric discomfort as the seizure begins. Some patients may cry out initially. During this tonic phase, there is an increase in muscle tone, resulting in a rigid, flexed posture and then a rigid, extended posture. The patient may become apneic and cyanotic. The eyes may open and stare or may be deviated to one side. The clonic phase follows, with involuntary movements of the body. These are often associated with salivation, eye rolling, and incontinence. Biting the tongue is common. After the clonic phase, the individual passes into a phase resembling sleep from which she or he cannot be easily awakened. Postictally, or after the seizure, the patient may be confused and often falls into a deep sleep that lasts for hours. Accompanying muscle pain and headache are common.
A myoclonic seizure is a minor motor seizure characterized by sudden muscle contractions of the face and upper extremities. The eyelids and forearms are commonly affected. There is no detectable loss of consciousness.
Febrile convulsions are common in children from 6 months to 6 years of age and are similar to grand mal seizures. When a child has a high fever, a seizure lasting less than 10 minutes may occur. The younger the child is at the time of the first febrile seizure, the greater is the likelihood that seizures will recur.
“Dizziness”
Dizziness is a term used frequently by patients and should be avoided by the interviewer. “Dizziness” may be the patient’s description of vertigo, ataxia, or lightheadedness. Any time the patient uses this term, it must be clarified by additional questioning, because different pathophysiologic mechanisms may be responsible. The interviewer needs to differentiate vertigo from ataxia. If the patient complains of “dizziness,” it is important to ask these questions:
“Would you describe the dizziness as a strange spinning sensation in your head?”
“Did the room spin, or did it feel as if you were spinning?”
Vertigo is partially discussed in Chapter 8, The Ear and Nose. Vertigo is the hallucination of movement. Acute vertigo may be associated with nausea, vomiting, perspiration, and a sense of anxiety. Ask patients whether they have the sensation that objects are moving around them or that they are spinning or moving. In addition to the questions in Chapter 8, ask the following:
“During the attack, did you experience any nausea or vomiting?”
“Have you noticed any problem with your hearing or ringing in your ears?”
Ménière‘s disease can result in protracted attacks of severe vertigo associated with vomiting. Many patients with Ménière’s disease also have the symptoms of tinnitus and hearing loss. During the attack, the patient is unsteady, with horizontal nystagmus directed away from the affected ear. Certain drugs (such as gentamicin) are associated with changes in the labyrinth of the ear and can cause vertigo and deafness.
Dizziness and stumbling are commonly associated with a stroke.
Ataxia
Disruption of the vestibular-ocular-cerebellar control mechanism produces ataxia. Ataxia is persistent unsteadiness in the upright position. Any patient complaining of dizziness must be evaluated for abnormal function of the vestibular, visual, proprioceptive, and cerebellar systems. Equilibrium requires the integration of sensory input and motor output, acting primarily at a reflex level for the maintenance of balance. The ears and eyes and their central connections in the brain stem and the cerebellum are intimately involved in balance. Any patient with ataxia should be asked the following questions:
“Are you unsteady when you walk?”
“Have you noticed that the dizziness is worse when your eyes are open or closed?”
“What does your diet consist of? What did you eat yesterday?”
Abnormal proprioceptive input from the lower extremities can cause ataxia. Severe posterior column damage from syphilis, vitamin B12 deficiency, or multiple sclerosis may produce a “sensory” ataxia, resulting in a wide-based, high-stepping gait. The gait is worsened by having the patient close the eyes and is improved by having the patient observe the feet. Vitamin B12 deficiency may result from pernicious anemia or from inadequate intake, although poor nutrition is a rare cause. “Motor” ataxia results from an abnormality in the cerebellum and central vestibular pathways. It is characterized by wide-based, irregular placement of the feet and poor placement of the center of gravity, with a lurching to either side.
Changes in Consciousness
Changes in consciousness may be related to changes in attention span, perception, arousal, or a combination. In confusional states, the patient has the ability to receive information normally, but the processing is disturbed. In delirium, the individual perceives the information abnormally. Any patient, or member of the patient’s family, who indicates that a change in consciousness has occurred should be asked the following:
“Did the change occur suddenly?”
“Have there been other symptoms associated with the change in consciousness?”
“Do you use any medications? Depressants? Insulin? Alcohol? Recreational drugs?”
“Is there a history of psychiatric illness?”
“Is there a history of kidney disease? Liver disease? Thyroid disease?”
Many factors can produce changes in consciousness. The acuteness of the change in consciousness is often helpful in making a diagnosis. Hemiparesis, paresthesia, hemianopsia, garbled speech, and arm and leg weakness are common associated symptoms of supratentorial lesions. Brainstem lesions are often associated with changes in consciousness and with nystagmus, vomiting, double vision, nausea, and excessive yawning. Drugs of any type can produce acute changes in consciousness. A history of earlier psychiatric illness is important. Toxic and metabolic changes are frequently associated with changes in consciousness. Liver or kidney failure, myxedema, and diabetic ketoacidosis are common causes of metabolic abnormalities. A history of head trauma may result in a subdural hematoma and produce a gradual change in consciousness.
Visual Disturbance
Visual disturbances are common neurologic presenting symptoms. The most important symptoms are acute visual loss, chronic visual loss, and double vision. Ask any patient complaining of visual disturbances the following questions:
“How long have you noticed these visual changes?”
“Is the visual loss associated with pain?”
“Do you have a history of glaucoma?”
Acute painless visual loss is caused by either a vascular accident or a retinal detachment. Painless loss of vision over a longer period occurs with compression of the optic nerve or tract or radiation. Glaucoma is often the cause of chronic, insidious, painless loss of vision. Acute narrow-angle glaucoma, however, may be responsible for transient loss of vision in association with intense ocular pain. Episodes of migraine may produce transient episodes of visual loss before the development of the headache. Amaurosis fugax is transient visual loss lasting up to 3 minutes and is a feature of internal carotid artery disease.
Double vision, or diplopia, is discussed in Chapter 7, The Eye. Ocular motor palsies, thyroid abnormalities, myasthenia gravis, and brainstem lesions are well-known causes of diplopia. Ocular motor palsies can occur in trauma, multiple sclerosis, myasthenia gravis, aneurysms of the circle of Willis, diabetes, and tumors. Ask the following questions of any patient complaining of diplopia:
“In which field of gaze do you have double vision?”
“Did the double vision occur suddenly?”
“Was there any pain associated with the double vision?”
“Has there been any injury to your head or eye?”
“Have you ever been told that your blood pressure was elevated?”
“Does the double vision get worse when you are tired?”
“Have you been exposed to the AIDS [acquired immune deficiency syndrome] virus?”
When a cranial nerve is affected, resulting in an extraocular muscle palsy, the patient may complain of diplopia in one field of gaze when the affected eye is unable to move conjugately with the other. Ocular palsies involve the third, fourth, and sixth cranial nerves. A complete third (oculomotor) nerve palsy causes ptosis, mydriasis, and loss of all extraocular movements except abduction. Trauma, multiple sclerosis, tumors, and aneurysms are the most frequent causes. Aneurysms of the posterior communicating artery can involve the third nerve, which passes near the artery on its way to the cavernous sinus. Cavernous sinus thrombosis, not infrequently seen in patients with AIDS, may also produce a complete third nerve palsy. Pupil-sparing third nerve, fourth (trochlear) nerve, and sixth (abducens) nerve palsies are seen in diabetic patients and in patients with long-standing hypertension. Patients with myasthenia gravis often have diplopia in the later part of the day as the muscles tire and weaken.
Visual disturbances, including blocked vision or loss of vision in one eye, blurry vision, or “graying out” are seen frequently in patients suffering a stroke.
Dysphasia
Speech abnormalities, or dysphasia, may be either nonfluent (expressive) or fluent (receptive). In expressive aphasia, the speech pattern is hesitant and labored, with poor articulation. The patient has no problem with comprehension. When asked to say, “no ifs, ands, or buts,” the patient has great difficulty. In receptive aphasia, the speech is rapid and appears fluent but is full of syntax errors, with the omission of many words. Handwriting changes are nonspecific but indicate an impairment of neuromuscular control. Ask the following questions:
“Have you noticed any recent change in your speech pattern, such as slurring of your words?”
“Do you have trouble understanding things that are said to you?”
“Have you had any difficulty finding the right word in conversation?”
Language problems, as well as slurred speech, are found commonly in patients suffering a stroke.
Dementia
An important symptom of neurologic disease is failing memory. Dementia can be defined as the progressive impairment of orientation, memory, judgment, and other aspects of intellectual function. Dementia is a symptom rather than a specific disease entity. The most common cause of dementia is Alzheimer‘s disease. Other causes include Parkinson’s disease, vascular disorders, metabolic disorders, drugs, tumors, vitamin B12 deficiency, tertiary syphilis, and normal-pressure hydrocephalus. It is common for patients with early dementia to recognize an increasing inability to comprehend written material. They are aware also of their cognitive impairment but fail to acknowledge it with friends and family. It is often so insidious that individuals with dementia may live with their family for years without the family recognizing the problem. In addition, family members and friends may not wish to acknowledge the failing mental capacities.
Ask the patient and his or her friends and family the following:
“Have you noticed any change in your memory lately?”
“Do you have difficulty reading or understanding what you have read?”
“What was the patient’s personality like a few years ago?”
“When was the last time the patient seemed normal?”
“What does the patient’s diet consist of? Does he or she eat well?”
Cerebrovascular Accident
Strokes, or cerebrovascular accidents, are common. Most are thromboembolic (80%), but some are hemorrhagic (20%). Thirty percent of patients who sustain a stroke die within the first month. Most patients with strokes have paresis of at least one limb. Transient ischemic attacks (TIAs) are short episodes manifested by focal neurologic dysfunction. They usually last only a few minutes, after which complete recovery occurs. The importance of TIAs is that, in 30% of affected patients, a stroke occurs within 4 to 5 years.
Gait Disturbance
Gait disturbances may occur for a variety of reasons. Gait may be changed by local pain in the foot, pain in a joint, claudication of the hip or leg, bone disease, vestibular problems, and extrapyramidal disorders. Interruption of the corticospinal tracts in the cerebrum after a stroke produces a spastic weakness in the contralateral leg. The foot is dragged, and the whole leg appears stiff and extended. Lesions in the spinal cord may produce a spastic paralysis affecting both legs. The gait is slow and stiff, with small steps. Patients with Parkinson’s disease walk stooped over, with short, quick, shuffling steps. Any patient with a gait disturbance should be asked the following:
Patients with vascular occlusive disease of the hip or leg may experience pain while walking and may alter their gait. Diabetes, syphilis, and pernicious anemia may produce a sensory loss, and each condition can result in gait abnormalities.
Tremor
A tremor is a rhythmic motion of the distal parts of the limbs or head. A physiologic tremor has an oscillation of 10 to 12 cycles per second and is more obvious after exercise. A pathologic tremor is slower. Parkinson‘s disease is the most frequently encountered extrapyramidal movement disorder. In this condition, the tremor is present at rest and is decreased with action. It has a frequency of three to six cycles per second and is worsened by anxiety. An intention, or ataxic, tremor is slow (two to four cycles per second) and worsens on attempted movement. Multiple sclerosis is one of the many causes of intention tremor. Metabolic problems from liver or kidney failure are frequently responsible. Withdrawal from alcohol or caffeine is often a precipitating factor. Any patient with the symptom of tremor should be asked these questions:
“Does the tremor worsen when you try to do something?”
“Is there a history of thyroid disease?”
“Have you ever been told about any problems with your liver or kidneys?”
“What is your daily consumption of alcoholic beverages?”
Chorea is involuntary jerky motions of the face and limbs. A common cause is Huntington‘s disease, in which chorea is accompanied by personality changes and progressive mental deterioration terminating in dementia.
“Numbness”
Numbness is another term used by patients to indicate a variety of problems. “Numbness” can be used by patients to describe a “pins-and-needles” sensation, coolness, pain, or clumsiness. The interviewer should be sure to clarify the meaning. The examiner must be careful during the physical examination to palpate the distal pulses in any patient complaining of numbness, because arterial insufficiency is a possible cause. Diabetes mellitus is a common cause of lower extremity numbness. Multiple sclerosis may cause numbness in any extremity.
“Weakness”
Weakness may be a symptom of the motor system. A patient with a proximal arm motor weakness complains of difficulty brushing hair, shaving, or reaching up to shelves. A patient with distal arm motor weakness complains of difficulty putting a button through a buttonhole, using keys, or writing with a pen or pencil. Proximal leg motor weakness is characterized by difficulty climbing stairs or getting into bed or the bathtub. Footdrop is a classic sign of distal leg motor weakness. Chapter 17, The Musculoskeletal System, reviews some of the important questions related to weakness.
Face droop and weakness are common signs of a stroke, as is the presence of numbness or clumsiness in one arm or hand.
Pain
Pain is an infrequent symptom of neurologic disease, but it merits mention. Trigeminal neuralgia, also known as tic douloureux, is the occurrence of severe, jabbing pain lasting only seconds in the distribution of the maxillary or mandibular divisions of the trigeminal nerve (Fig. 18-10). It is frequently provoked by motion, touch, eating, or exposure to cold temperatures. Another cause of facial pain is the cluster headache, already discussed. Herpes zoster infection of a sensory nerve root, also known as shingles, manifests with intense pain along the distribution of that nerve root. The classic linear, vesicular skin eruption develops 3 to 4 days later along the distribution of the nerve. Figure 5-70 shows the classic dermatologic manifestations of herpes zoster infection of spinal nerve T3.
Sciatica is intense pain shooting down the leg in the distribution of the sciatic nerve. In this condition, there is impingement of portions of the sciatic nerve by the vertebrae. Arthritis of the lumbosacral spine is frequently the cause.
Sometimes the paresthesias associated with demyelinating diseases are so intense that the patient may describe them as pain.
Patients with inflammation of the meninges often complain of pain in the neck and a resistance to flexion of the neck. If meningitis is suspected, have the patient lie on his or her back. Place your hand behind the patient’s neck and flex it until the chin touches the sternum. In patients with meningitis, there is neck pain and resistance to motion. This is called Brudzinski‘s sign. There may also be flexion of the patient’s hips and knees. Jósef Brudzinski described at least five different physical signs indicative of meningeal irritation. This sign is the best known and most reliable sign. Another sign of meningeal irritation can be elicited while the patient lies on the back and you flex one of the patient’s legs at the hip and knee. If pain or resistance is elicited as the knee is extended, a positive Kernig‘s sign is present.
Effect of Chronic Neurologic Disease on the Patient
The ramifications of chronic neurologic disease on the patient and his or her family are enormous. All family members experience emotional pain while observing the progressive clinical changes. The family bears an immense personal burden in assisting the patient to cope with disability.
One example of a progressive neurologic condition is Alzheimer’s disease. A devastating chronic disorder of unknown cause, Alzheimer’s disease is the most common diffuse brain degeneration causing brain failure. This condition is characterized by progressive and widespread brain degeneration with a hopeless prognosis.
Memory problems and impairment of intellectual function are the main symptoms of Alzheimer’s disease. Depression is common. Patients may have significant cognitive impairment, which ruins their ability to negotiate their environment. They may forget where they live. They may forget to turn off a gas burner on the stove or to put out a cigarette. They may wander aimlessly outdoors.
Manifestations of Alzheimer’s disease span a clinical spectrum from awareness of the disability to a vegetative state. Many patients lose touch with reality. During an interview with such a patient, it may become clear that even the ability to describe the patient’s own medical history has been lost.
Early in the course of the disease, affected patients may use a number of circumlocutions, such as substituting words when they cannot find more appropriate ones. Another early change is disorientation with regard to time and place. Visual hallucinations are common. Lack of interest in sex is almost universal. Motor behavior diminishes progressively as impairment of consciousness increases. An important characteristic is the development of bizarre thoughts and fantasies that come to dominate consciousness. Delusions, especially delusions of persecution, are common.
In the early stages of the disease—when patients are still aware of their environment but have experienced the symptom of memory loss—mild depression, anxiety, and irritability are common. As the disease progresses, apathy is the dominant feature. Patients may actually appear indifferent and emotionally withdrawn. In others in whom there is increased motor activity, anxiety and fear are common. In these individuals, terror and panic attacks are not uncommon. Hostility and paranoia develop rapidly. Regression and sudden displays of highly charged emotion are the responses to their frequent hallucinations.
In milder cases, depression, hypochondriasis, and phobic features abound. Hysterical conversion reactions, such as hysterical blindness, may occur. Social interaction is lost, and the patient may suddenly explode with anger, anxiety, or tears. As the disease progresses, suicide attempts are common. Emotional lability is often extreme, with periods of laughter followed by crying. With progressive disease, dullness of affect and lack of an emotional response occur as gross neurologic disability develops. In the terminal stages, patients with Alzheimer’s disease may show severe body wasting with profound brain failure.
Physical Examination
The equipment necessary for the neurologic examination consists of safety pins, cotton-tipped applicators, a 128-Hz tuning fork for vibration sense, a 512-Hz tuning fork for hearing, gauze pads, familiar objects (coins, keys), and a reflex hammer.
The neurologic examination consists of assessment of the following:
• Reflexes
Mental Status


During the interview, the examiner has already gained much insight into the mental status of the patient. The interviewer may have already been able to assess the patient’s remote memory, affect, and judgment. The formal mental status portion of the neurologic examination is introduced by saying to the patient, “I would like to ask you a few routine questions. Some of them you will find very easy. Others will be more difficult. Do the best you can.”
The mental status examination consists of evaluation of the following:
Assess Level of Consciousness
The level of consciousness can be assessed as soon as you introduce yourself to the patient. Is the patient awake? Alert? Is the patient’s sensorium clouded by exogenous or endogenous insults? Does the patient appear confused? If the patient does not respond to your introduction, hold the patient’s hand and softly say, “Hello, Mr./Ms. ____. Can you hear me? If you hear me, squeeze my hand.” If there is no response, try gently shaking the patient. If there is still no response and the patient appears obtunded, squeezing the nipple or applying pressure with your thumb to the bony ridge under the eyebrow is a painful maneuver that may rouse the patient. If these maneuvers fail to awaken the patient, the patient is in coma. Patients who are in coma are completely unconscious and cannot be roused even by painful stimuli. If either painful stimulus is used, be careful not to pinch the skin or bruise the patient. If friends or relatives are present, make sure to explain to them what you are doing.
Evaluate Speech
If the patient is awake and alert, you have already observed his or her speech. The patient should now be asked to recite short phrases such as “no ifs, ands, or buts.” Is dysarthria, dysphonia, dysphasia, or aphasia present? Dysarthria is difficulty in articulation. In general, lesions of the tongue and palate are responsible for dysarthria. Dysphonia is difficulty in phonation. The result is an alteration in the volume and tone of the voice. Lesions of the palate and vocal cords are often responsible. Dysphasia is difficulty comprehending or speaking as a result of cerebral dysfunction. Patients with a total loss of speech have aphasia. Different areas of the brain are responsible for the different types of aphasia. A motor, expressive, nonfluent aphasia is present when patients know what they want to say but have motor impairment and cannot articulate properly. They understand written and verbal commands but cannot repeat them. A frontal lobe lesion is often the cause. A sensory, receptive, fluent aphasia is present when the patient articulates spontaneously but uses words inappropriately. The patient has difficulty understanding written and verbal commands and cannot repeat them. A temporoparietal lesion is frequently the cause.
Evaluate Orientation
The patient’s orientation to person, place, and time must be established. Orientation refers to the person’s awareness of self in relation to other persons, places, and time. Disorientation occurs in association with impairment of memory and attention span. The patient should be asked these questions:
To evaluate orientation, do not ask if the patient knows his or her name or other questions that cannot be verified. Patients with an early cognitive impairment are cagey in providing answers if they do not know the correct answer; they hope that you will accept their answer and not pursue the question. As an example, if an examiner asks, “Where are you now,” and the patient does not remember the address, he or she might reply with an answer like, “I’m in your office.” You should then ask, “But where is my office?”
Evaluate Knowledge of Current Events
Knowledge of current events can be assessed by asking the patient to name the last four presidents of the United States. Asking the patient the name of the local mayor or governor is also useful. If the patient is not American or is unfamiliar with American affairs, asking the patient about more general current events may be more useful. The ability to name current events requires an intact orientation, intact recent memory, and the ability to think abstractly.
Assess Judgment
Evaluation of judgment is performed by asking the patient to interpret a simple problem. Ask the patient the following:
A correct response to the first question would be to pick up the letter and mail it. An example of an incorrect response might be, “I’d throw it in the trash.” Judgment requires higher cerebral function.
Assess Abstraction
Abstraction is a higher cerebral function that requires comprehension and judgment. Proverbs are commonly used to test abstract reasoning. The patient should be asked to interpret the following:
A patient with an abnormality in abstract reasoning might respond to the first quotation with a concrete interpretation, such as, “The glass will break if you throw a stone through it.” A concrete interpretation of the second proverb might be “Moss grows only under rocks that don’t move and not under a rolling stone.” Concrete responses are common in patients with mental retardation or brain failure. Schizophrenic patients often answer with concrete interpretations, but bizarre assessments are also common. Be careful when assessing abstraction in patients whose mother tongue is not English. They may also provide concrete answers as they literally translate the words of the proverb.
Another method of testing abstract reasoning is to ask the patient how two items are similar or dissimilar. You might ask, “What is similar about a dog and a cat?” “What is similar about a church and a synagogue?” or “What is dissimilar about an apple and a chicken?”
Assess Vocabulary
Vocabulary is often difficult to assess. It is based on many factors, which include the patient’s education, background, work, environment, and cerebral function. It is, however, an important parameter in assessing intellectual capacity. Patients who are mentally retarded have a limited vocabulary, whereas those with mild brain failure have a well-preserved vocabulary. Patients should be asked to define words or use them in sentences. Any words can be used, but they should be asked in order of increasing level of difficulty. The following list is an example:
Assess Emotional Responses
Although emotional response has probably been informally observed already, inquire specifically whether the patient has noticed any sudden mood changes. It is appropriate to ask, “How are your spirits?” During the interview, the interviewer has already noticed the patient’s affect, which is the emotional response to an event. The response may be appropriate, abnormal, or flat. An appropriate response to a loved one’s death may be to cry. An inappropriate response is to laugh. A flat response shows little emotion. Patients with bilateral cerebral damage lose control of their emotions.
Assess Memory
To test memory, have the patient recall the recent and the remote past. Recent memory is easily tested by presenting three words to the patient and asking for them to be repeated 5 minutes later. For example, tell the patient, “Repeat these words after me and remember them. I will ask for them later: necklace, thirty-two, barn.” Continue with the mental status examination. Five minutes later, ask the patient, “What were those words I asked you to remember?”
A simpler test of memory is to have the patient recall as many elements in a category as possible. Request that the patient do one of the following:
An abnormality in recent memory may be related to a lesion in the temporal lobe.
To test the remote past memory, ask the patient about well-known events in the past. Do not ask about events that you cannot verify.
Assess Calculation Ability
The ability to calculate depends on the integrity of the dominant cerebral hemisphere, as well as on the patient’s intelligence. Ask the patient to perform simple arithmetic problems, such as subtracting 7 from 100, then 7 from the result, then 7 from the result, and so forth. This is the serial sevens test. If there is difficulty with serial sevens, ask the patient to add or subtract several numbers, such as “How much is 5 plus 7? How much is 12 plus 9? How much is 27 minus 9?”
Assess Object Recognition
Object recognition is termed gnosia. Agnosia is the failure to recognize a sensory stimulus despite normal primary sensation. Show the patient a series of well-known objects, such as coins, pens, eyeglasses, or pieces of clothing, and ask the patient to name them. If the patient has normal vision and fails to recognize the object, visual agnosia is present. Tactile agnosia is the inability to recognize an object by palpation in the absence of a sensory deficit. This occurs with a lesion in the nondominant parietal lobe. Autotopagnosia is the term used to describe a patient’s inability to recognize his or her own body part, such as the hand or leg.
Assess Praxis
Praxis is the ability to perform a motor activity. Apraxia is the inability to perform a voluntary movement in the absence of deficits in motor strength, sensation, or coordination. Dyspraxia is the decreased ability to perform the activity. The patient hears and understands the command but cannot integrate the motor activities that will complete the action. Ask a patient to pour water from the bedside pitcher into a glass and drink the water. A patient with dyspraxia may either drink the water from the pitcher or try to drink from the empty glass. A deep frontal lobe lesion is frequently responsible for this disorder.
Another type of apraxia is constructional apraxia. In this condition, the patient is unable to construct or draw simple designs. The examiner draws a shape and asks the patient to copy it. Alternatively, the patient can be asked to draw the face of a clock. Patients with constructional apraxia often have a lesion in the posterior portion of the parietal lobe.
Cranial Nerves
The examination of the cranial nerves should be carried out in an orderly manner. Several of the cranial nerves have already been evaluated. Table 18-1 lists the cranial nerves, their functions, and the clinical findings when a lesion exists.
Table 18–1
Cranial Nerves
| Cranial Nerve | Function | Clinical Findings with Lesion |
| I: Olfactory | Smell | Anosmia |
| II: Optic | Vision | Amaurosis |
| III: Oculomotor | Eye movements, papillary constriction, accommodation | Diplopia, ptosis, mydriasis, loss of accommodation |
| IV: Trochlear | Eye movements | Diplopia |
| V: Trigeminal | General sensation of face, scalp, and teeth; chewing movements | “Numbness” of face; weakness of jaw muscles |
| VI: Abducens | Eye movements | Diplopia |
| VII: Facial | Taste; general sensation of palate and external ear; lacrimal gland and submandibular and sublingual gland secretion; facial expression | Loss of taste on anterior two thirds of tongue, dry mouth, loss of lacrimation, paralysis of facial muscles |
| VIII: Vestibulocochlear | Hearing; equilibrium | Deafness, tinnitus, vertigo, nystagmus |
| IX: Glossopharyngeal | Taste, general sensation of pharynx and ear, elevation of palate, parotid gland secretion | Loss of taste on posterior one third of tongue, anesthesia of pharynx, partially dry mouth |
| X: Vagus | Taste; general sensation of pharynx, larynx, and ear; swallowing; phonation; parasympathetic innervation to heart and abdominal viscera | Dysphagia, hoarseness, palatal paralysis |
| XI: Spinal accessory | Phonation; head, neck, and shoulder movements | Hoarseness; weakness of head, neck, and shoulder muscles |
| XII: Hypoglossal | Tongue movements | Weakness and wasting of tongue |
Cranial Nerve I: Olfactory
The olfactory nerve supplies nerve endings to the superior nasal concha and upper one third of the nasal septum. The olfactory nerve is not routinely tested. However, in any patient with a suspected frontal lobe disorder, the olfactory nerve should be evaluated.
Test Olfaction
The patient is asked to close the eyes and one nostril as the examiner brings a test substance close to the patient’s other nostril. The patient is instructed to sniff the test substance. The substance must be volatile and nonirritating, such as cloves, vanilla beans, freshly ground coffee, or lavender. The use of an irritating agent such as alcohol would involve cranial nerve V, as well as cranial nerve I, and the test results would be inaccurate.
Each nostril is tested separately. The examiner asks the patient to identify the test material. A unilateral loss of smell, known as unilateral anosmia, is more important than a bilateral loss, because it indicates a lesion affecting the olfactory nerve or tract on that side.
Cranial Nerve II: Optic

The optic nerve ends in the retina. The examinations for visual acuity and the ophthalmoscopic examination are discussed in Chapter 7, The Eye.
Cranial Nerve III: Oculomotor

The oculomotor nerve supplies the medial, superior, and inferior rectus muscles and the inferior oblique muscle, which control most eye movements. The third nerve also innervates the intrinsic muscles, controlling pupillary constriction and accommodation.
Extraocular muscle movements are discussed in Chapter 7. A patient with an oculomotor palsy is shown in Figure 7-150. The pupillary light reflex depends on the function of cranial nerves II and III (see Chapter 7). Visual fields are part of both the eye examination and the neurologic examination. The technique for visual field testing is discussed in Chapter 7.
Cranial Nerve IV: Trochlear

The trochlear nerve is responsible for movement of the superior oblique muscle. Extraocular muscle movements are discussed in Chapter 7.
Cranial Nerve V: Trigeminal

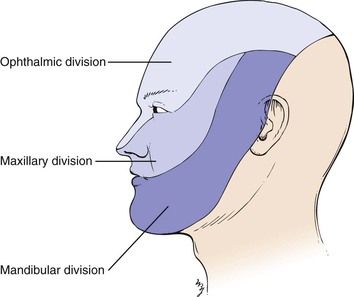
The trigeminal nerve is responsible for supplying sensation to the face, the nasal and buccal mucosa, and the teeth. The motor division supplies the muscles of mastication. The three major subdivisions of the trigeminal nerve are the ophthalmic, the maxillary, and the mandibular. These divisions are illustrated in Figure 18-10.
The ophthalmic division supplies sensation to the frontal sinuses, the conjunctiva, the cornea, the upper eyelid, the bridge of the nose, the forehead, and the scalp as far as the vertex of the skull. The maxillary division supplies sensation to the cheek, the maxillary sinus, the lateral aspects of the nose, the upper teeth, the nasal pharynx, the hard palate, and the uvula. The mandibular division supplies sensation to the chin, the lower jaw, the anterior two thirds of the tongue, the lower teeth, the gums and floor of the mouth, and the buccal mucosa of the cheek. The motor division innervates the muscles of mastication and the tensor tympani.
The examination of the trigeminal nerve consists of the following:
Test Corneal Reflex
The corneal reflex depends on the function of cranial nerves V and VII. To evaluate the corneal reflex, the examiner uses a cotton-tipped applicator, the tip of which has been pulled into a thin strand about 1.3 cm in length. The examiner stabilizes the patient’s head by placing a hand on the patient’s eyebrow and head. The patient is asked to look to the left side as the cotton tip is brought in from the right side to touch the right cornea gently. This is demonstrated in Figure 18-11. A prompt bilateral reflex closure of the eyelids is the normal response. The examination is repeated on the other side by reversing the directions.

Figure 18–11 Technique for evaluating the corneal reflex.
The responses on the two sides are compared. The sensory limb of the corneal reflex is the ophthalmic division of the trigeminal nerve; the motor limb is conducted through the facial nerve.
In performing the corneal reflex test, touch the cornea and not the eyelashes or conjunctiva, which will elicit an inaccurate result.
Test Sensory Function
The sensory function of the trigeminal nerve is tested by asking the patient to close the eyes and to respond when a touch is felt. A piece of gauze is brushed against one side of the forehead and then the corresponding position on the other side. This test is then performed on the cheeks and the jaw, so that all three subdivisions of the nerve are tested. The patient is also asked whether one side feels the same as or different from the other side. The examination is demonstrated in Figure 18-12.

Test Motor Function
The motor function of the trigeminal nerve is tested by having the patient bite down or clench the teeth while the masseter and temporalis muscles are palpated bilaterally. This is demonstrated in Figure 18-13. Unilateral weakness causes the jaw to deviate toward the side of the lesion.

Cranial Nerve VI: Abducens

The abducens nerve is responsible for movement of the lateral rectus muscle. Extraocular muscle movements are discussed in Chapter 7, The Eye.
Cranial Nerve VII: Facial

The facial nerve innervates the facial muscles and enables taste on the anterior two thirds of the tongue. A small component also supplies general sensation to the external ear. The facial nerve carries parasympathetic motor fibers to the salivary glands and chorda tympani. Testing for abnormalities of taste is usually not performed by an internist.
Test Motor Function
The patient is asked to bare the teeth while the examiner observes for asymmetry. The patient is asked to puff out the cheeks against resistance and then to wrinkle the forehead. It is helpful if the examiner actually demonstrates these maneuvers for the patient. These maneuvers are demonstrated in Figure 18-14.
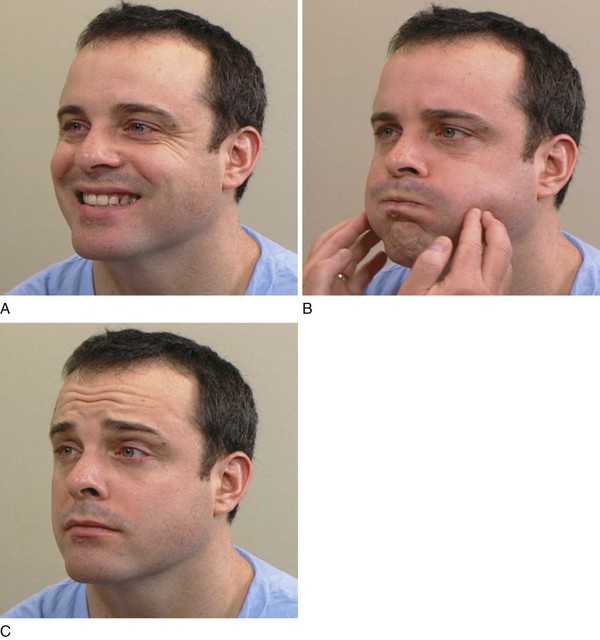
Figure 18–14 Testing the facial nerve. A and B, Tests for the lower division. C, Test for the upper division.
The patient is then asked to close the eyes tightly while the examiner tries to open them. The patient is told to close the eyes as tightly as possible. The examiner can say, “Don’t let me open them.” This procedure is demonstrated in Figure 18-15A. Each eye is examined separately, and the strengths are compared. Normally the examiner should not be able to open the patient’s eyes. The patient in Figure 18-15B had marked weakness of the left orbicularis oculi muscle as a result of a stroke involving the facial nucleus.
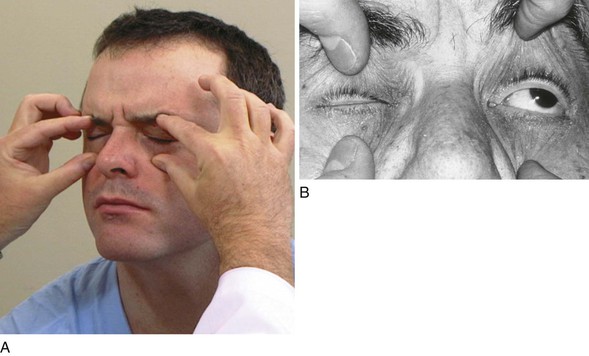
Figure 18–15 Testing the strength of eyelid closure. A, Normal response. Note that the eyelids cannot be opened by the examiner. B, Test in a patient with a stroke that involved the facial nerve nucleus. Note the loss in strength of the muscle around the left eye.
The innervations of the facial nerve are illustrated in Figure 18-16. There are two types of facial weakness. Upper motor neuron lesions such as a stroke involving the corticobulbar pathways produce contralateral weakness of the lower face, with normal function of the upper face. The patient is still able to wrinkle the forehead. This is related to the bilateral innervation of the upper face by the corticobulbar fibers. The lower face has only unilateral innervation from contralateral cortical centers. This type of upper motor neuron lesion is illustrated by lesion A in Figure 18-16. The second type of facial weakness produces total involvement of the ipsilateral facial muscles, with no area being spared. This may result from lesions of the nerve as it exits from the skull or from involvement of the facial nucleus in the pons, as illustrated by lesion B in Figure 18-16.
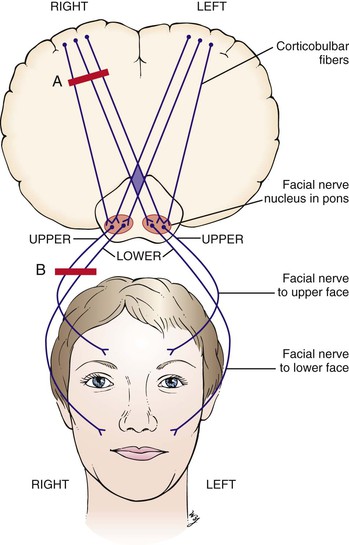
Figure 18–16 Innervations of the facial nerve and types of facial weakness. Lesion A produces an upper motor nerve palsy that causes contralateral weakness of the lower face but spares the contralateral forehead. Lesion B produces a lower motor nerve palsy that causes total paralysis of the ipsilateral face.
When the patient in Figure 18-17 was asked to smile, the right side of his face was drawn to the left. This patient has right facial palsy, also known as right Bell‘s palsy. Further maneuvers revealed that the entire right side of his face was involved as a result of a lesion affecting the right facial nucleus.
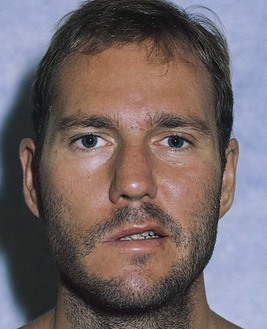
Figure 18–17 Right facial palsy.
Cranial Nerve VIII: Vestibulocochlear

The vestibulocochlear nerve is responsible for hearing, balance, and awareness of position. Auditory testing is discussed in Chapter 8, The Ear and Nose. Tests for the vestibular function of cranial nerve VIII usually are not performed.
Cranial Nerve IX: Glossopharyngeal

The glossopharyngeal nerve supplies sensation to the pharynx, posterior one third of the tongue, and tympanic membrane, as well as secretory fibers to the parotid gland.
Test Sensory Function
Examination of the glossopharyngeal nerve involves the gag reflex. The examiner may use either a tongue blade or an applicator stick. By touching the posterior third of the tongue, the soft palate, or the posterior pharyngeal wall, the examiner should elicit a gag reflex. The sensory portion of the loop is through the glossopharyngeal nerve; the motor portion is mediated through the vagus nerve.
Another way to test the nerve is to ask the patient to open the mouth widely and to say, “Ah … ah.” Symmetric elevation of the soft palate demonstrates normal function of cranial nerves IX and X. The uvula should remain in the midline.
Taste sensation of the posterior third of the tongue is not routinely tested.
Cranial Nerve X: Vagus

The vagus nerve supplies parasympathetic fibers to the viscera of the chest and abdomen; motor fibers to the pharynx and larynx; and sensory fibers to the external ear canal, the meninges of the posterior cranial fossa, the pharynx, the larynx, and the viscera of the body cavities above the pelvis.
Examination of the vagus nerve was performed during evaluation of the glossopharyngeal nerve.
Dysphonia or dysarthria may result from paralysis of the vagus nerve.
Cranial Nerve XI: Spinal Accessory

The spinal accessory nerve is a motor nerve that supplies the sternocleidomastoid and trapezius muscles.
Test Motor Function
The left spinal accessory nerve is examined by asking the patient to turn the head to the right against the resistance of the examiner’s hand. This is demonstrated in Figure 18-18. The right spinal accessory nerve is examined by reversing the directions.

Figure 18–18 Technique for evaluating the spinal accessory nerve.
An alternative test is to evaluate the trapezius muscles. The examiner places both hands on the patient’s trapezius muscles. Both muscles are palpated between the examiner’s thumbs and index fingers. The patient is then asked to shrug the shoulders against the resistance of the examiner’s hands. Both sides should move equally. This technique is demonstrated in Figure 18-19.

Cranial Nerve XII: Hypoglossal

The hypoglossal nerve supplies motor fibers to the muscles of the tongue. The examination of the hypoglossal nerve is performed by asking the patient to open the mouth, with the tongue resting quietly on the floor of the mouth. Inspection for fasciculations6 is performed. Fasciculations are indicative of a hypoglossal lower motor neuron lesion.
Test Motor Function

Ask the patient to open the mouth and stick out the tongue. Normally, the tongue is protruded and lies in the midline. This is demonstrated in Figure 18-20. Deviation of the tongue to either side is abnormal. Because the tongue muscles push rather than pull, weakness of one side results in the tongue’s being pushed by the normal side to the side of the lesion.

Figure 18–20 Technique for evaluating the hypoglossal nerve.
In Figure 18-21, notice the marked scalloping of the tongue’s surface. The patient has a chronic neurologic disease known as amyotrophic lateral sclerosis7 characterized by progressive degeneration of motor neurons. The patient has the typical features of a lower motor neuron bulbar palsy affecting the hypoglossal nucleus: wasting of the tongue with fasciculations.

Motor Function
Basic Principles
The motor system is evaluated for the following:
The motor examination begins with inspection of each area being tested. The contours of symmetric muscle masses in both the upper and lower extremities are compared. Inspection is used to detect muscle atrophy and the presence of fasciculations.
Test muscle strength by having the patient move actively against your resistance. Compare one side with the other. The following is an arbitrary scale that is commonly used for the grading of muscle strength:
0, Absent: No contraction detected
1, Trace: Slight contraction detected
2, Weak: Movement with gravity eliminated (sideways)
3, Fair: Movement against gravity (upward)
If muscle weakness is found, compare the proximal and distal strengths. In general, proximal weakness is related to muscle disease; distal weakness is related to neurologic disease.
Tone can be defined as the slight residual tension in a voluntarily relaxed muscle. Tone is assessed by resistance to passive movement. Ask the patient to relax. Perform passive motion of the muscle. Compare one side with the other. Upper motor neuron lesions produce spasticity,8 hyperreflexia, clonus,9 and Babinski’s sign.10
Lower motor neuron lesions produce atrophy, fasciculations, decreased tone, and hyporeflexia. Both types of lesions result in weakness. Fasciculations may become more apparent by gently tapping the muscle with a reflex hammer.
It is impractical to test all muscles during the neurologic examination. By testing key muscle groups, the examiner can determine whether a gross deficit exists. Further testing of specific muscles and nerve roots may then be necessary. The student is referred to the many textbooks on neurology for these detailed examinations.
Examine Upper Extremities
In the assessment of motor function, the upper extremities are examined first.
Inspect the Upper Extremities for Symmetry
Ask the patient to sit on the side of the bed facing you. Inspect both arms and hands for size differences, paying special attention to the size of the thumbs and the small muscles of the hands. Is muscle wasting present?
Test Flexion and Extension of the Arm
Test flexion and extension strength of the upper extremity by having the patient pull and push against your resistance. You might say, “Push down … relax,” “Push up … relax,” “Push back … relax,” and “Push forward … relax.” Say “relax” after each direction so that the patient does not continue to push or pull after you have removed your hands. After one side is tested, the other is tested, and the results of the two sides are compared.
Test Arm Abduction
Ask the patient to extend the arms, with palms facing down. Place your hands at the lateral aspect of the patient’s arms. Instruct the patient to abduct the arms against resistance. This is a test of abduction of the arm by the axillary nerve from roots C5 to C6. This test is demonstrated in Figure 18-22.

Figure 18–22 Technique for testing abduction of the arm.
Test Forearm Flexion
Have the patient make a fist and flex the forearm. Hold the patient’s fist or wrist. Ask the patient to pull the arm in against your resistance. This is a test of flexion of the forearm by the musculocutaneous nerve from roots C5 to C6. This test is demonstrated in Figure 18-23.

Figure 18–23 Technique for testing flexion of the forearm.
Test Forearm Extension
Ask the patient to abduct the arm and hold it midway between flexion and extension. Support the patient’s arm by holding the wrist. Instruct the patient to extend the arm against your resistance. This is a test of extension of the forearm by the radial nerve from roots C6 to C8. This test is demonstrated in Figure 18-24.

Figure 18–24 Technique for testing extension of the forearm.
Test Wrist Extension
Instruct the patient to make a fist and extend the wrist while you attempt to push it up. This is a test of extension of the wrist by the radial nerve from roots C6 to C8. This test is demonstrated in Figure 18-25.

Figure 18–25 Technique for testing extension of the wrist.
Test Wrist Flexion
Ask the patient to make a fist and flex the wrist while you attempt to pull it down. This is a test of flexion of the wrist by the median nerve from roots C6 to C7. This test is demonstrated in Figure 18-26.

Figure 18–26 Technique for testing flexion of the wrist.
Test Finger Adduction
Ask the patient to grasp your extended index and middle fingers and to squeeze them as hard as possible. Compare the strengths of both hands. (It is important for you to remove any rings, which may produce discomfort.) This is a test of adduction of the fingers by the median nerve from roots C7 to T1. This test is demonstrated in Figure 18-27.

Figure 18–27 Technique for testing finger adduction.
Test Finger Abduction
Ask the patient to extend the hand with the palm down and to spread the fingers as widely as possible. Tell the patient to resist your attempt to bring the fingers together. This is a test of abduction of the fingers by the ulnar nerve from roots C8 to T1. This test is demonstrated in Figure 18-28.

Figure 18–28 Technique for testing finger abduction.
Test Thumb Adduction
Instruct the patient to touch the base of the little finger with the tip of the thumb against resistance while the thumbnail remains parallel to the palm. This is a test of adduction of the thumb by the median nerve from roots C8 to T1. This test is demonstrated in Figure 18-29.

Figure 18–29 Technique for testing thumb adduction.
Assess Upper Extremity Tone
Tone is assessed in the patient’s upper limbs by passively flexing and extending the limbs to determine the amount of resistance to the examiner’s movements. Increased resistance, such as that in muscle rigidity or spasticity, means increased muscle tone. Decreased resistance, such as that in limpness or flaccidity, means decreased muscle tone. Normal tone has a smooth sensation. In extrapyramidal disease, palpation of a proximal muscle during passive movement detects the presence of cogwheeling, which is a ratchety jerkiness to the motion.
Examine Lower Extremities
Inspect the Lower Extremities for Symmetry
The lower extremities are now examined for muscle bulk and muscle wasting. This examination is performed with the patient lying on his or her back in bed. As with the upper extremities, proximal and distal muscle strengths are compared, as are the legs with regard to symmetry.
Test Hip Adduction
Ask the patient to move the legs apart. Place your hands on the medial aspect of the patient’s knees. Instruct the patient to close the legs against your resistance. This is a test of adduction of the hips by the obturator nerve from roots L2 to L4. This test is demonstrated in Figure 18-30.

Figure 18–30 Technique for testing hip adduction.
Test Hip Abduction
Place your hands on the lateral margins of the patient’s knees. Ask the patient to open the legs against your resistance. This is a test of abduction of the hips by the superior gluteal nerve from roots L4 to S1. This test is demonstrated in Figure 18-31.

Figure 18–31 Technique for testing hip abduction.
Test Knee Flexion
Ask the patient to elevate a knee, with the foot resting on the bed. Instruct the patient to hold the foot down as you try to extend the leg. This is a test of flexion of the knee by the sciatic nerve from roots L4 to S1. This test is illustrated in Figure 18-32.

Figure 18–32 Technique for testing knee flexion.
Test Knee Extension
Instruct the patient to elevate the knee, with the foot resting on the bed. Place your left hand under the knee. Ask the patient to straighten the leg against the resistance of your right hand, which is placed on the patient’s shin. This procedure tests extension of the knee by the femoral nerve from roots L2 to L4. This test is illustrated in Figure 18-33.

Figure 18–33 Technique for testing knee extension.
Test Ankle Dorsiflexion
Place your hands on the dorsum of the foot, and ask the patient to dorsiflex the foot at the ankle against your resistance. This is a test of dorsiflexion of the ankle by the deep peroneal nerve from roots L4 to L5. This maneuver is demonstrated in Figure 18-34.

Figure 18–34 Technique for testing ankle dorsiflexion.
Test Ankle Plantar Flexion
Place your hand on the sole, and ask the patient to plantarflex the foot at the ankle against your resistance. This is a test of plantar flexion of the ankle by the tibial nerve from roots L5 to S2. This test is demonstrated in Figure 18-35.

Figure 18–35 Technique for testing plantar flexion.
Test Great Toe Dorsiflexion
Place your hand on the dorsal aspect of the patient’s big toe. Ask the patient to dorsiflex the big toe against your resistance. This is a test of dorsiflexion of the big toe by the deep peroneal nerve from roots L4 to S1. This test is demonstrated in Figure 18-36.

Figure 18–36 Technique for testing great toe dorsiflexion.
Test Great Toe Plantar Flexion
Place your hand on the plantar surface of the patient’s big toe. Ask the patient to plantarflex the great toe against your resistance. This is a test of plantar flexion of the great toe by the posterior tibial nerve from roots L5 to S2. This test is demonstrated in Figure 18-37.

Figure 18–37 Technique for testing great toe plantar flexion.
Assess Lower Extremity Tone
Tone in the lower extremities is assessed in the same way as in the upper extremities.
Grasp the foot and passively dorsiflex and plantarflex it several times, ending with dorsiflexion of the foot. If a sudden rhythmic involuntary dorsiflexion and plantar flexion occur, ankle clonus is present. This frequently occurs in conditions of increased tone.
If any abnormality is noted in the motor strength of the upper or lower extremity, a more detailed examination should be performed. See Table 18-7 for a list of the muscle innervations and their actions.
Reflexes
Basic Principles
Two main types of reflexes are tested. They are the stretch, or deep tendon, reflexes and the superficial reflexes.
There is individual variation in the reflex response. Only with experience is the examiner able to make an adequate assessment of normal reflexes. Reflexes are commonly graded on a scale from 0 to 4+ as follows:
Hyperactive reflexes are characteristic of pyramidal tract disease. Electrolyte abnormalities, hyperthyroidism, and other metabolic abnormalities may be the cause of hyperactive reflexes. Diminished reflexes are characteristic of anterior horn cell disorders and myopathies. The examiner should always consider the strength of the reflex in relation to the bulk of the muscle mass. A patient may have diminished reflexes as a result of a decrease in muscle bulk. Patients with hypothyroidism have decreased relaxation after a deep tendon reflex, which is termed a hung reflex.
In a patient with a diminished reflex, the technique of reinforcement may be useful. If the patient performs isometric contraction of other muscles, the generalized reflex activity may be increased. When testing reflexes in the upper extremities, have the patient clench the teeth or push down on the bed with the thighs. When testing reflexes in the lower extremities, have the patient lock fingers and try to pull them apart at the time of testing. This procedure, sometimes called Jendrassik‘s maneuver, is demonstrated in Figure 18-38.

Figure 18–38 Jendrassik’s maneuver.
Test the Deep Tendon Reflexes
The deep tendon reflexes that are routinely tested are as follows:
Test the Biceps Tendon Reflex

The biceps tendon reflex is assessed by having the patient relax the arm and pronate the forearm midway between flexion and extension. The examiner should place a thumb firmly on the biceps tendon. The hammer is then struck on the examiner’s thumb. This is demonstrated in Figure 18-39. The examiner should observe for contraction of the biceps tendon, followed by flexion at the elbow. The examiner may also palpate the contraction of the muscle. This procedure is a test of the nerves at roots C5 to C6.

Figure 18–39 Technique for testing the biceps tendon reflex.
Test the Brachioradialis Tendon Reflex

The brachioradialis tendon reflex is performed by having the patient’s forearm in semiflexion and semipronation. The arm should be rested on the patient’s knee. If a triangular reflex hammer is used, the wide end should strike the styloid process of the radius approximately 2.5 to 5 cm above the wrist. The examiner should observe for flexion at the elbow and simultaneous supination of the forearm. The position is demonstrated in Figure 18-40. This procedure is a test of the nerves at roots C5 to C6.

Test the Triceps Tendon Reflex

The triceps tendon reflex is tested by flexing the patient’s forearm at the elbow and pulling the arm toward the chest. The elbow should be midway between flexion and extension. Tap the triceps tendon above the insertion of the ulna’s olecranon process approximately 2.5 to 5 cm above the elbow. There should be a prompt contraction of the triceps tendon with extension at the elbow. This technique is demonstrated in Figure 18-41. This procedure is a test of the nerves at roots C6 to C8.

Figure 18–41 Technique for testing the triceps tendon reflex.
If the triceps tendon reflex cannot be elicited by this maneuver, try to hang the patient’s arm over your arm, as demonstrated in Figure 18-42. Tapping the triceps tendon in this position often elicits the reflex.

Figure 18–42 Another test of the triceps tendon reflex.
Test the Patellar Tendon Reflex

Perform the patellar tendon reflex, also known as the knee jerk, by having the patient sit with his or her legs dangling off the side of the bed. Place your hand on the patient’s quadriceps muscle. Strike the patellar tendon firmly with the base of the reflex hammer. A contraction of the quadriceps should be felt, and extension at the knee should be observed. This technique is demonstrated in Figure 18-43. It is a test of the nerves at roots L2 to L4.

Figure 18–43 Technique for testing the patellar tendon reflex.
Test the Achilles Tendon Reflex

The Achilles tendon reflex, also known as the ankle jerk, is elicited by having the patient sit with his or her feet dangling off the side of the bed. The leg should be flexed at the hip and the knee. The examiner places a hand under the patient’s foot to dorsiflex the ankle. The Achilles tendon is struck just above its insertion on the posterior aspect of the calcaneus with the wide end of the reflex hammer. The result is plantar flexion at the ankle. This technique is demonstrated in Figure 18-44. It is a test of the nerves at roots S1 to S2.

Figure 18–44 Technique for testing the Achilles tendon reflex.
Another method of testing for the Achilles reflex is to have the patient lie in bed. Flex one of the patient’s legs at the hip and knee, and rotate the leg externally so that it lies on the opposite shin. Dorsiflex the ankle as the tendon is struck. This test is demonstrated in Figure 18-45A.
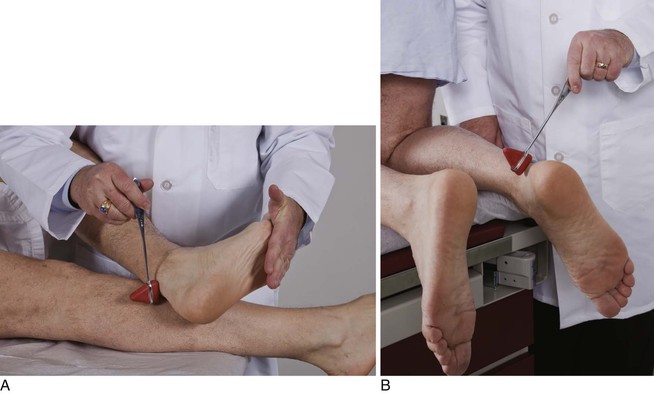
Figure 18–45 A, Alternative technique for evaluating the Achilles tendon reflex. B, Technique for assessing the Achilles tendon reflex when the reflex appears to be depressed.
A patient with a depressed Achilles reflex should be asked to kneel, if possible, on the bed with the feet hanging off the side, as shown in Figure 18-45B. Tap the Achilles tendon, and observe the reflex response in this position.
Test the Superficial Reflexes
The most commonly tested superficial reflexes are the abdominal and the cremasteric. The abdominal superficial reflex is elicited by having the patient lie on his or her back. An applicator stick or tongue blade is quickly stroked horizontally laterally to medially toward the umbilicus. The result is a contraction of the abdominal muscles, with the umbilicus deviating toward the stimulus. The abdominal reflex is frequently not seen in obese individuals. The cremasteric superficial reflex in men is elicited by lightly stroking the inner aspect of the thigh with an applicator stick or tongue depressor. The result is a rapid elevation of the testicle on the same side. Although the superficial reflexes are absent on the side of a corticospinal tract lesion, there is little clinical significance to their presence or absence. They are described here for completeness only.
Test for Abnormal Reflexes

Babinski‘s sign or reflex is a pathologic reflex. Normally, when the lateral aspect of the sole is stroked from the heel to the ball of the foot and curved medially across the heads of the metatarsal bones, there is plantar flexion of the big toe. This is a test of the nerve roots at L5 to S2. The foot should be stroked with a stimulus such as a key. A pin should never be used. In the presence of pyramidal tract disease, when the described movement is performed, there is dorsiflexion of the big toe, with fanning of the other toes. This is Babinski’s reflex. Because Babinski’s sign is an abnormal reflex, the clinician should note it only when it is present. It is correct to describe the plantar reflex as either plantar flexion (normal) or dorsiflexion (abnormal, Babinski’s). The technique for evaluating the plantar reflex is shown in Figure 18-46.
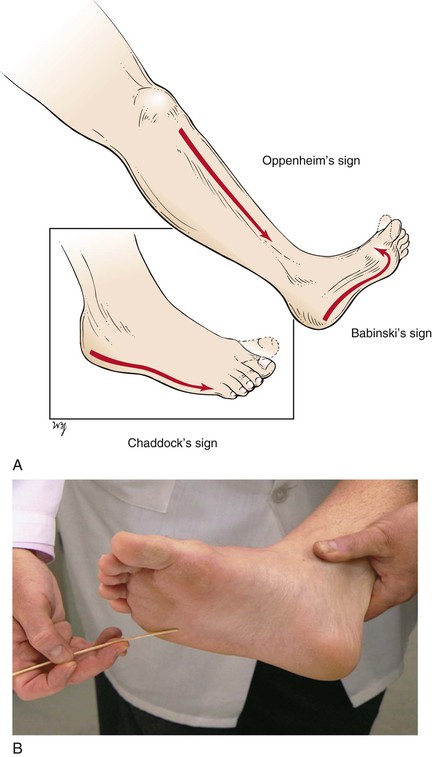
Pyramidal tract disease is also suggested when the big toe dorsiflexes on stroking the lateral aspect of the foot. This is Chaddock‘s sign. In the presence of pyramidal tract disease, downward pressure along the shin also causes the big toe to dorsiflex. This is Oppenheim‘s sign. The elicitation of these signs is less sensitive than stroking the plantar surface.
Another abnormal reflex associated with pyramidal tract disease is Hoffmann‘s sign. To elicit this sign, the patient’s hand is pronated, and the examiner grasps the terminal phalanx of the middle finger between the index finger and thumb. With a sharp jerk, the phalanx is passively flexed and suddenly released. A positive response consists of adduction and flexion of the thumb as well as flexion of the other fingers.
Sensory Function
Basic Principles
The sensory examination consists of testing for the following:
As with the motor examination, the examiner compares side with side and proximal with distal aspect. Neurologic disorders usually result in a sensory loss that is first seen more distally than proximally.
The hand is supplied by the median, ulnar, and radial nerves. The median nerve is the chief nerve of sensation because it supplies the palmar surfaces of the digits, the parts of the hand most commonly used for feeling. The ulnar nerve supplies sensation only to the ulnar one and a half fingers. The radial nerve has its sensory distribution to the dorsum of the hand. There is considerable overlap in innervation. The most reliable cutaneous areas for testing these nerves are illustrated in Figure 18-47. These areas have the least likelihood of overlapping innervation.
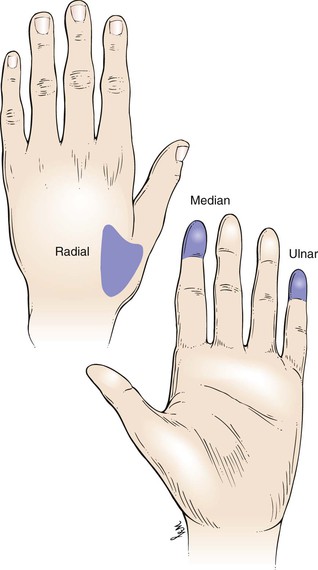
Test Light Touch

Light touch is evaluated by lightly touching the patient with a small piece of gauze. Ask the patient to close his or her eyes and to tell you when the touch is felt. Try touching the patient on the toes and fingers. This is demonstrated in Figure 18-48. If sensation is normal, continue with the next test. If sensation is abnormal, work proximally until a sensory level can be determined. A sensory level is a spinal cord level below which there is a marked decrease in sensation. Figure 18-49 illustrates the segmental distribution of the spinal nerves that transmit sensation to the spinal cord.

Figure 18–48 Technique for testing light touch.
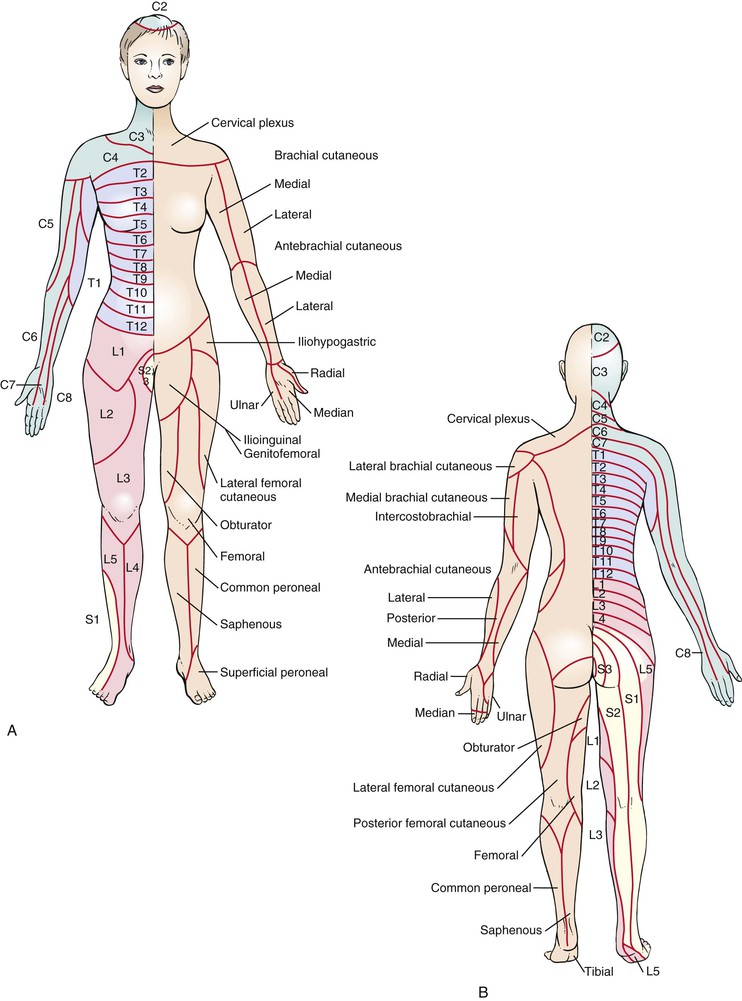
Test Pain Sensation

Pain sensation is tested by using a safety pin and asking the patient if it is felt. Ask the patient to close his or her eyes. Open the safety pin and touch the patient with its tip. Tell the patient, “This is sharp.” Now touch the patient with the blunt end of the pin and say, “This is dull.” This is demonstrated in Figure 18-50. Start testing pain sensation on the toes and fingers and say, “What is this, sharp or dull?” If the patient has no loss of sensation, proceed with the next examination. If there is a sensory loss to pain, continue proximally to determine the sensory level. A new pin should be used for each patient. Instead of using a pin, you can use a wooden applicator stick that has been broken. Use the broken end for sharp testing and the cotton tip for dull testing as illustrated in Figure 18-51.
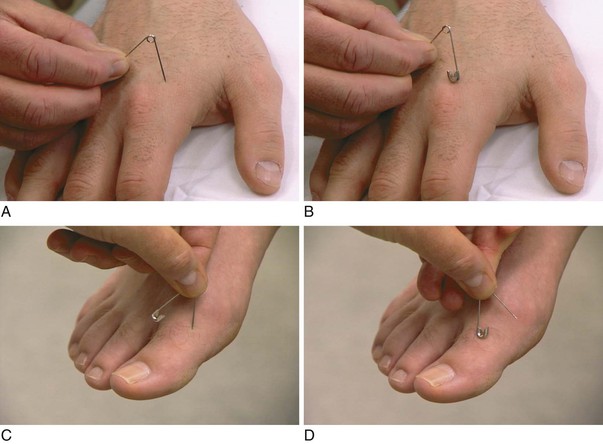
Figure 18–50 Technique for testing pain sensation. A and C, The examiner should hold the pin as demonstrated and say, “This is sharp.” B and in D, The examiner should hold the other end of the pin and say “This is dull.”
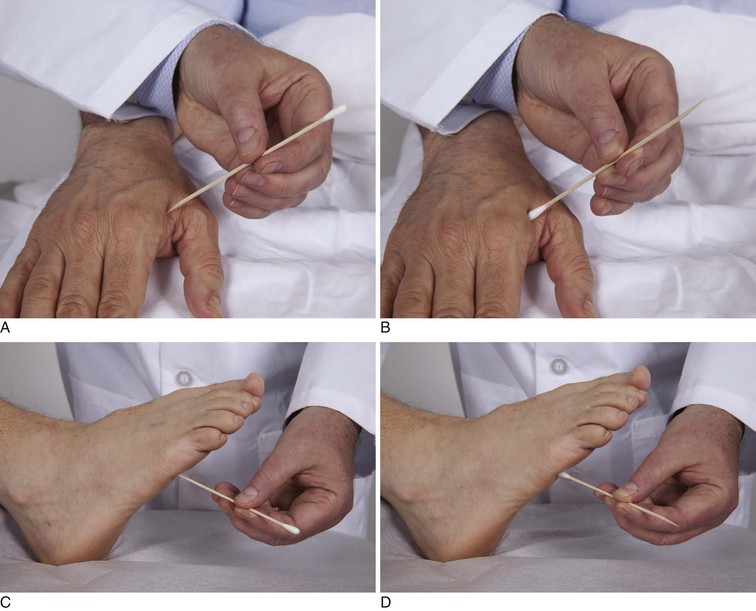
Figure 18–51 An alternate, and better, technique for testing pain sensation using a broken applicator stick. A and C, The examiner should hold the broken end of the applicator and say, “This is sharp.” B and D, The examiner should hold the cotton tip end of the applicator stick and say “This is dull.”
Test Vibration Sense

Vibration sense is tested using a 128-Hz tuning fork. Tap the tuning fork on the heel of your hand and place it on the patient on a bony prominence distally. Instruct the patient to inform you when the vibration is no longer felt. Ask the patient to close his or her eyes. Place the vibrating tuning fork over the distal phalanx of the patient’s finger with your own finger under the patient’s finger, as demonstrated in Figure 18-52A. In this manner, you will be able to feel the vibration through the patient’s finger to determine the accuracy of the patient’s response. After the fingers are tested, test the big toes, as demonstrated in Figure 18-52B. If there is no loss of vibration sense, proceed with the next examination. If a loss is present, determine the level.
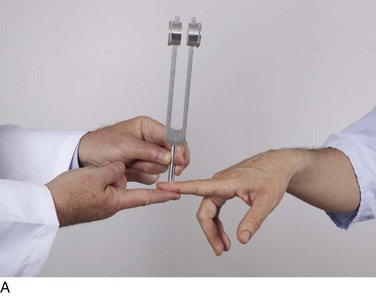
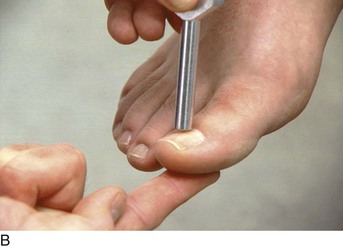
Test Proprioception

Position sense, or proprioception, is tested by moving the distal phalanx. Hold the distal phalanx at its lateral aspects, and move the digit up while telling the patient, “This is up.” Move the distal phalanx down and tell the patient, “This is down.” With the patient’s eyes closed, move the distal phalanx up and down and finally stop and ask, “What is this, up or down?” This is demonstrated in Figure 18-53A. Grasp only the sides of the digit so that the patient cannot be clued by the pressure exerted on the digit. It is routine to test the terminal phalanx of a finger on each hand and the terminal phalanx of the toes (see Fig. 18-53B). If no loss of position sense is detected, continue with the rest of the examination. A loss of proprioception necessitates further evaluation to determine the level of loss.
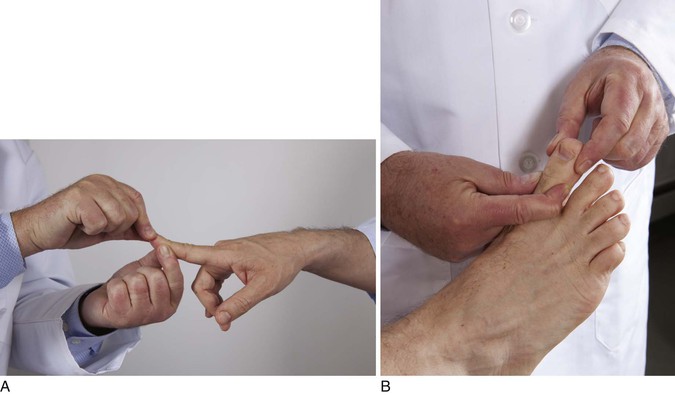
Test Tactile Localization
Tactile localization, also known as double simultaneous stimulation, is assessed by having the patient close his or her eyes and identify where your touch was felt. Touch the patient on the right cheek and the left arm. The patient is then asked, “Where did I touch you?” This is demonstrated in Figure 18-54. Normally, patients have no problem identifying both areas. A patient with a lesion in the parietal lobe may feel the individual touches but may “extinguish” the sensation on the side contralateral to the side of the lesion. This is the phenomenon termed extinction.

Figure 18–54 Technique for testing tactile localization.
Test Two-Point Discrimination
Two-point discrimination tests the patient’s ability to differentiate one stimulus from two. Gently hold two pins 2 to 3 mm apart, and touch the patient’s fingertip. Ask the patient to state the number of pins felt. This is demonstrated in Figure 18-55. Compare this finding with that from the corresponding area on a fingertip of the other hand. Because different areas of the body have different sensitivities, you must know these differences. At the fingertips, two-point discrimination is 2 mm apart. The tongue can discriminate two objects 1 mm apart; the toes, 3 to 8 mm apart; the palms, 8 to 12 mm apart; and the back, 40 to 60 mm apart. A lesion in the parietal lobe impairs two-point discrimination.

Figure 18–55 Technique for testing two-point discrimination.
Test Stereognosis
Stereognosis is the integrative function of the parietal and occipital lobes. It is tested by having the patient attempt to identify an object placed in the hands. Have the patient close his or her eyes. Place a key, pencil, paper clip, or coin in the palm of the patient’s hand, and ask what it is. Test the other hand and compare the findings.
Test Graphesthesia
Graphesthesia is the ability to identify a number “written” in the palm of one’s hand. Ask the patient to close his or her eyes and extend the hand. Use the blunt end of a pencil to “write” numbers from 0 to 9 in the palm. The numbers should be oriented facing the patient. This is demonstrated in Figure 18-56. Normally, the patient should be able to identify the numbers. Compare one hand with the other. The inability to identify the numbers is a sensitive sign of parietal lobe disease.

Figure 18–56 Technique for testing graphesthesia.
Test Point Localization
Point localization is the ability of a person to point to an area where he or she was touched. Have the patient close his or her eyes. Touch the patient. Ask the patient to open the eyes and point to the area touched. Abnormalities of the sensory cortex impair the ability to localize the area touched.
Cerebellar Function
Cerebellar function is tested by the following:
Perform the Finger-to-Nose Test

The finger-to-nose test is performed by asking the patient to touch his or her own nose and the examiner’s finger alternately as quickly, accurately, and smoothly as possible. The examiner holds a finger at arm’s length from the patient. The patient is instructed to touch the finger and then the nose. This is repeated several times, after which the patient is asked to perform the test with eyes closed. This is demonstrated in Figure 18-57. Patients with cerebellar disease persistently overshoot the target, a condition known as past pointing. They may also have a tremor as the finger approaches the target.
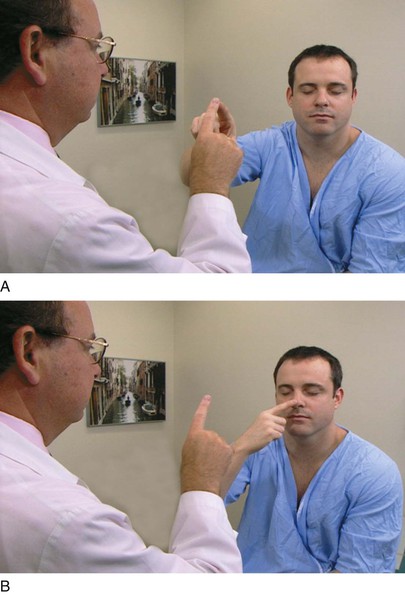
Figure 18–57 A and B, Finger-to-nose test.
Perform the Heel-to-Knee Test
The heel-to-knee test is performed by having the patient lie on his or her back. The patient is instructed to slide the heel of one lower extremity down the shin of the other, starting at the knee. This is demonstrated in Figure 18-58. A smooth movement should be seen, with the heel staying on the shin. In patients with cerebellar disease, the heel wobbles from side to side.

Figure 18–58 Heel-to-knee test.
Assess Rapid Alternating Movements
The ability to perform rapid alternating movements is called diadochokinesia. These motions may be tested in the upper extremity or the lower extremity. The patient can be asked to pronate and supinate one hand on the other hand rapidly. Another technique involves having the patient touch the thumb to each finger as quickly as possible. The patient may also be asked to slap the thigh, raise the hand, turn it over, and slap the thigh again rapidly. This pattern is repeated over and over as quickly as possible. These techniques are illustrated in Figure 18-59. An abnormality in performing rapid alternating movements is called adiadochokinesia.
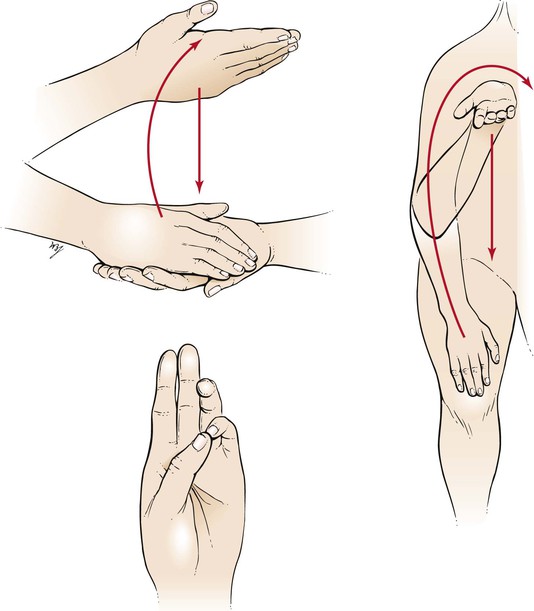
Figure 18–59 Techniques for testing rapid alternating movements.
Perform Romberg Test

The Romberg test is performed by having the patient stand in front of the examiner with feet together so that the heels and toes are touching. The examiner instructs the patient to extend the arms with palms facing upward and to close the eyes. If the patient can maintain this posture without moving, the test result is negative. The result is positive if the patient begins to sway and has to move the feet for balance. Another common finding is for one of the arms to drift downward, with flexion of the fingers. This is called pronator drift and is seen in patients with mild hemiparesis. The Romberg test is used to examine the posterior columns rather than actual cerebellar function. The examiner should be at the patient’s side during this test because an occasional patient may suddenly sway and fall if assistance is not provided.
Assess Gait

Foremost in the examination of cerebellar function is the observation of gait. The patient is asked to walk straight ahead while the examiner observes the gait. The patient is then instructed to return on tiptoes; to walk away again on the heels; and to return to the examiner by walking in tandem gait: one foot placed in front of the other, the heel of one foot touching the toes of the other on each step. The examiner may need to demonstrate this gait for the patient. The patient should have normal posture, and there should be normal associated movements of the arms. The examiner should pay special attention to the way in which the patient turns around. These maneuvers often accentuate cerebellar ataxia, as well as indicate weakness in the lower extremities (see Figure 17-23).
Many neurologic disorders produce striking and characteristic gaits. A patient with hemiplegia tends to drag or circumduct a weak and spastic leg. The arm is frequently flexed at the elbow across the abdomen as the patient walks. A patient with Parkinson‘s disease shuffles, with short, hurried steps. The head is bowed, with the back bent over. A patient with cerebellar ataxia walks with a wide-based gait. The feet are very far apart as the patient staggers from side to side. A patient with footdrop has a characteristic slapping gait resulting from weakness of the dorsiflexors of the ankle. A patient with sensory ataxia has a high-stepping gait in which the feet are slapped down firmly, as if the person is unsure of the foot’s location. Figure 18-60 illustrates these gaits.
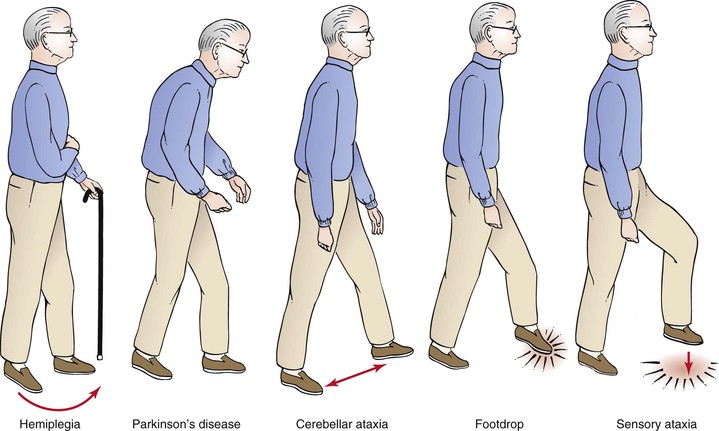
Figure 18–60 Common types of gait abnormalities.
Clinicopathologic Correlations
The Comatose Patient
Coma is the state in which the patient is unable to respond to any stimuli. The causes of coma include the following:
If the patient’s friends or family members are available, speak with them. They can help in the evaluation of the patient by giving valuable information. Is there a history of hypertension, diabetes, epilepsy, substance abuse, or recent head trauma?
If there is any evidence of head trauma, radiographs of the cervical spine must be taken before the examiner moves the patient’s neck.
The physical examination of the comatose patient should start with inspection. The clothing, age, and evidence of chronic illness provide valuable clues as to the cause of the coma. Does the patient have gingival enlargement consistent with antiepileptic medical therapy?12
Is there a characteristic odor to the breath? The sweet smell of ketones may be present in diabetic ketoacidosis. An odor of alcohol may be present. Are there stigmata of chronic liver disease?
What is the posture of the patient? Patients with cerebral hemispheric dysfunction or a destructive lesion of the pyramidal tracts maintain a decorticate posture, whereas those patients with a midbrain or pons lesion maintain a decerebrate posture. In decorticate rigidity, the arms are adducted and the elbows, wrists, and fingers are flexed. The legs are internally rotated. In decerebrate rigidity, the arms are also adducted but they are rigidly extended at the elbows, and the forearms are pronated. The wrists and fingers are flexed. In both postures, the feet are plantarflexed. The positions of the arms and hands are shown in Figure 18-61.
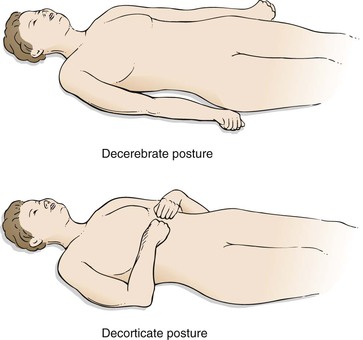
Figure 18–61 Postures of comatose patients.
The respiratory pattern should be evaluated. Central neurogenic hyperventilation is seen in lesions of the midbrain or pons. This type of respiration consists of rapid, deep, regular breathing. Cheyne-Stokes breathing is characterized by rhythmic changes in the breathing pattern. Periods of rapid breathing are separated by periods of apnea. Cheyne-Stokes breathing is associated with brainstem compression or bilateral cerebral dysfunction.
The neurologic examination of the comatose patient is largely based on pupillary size and light reflexes. The pupils are small and reactive in bilateral cerebral dysfunction. They are dilated after an overdose of hallucinogenic agents or central nervous system stimulants. A unilateral fixed and dilated pupil is suggestive of pressure on the ipsilateral oculomotor nerve. Pupillary dilatation precedes paralysis of the extraocular muscles; this is because the pupillary nerve fibers are superficial to the fibers innervating the extraocular muscles and are more vulnerable to extrinsic stresses. This is an important sign of uncal herniation. In the presence of normally reactive pupils with absence of corneal reflexes and absence of extraocular movement, a metabolic abnormality may be the cause of the coma.
The fundus of the eye may provide a clue as to the cause of the coma.
If there is no evidence of a fracture of the cervical spine, oculocephalic reflexes should be tested. If a comatose patient’s head is rapidly turned to one side while the eyelids are held open, the eyes should move conjugately to the other side. This is the doll‘s eyes reflex. In a patient with a lesion in the brain stem, the doll’s eyes reflex is absent. The doll’s eyes reflex can be elicited only in a comatose patient because alert individuals fixate on an object and override this reflex.
Caloric stimulation is used to enhance the doll’s eyes reflex or to test movements in an individual with a fractured cervical spine. The patient should be placed with the head flexed at 30 degrees. This orients the semicircular canal in a horizontal position. A large-bore syringe is filled with 20 to 30 mL of ice water, and the water is squeezed into one of the external auditory canals. The normal response is the development of nystagmus. Slowly the eyes move conjugately to the ipsilateral side and then move rapidly (nystagmus) back to the midline. The use of cold water causes nystagmus to the opposite side. If warm water is used, the eyes move rapidly toward the side being irrigated. This can easily be remembered by using the mnemonic COWS, which stands for “cold opposite, warm same.”
An absence of the caloric response is seen in patients with a disruption of the connections between the vestibular nuclei and the sixth cranial nerve nucleus at the level of the brain stem.
As was indicated earlier in the chapter, headache is an important symptom of neurologic disease. Table 18-2 provides a differential diagnosis of headaches.
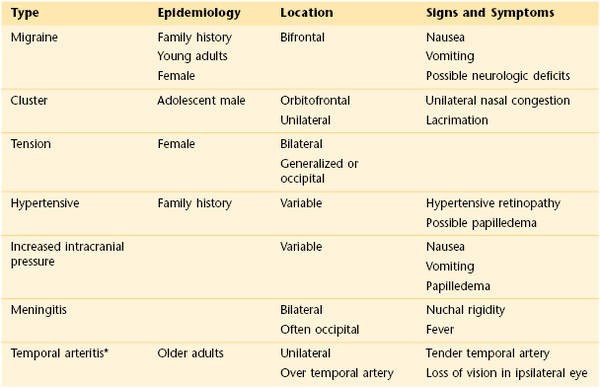
The correct assessment of a patient’s motor activity can help localize the site of a lesion. The term extrapyramidal refers to those parts of the motor system that are not directly involved with the pyramidal tracts. The extrapyramidal system is composed of the basal ganglia, nuclei of the midbrain and reticular formation, and cerebellum. Table 18-3 lists the major areas and the specific motor problems associated with lesions of the lower motor neuron, the pyramidal tract, and the extrapyramidal tract. Table 18-4 summarizes the important signs and symptoms in five common chronic neurologic disorders.
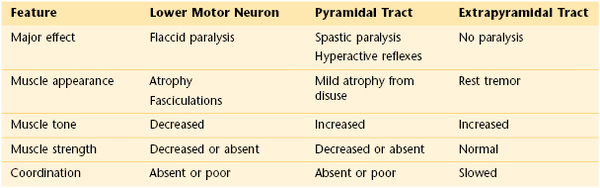
Table 18–4
Common Neurologic Conditions and Their Signs and Symptoms
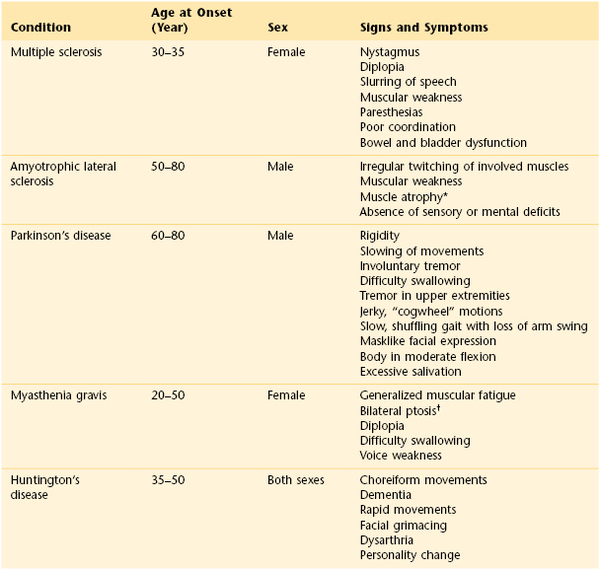
* See Figure 18-21.
† See Figure 7-16.
A comparison of the effects of upper and lower motor neuron lesions is shown in Table 18-5.
Table 18–5
Comparison of Effects of Upper and Lower Motor Neuron Lesions
| Effect | Upper Motor Neuron Lesion | Lower Motor Neuron Lesion |
| Voluntary control | Lost | Lost |
| Muscle tone | Spastic, increased | Flaccid, decreased |
| Reflex arcs | Present | Absent |
| Pathologic reflexes | Present | Not present |
| Muscle atrophy | Little or none | Significant |
Paraplegia and quadriplegia are upper motor neuron defects. They can also involve lower motor neurons. Injury of the spinal cord can produce partial or complete paralysis. In patients with cervical or thoracic lesions, spasticity is present below the level of the lesion, and flaccidity is present in all muscles supplied from reflex arcs at the level of the lesion. In the presence of sacral lesions, a flaccid paralysis results. Table 18-6 summarizes motor involvement in spinal cord lesions.
Table 18–6
Motor Involvement in Spinal Cord Lesions
| Affected Cord Segment | Motor Involvement |
| C1–C4 | Paralysis of neck, diaphragm, intercostals, and all four extremities |
| C5 | Spastic paralysis of trunk, arms, and legs; partial shoulder control |
| C6, C7 | Spastic paralysis of trunk and legs; upper arm control; partial lower arm control |
| C8 | Spastic paralysis of trunk and legs; hand weakness only |
| T1–T10 | Spastic paralysis of trunk and legs |
| T11–T12 | Spastic paralysis of legs |
| L1–S1 | Flaccid paralysis of legs |
| S2–S5 | Flaccid paralysis of lower legs; bowel, bladder, and sexual function affected |
Often a patient may complain of a decreased ability to perform a task. Physical examination may reveal decreased motor strength. Table 18-7 summarizes the major actions of the more common muscles and their corresponding cord segments.
Table 18–7
Motor Function According to Cord Segments
| Area of Body | Action Tested | Cord Segment |
| Shoulder | Flexion, extension, or rotation of neck | C1–C4 |
| Arm | Adduction of arm | C5–T1 |
| Abduction of arm | C4–C6 | |
| Flexion of forearm | C5–C6 | |
| Extension of forearm | C6–C8 | |
| Supination of forearm | C5–C7 | |
| Pronation of forearm | C6–C7 | |
| Hand | Extension of hand | C6–C8 |
| Flexion of hand | C7–C8, T1 | |
| Finger | Abduction of thumb | C7–C8, T1 |
| Adduction of thumb | C8, T1 | |
| Abduction of little finger | C8, T1 | |
| Opposition of thumb | C8, T1 | |
| Hip | Flexion of hip | L1–L3 |
| Extension of leg | L2–L4 | |
| Flexion of leg | L4–L5, S1–S2 | |
| Adduction of thigh | L2–L4 | |
| Abduction of thigh | L4–L5, S1–S2 | |
| Medial rotation of thigh | L4–L5, S1 | |
| Lateral rotation of thigh | L4–L5, S1–S2 | |
| Flexion of thigh | L4–L5 | |
| Foot | Dorsiflexion of foot | L4–L5, S1 |
| Plantar flexion of foot | L5, S1–S2 | |
| Toe | Extension of great toe | L4–L5, S1 |
| Flexion of great toe | L5, S1–S2 | |
| Spreading of toes | S1–S2 |
The bibliography for this chapter is available at studentconsult.com.
Useful Vocabulary
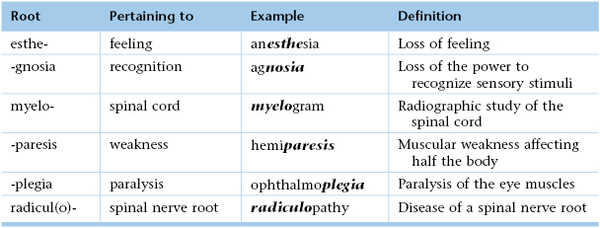
Bibliography
American Psychiatric Association. DSM-5 revisions for personality disorders reflect major change. [Available at] http://www.dsm5.org/Newsroom/Documents/DSM-5-Revisions-for-Personality-Disorders-Reflect-Major-Change.pdf; July 7, 2011 [Accessed January 29, 2013] .
Blass DM, Rabins DV. In the clinic: dementia. Ann Intern Med. 2008;148.
Boulton AJ, et al. Diabetic neuropathies. A statement by the American Diabetes Association. Diabetes Care. 2005;28:956.
Centers for Disease Control and Prevention. Suicide facts at a glance. [Available at] http://www.cdc.gov/ViolencePrevention/pdf/Suicide_DataSheet-a.pdf; Summer 2010 [Accessed January 28, 2013] .
Chan Y. Differential diagnosis of dizziness. Curr Opin Otolaryngol Head Neck Surg. 2009;17:200.
Cuccharia G, Kasner SE. In the clinic: transient ischemic attack. Ann Intern Med. 2011;154.
Davenport R. Diagnosing acute headache. Clin Med. 2004;4:108.
Diener HC, Limmroth V. Medication-overuse headache: a worldwide problem. Lancet Neurol. 2004;3:475.
Frye MA. Bipolar disorder—a focus on depression. N Engl J Med. 2011;364:51.
Gilden DH. Bell’s palsy. N Engl J Med. 2004;351:1323.
Goldstein LB, et al. on behalf of the American Heart Association Stroke Council, Council on Cardiovascular Nursing Council on Epidemiology and Prevention Council for High Blood Pressure Research, Council on Peripheral Vascular Disease, and Interdisciplinary Council on Quality of Care and Outcomes Research: Guidelines for the primary prevention of stroke. A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42:517 http://stroke.ahajournals.org/content/42/2/517.full.pdf.
Goldstein LB, Simel DL. Is this patient having a stroke? JAMA. 2005;293:2391.
Gonzalez HM, et al. Depression care in the United State: too little for too few. Arch Gen Psychiatry. 2010;67:37.
Gunderson JG. Borderline personality disorder. N Engl J Med. 2011;364:2037.
Holsinger T, et al. Does this patient have dementia? JAMA. 2007;297:2391.
Houston JP, et al. A provisional screening instrument for four common mental disorders in adult primary care patients. Psychosomatics. 2011;52:48.
Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79:368.
Kanji JN, et al. Does this patient with diabetes have large-fiber peripheral neuropathy? JAMA. 2010;303:1526.
Kroenke K, et al. The patient health questionnaire somatic, anxiety, and depressive symptom scales: a systematic review. Gen Hosp Psychiatry. 2010;32:345.
Larrue V, et al. Etiologic investigation of ischemic stroke in young adults. Neurology. 2011;76:1983.
Maizels M. The patient with daily headaches. Am Fam Physician. 2004;70:2299.
Martin CL, et al. Neuropathy among the Diabetes Control and Complications Trial Cohort 8 years after trial completion. Diabetes Care. 2006;29:340.
Mendizabal M, Silva MO. Asterixis. N Engl J Med. 2010;363:9 http://www.nejm.org/doi/full/10.1056/NEJMicm0911157.
Moore FG, Chalk C. The essential neurologic examination. Neurology. 2009;72:2020.
National Institute of Mental Health. Suicide in the U.S.: statistics and prevention. [Updated June 2008. Available at] http://www.nimh.nih.gov/health/publications/suicide-in-the-us-statistics-and-prevention/index.shtml [Accessed September 22, 2013] .
National Institute of Mental Health. The numbers count: mental disorders in America. [Updated June 26, 2008. Available at] http://www.nihm.nih.gov/health/publications/the-numbers-count-mental-disorders-in-America/index.shtml [Accessed September 22, 2013] .
National Institute of Neurologic Disorders and Stroke, National Institutes of Health. Spinal cord injury: hope through research. [Updated December 31, 2012. Available at] http://www.ninds.nih.gov/disorders/sci/detail_sci.htm [Accessed January 31, 2013] .
O’Mahony R, et al. Synopsis of the National Institute for Health and clinical excellence guideline for prevention of delirium. Ann Intern Med. 2011;154:746.
Parry SW, Tan MP. An approach to the evaluation and management of syncope in adults. BMJ. 2010;340:340.
Pascuzzi RM. Peripheral neuropathy. Med Clin North Am. 2009;93:317.
Petersen RC. Mild cognitive impairment. N Engl J Med. 2011;364:2227.
Rao G, et al. Does this patient have Parkinson’s disease? JAMA. 2003;289:347.
Ryan RE, Pearlman SH. Common headache misdiagnoses. Prim Care Clin Office Pract. 2004;31:395.
Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl J Med. 2005;352:2618.
Scherer K, Bedlack RS, Simel DL. Does this patient have myasthenia gravis? JAMA. 2005;293(15):1906.
Scherokman B, Sclwa L, Alguire PC. Approach to common neurological symptoms in internal medicine: internal medicine curriculum in neurology. American Academy of Neurology and American College of Physicians. [Available at] http://www.aan.com/go/education/curricula/internal/toc; 2013 [Accessed January 31, 2013] .
Taylor FR. Diagnosis and classification of headache. Prim Care. 2004;31:243.
Unutzer J. Late-life depression. N Engl J Med. 2011;357:2269.
Velickovic M, Gracies JM. Movement disorders: keys to identifying and treating tremor. Geriatrics. 2002;57:32.
Wilson JF. Migraine. Ann Intern Med. 2007;144.
Wong CL, et al. Does this patient have delirium? Value of bedside instruments. JAMA. 2011;304:779.
Yew KS, Cheng E. Acute stroke diagnosis. Am Fam Physician. 2009;80:33.
1 Paralysis of the tongue muscles on the same side as the lesion. The tongue deviates to the side of the lesion when the patient is asked to stick out the tongue.
2 Paralysis of the soft palate and difficulty speaking, termed dysarthria.
3 Paralysis of the sternocleidomastoid or trapezius muscle, or both. This results in the inability to turn the head to the side opposite the lesion and to shrug the shoulder. There are many more clinical syndromes that are beyond the scope of this text. The reader is advised to review the neuroanatomy further to understand the complexities of these neurologic syndromes.
4 Tremors that result when the individual moves the hands to do something but that may not be present at rest.
5 Document a history with an observer, if possible.
6 Spontaneous contractions of groups of muscles that are visible on inspection.
7 This disease is also called Lou Gehrig’s disease, after the famous baseball player who was one of its victims.
8 An increase in muscle tone that results in continuous resistance to stretching. Spasticity is usually worse at extremes of range.
9 Spasm in which rigidity and relaxation alternate in rapid succession.
10 Dorsiflexion of the big toe on stimulation of the sole of the foot.
11 Common causes include electrolyte abnormalities, endocrine disorders, liver or kidney failure, vitamin deficiencies, poisoning, intoxications, and marked changes in body temperature.
12 Commonly related to phenytoin (Dilantin) therapy.
[/level-membership-for-internal-medicine-category][not-level-membership-for-internal-medicine-category]Chapter 18
The Nervous System
As the debility increases and the influence of the will over the muscles fades, the tremulous agitation becomes more vehement. It now seldom leaves him for a moment; but even when exhausted nature seizes a small portion of sleep, the motion becomes so violent as not only to shake the bed-hangings, but even the floor and sashes of the room. The chin is now almost immovably bent down upon the sternum. The slops with which he is attempted to be fed, with the saliva, are continually trickling from the mouth. The power of articulation is lost. The urine and faeces are passed involuntarily; and at the last, constant sleepiness, with slight delirium, and other marks of extreme exhaustion, announce the wished-for release.
James Parkinson (1755–1824)
General Considerations
By the second century CE, Galen had already described the cerebral ventricles, 7 of the 12 cranial nerves, and the cerebral convolutions. There was, however, little further interest in the anatomy and physiologic characteristics of the neurologic system until the sixteenth century. In 1543, Andreas Vesalius illustrated the basal ganglia, and in 1552, Bartolommeo Eustachius described the cerebellar peduncles and the pons.
In the seventeenth century, Thomas Willis published descriptions and illustrations of the cerebral circulation, the “striate body,” and the internal capsule. Caspar Bartholin and others thought that the function of the cerebral cortex was to protect the blood vessels, whereas other investigators believed that the cerebrum possessed higher functions. François Pourfour du Petit stressed that the cortex was responsible for motor activity. This concept lay dormant until the end of the nineteenth century.
Careful anatomic descriptions of the tracts, nuclei, and gyri were contained in the writings of scientists of the eighteenth and early nineteenth centuries. Johann Christian Reil and Karl Friedrich Burdach provided names for the many gross anatomic structures that had been illustrated by others in previous centuries. Reil has been credited with the naming of the insula, capsule, uncinate and cingulate fasciculi, and tapetum. The uncus, lenticular nucleus, pulvinar, and gyrus cinguli were named by Burdach. During this same period, Samuel von Soemmering, Felix Vicq d’Azyr, Franz Josef Gall, Louis Gratiolet, and Luigi Rolando made many detailed illustrations of the cerebral convolutional patterns.
The next instance was in a man wounded by the horn of an ox. The point entered under the angle of the jaw and came out before the ear. … He remains now a singular proof of the effects of the loss of function in the muscles of the face by this nerve being divided. The forehead of the corresponding side is without motion, the eyelids remain open, the nostril has no motion in breathing, and the mouth is drawn to the opposite side.
This is the classic description of facial nerve (seventh cranial nerve) palsy, also known as Bell’s palsy.
In the mid-nineteenth century, an interest in microscopic neuroanatomy developed. Jan Purkinje, Theodor Schwann, and Hermann von Helmholtz were a few of the many neuroanatomists who contributed valuable information about the intricacies of the nervous system. However, not until the late nineteenth century were specific staining techniques developed by Camillo Golgi, Vittorio Marchi, and Franz Nissl, which led to the current understanding of neuronal disease. The nerve cell had finally been discovered.
The twentieth century was a period of further progress in the description of the cerebral cortex, anterior commissure, thalamus, and hypothalamus. A major advance came from the work of Santiago Ramón y Cajal in 1904. His histologic exploration clarified the complexities of the neuron. Not until 1925 were the hypophysial-hypothalamic connections described, and even today, the function of the hypothalamus is not fully understood.
It has been suggested that more than 40% of patients who present to internists have symptoms referable to neurologic disease. The internist must be able to identify the early signs and symptoms of neurologic disease and initiate the appropriate therapy. All too often, subtle signs and symptoms may be ignored, and a diagnosis is not made until advanced disability is apparent.
Cerebrovascular disease is one of the most devastating diseases of our time. It remains the third leading cause of death in the United States. More than 700,000 Americans suffer a stroke yearly, and it is the number one cause of disability; more than 3 million Americans currently live with permanent brain damage caused by such an event. On average, someone in the United States suffers a stroke every 53 seconds, and every 3.3 minutes, someone dies of one. In 2011, there were 2,513,171 deaths from cardiovascular disease, including 128,931 deaths related to cerebrovascular disease. The number of noninstitutionalized adults who have ever had a stroke is 6.2 million people. The debilitating consequences of stroke and the economic effect on society are enormous.
The generalist or internist holds an important position because a patient with a neurologic problem usually seeks help from that physician first. A thorough knowledge of basic neuroanatomy and physiology is the cornerstone of neurologic diagnosis.
Structure and Physiologic Characteristics
The brain, which is enclosed in the cranium and surrounded by the meninges, is the center of the nervous system. The brain can be divided into paired cerebral hemispheres, basal ganglia, diencephalon (thalamus and hypothalamus), brain stem, and cerebellum.
The two cerebral hemispheres make up the largest portion of the brain. Each hemisphere can be subdivided into four major lobes named for the cranial bones that overlie them: frontal, parietal, occipital, and temporal. The fissures and sulci divide the cerebral surface. A deep midline, longitudinal fissure separates the two hemispheres. The convolutions, or gyri, lie between the sulci. A lateral view of the left cerebral hemisphere is pictured in Figure 18-1. Figure 18-2 is a medial view of the right cerebral hemisphere. A basal view of the cerebral hemispheres is pictured in Figure 18-3.
Figure 18–1 Lateral view of the left cerebral hemisphere.
Figure 18–2 Medial view of the right cerebral hemisphere.
Figure 18–3 Basal view of the cerebral hemispheres.
The cerebrum is responsible for motor, sensory, associative, and higher mental functions. The primary motor cortex is located in the precentral gyrus. Neurons in this area control voluntary movements of the skeletal muscles on the opposite side of the body. An irritative lesion in this area may cause seizures or changes in consciousness. Destructive lesions in this area can produce contralateral flaccid paresis or paralysis.
The primary visual cortex is located in the occipital lobe along the calcarine fissure, which divides the cuneus from the lingual gyri. Irritative lesions in this area produce visual symptoms such as flashes of light or rainbows. Destructive lesions cause homonymous hemianopsia on the contralateral side. Central macular vision is spared.
The primary auditory cortex is located in the temporal lobe along the transverse temporal gyrus. Irritative lesions in this area produce a buzzing or ringing in the ears. Destructive lesions almost never produce deafness.
The basal ganglia are situated deep within the cerebral hemispheres. The structures constituting the basal ganglia include the caudate and lenticular nuclei, as well as the amygdala. The amygdala is part of the limbic system and is concerned with emotion. All other components are important structures in the extrapyramidal system, which is concerned with modulating voluntary body movements, postural changes, and autonomic integration. The basal ganglia are especially involved with fine movements of the extremities. Disturbances of the basal ganglia can result in tremors and rigid movements.
The thalamus is a large nuclear mass located on each side of the third ventricle. The thalamus is the chief sensory and motor integrating mechanism of the neuraxis. All sensory impulses, except olfactory ones, and the major output from systems that modulate and modify motor function (i.e., the cerebellum and corpus striatum) terminate in the thalamus, from which they are projected to specific areas of the cerebral cortex. The thalamus is involved in certain emotional connotations that accompany most sensory experiences. Through its connections with the hypothalamus and striatum, the thalamus can influence visceral and somatic effectors serving primarily affective reactions. Through its control of the electrical excitability of the cerebral cortex, the thalamus plays a dominant role in the maintenance and regulation of the state of consciousness, alertness, and attention. The thalamus may be the critical structure for pain perception and thermal sense, which remain after complete destruction of the primary sensory cortex. Thermal sense endows sensation with discriminative faculties and is not concerned with the recognition of crude sensory modalities.
The hypothalamus is located below the thalamus. It includes the optic chiasm and the neurohypophysis. The hypothalamus is responsible for many regulatory mechanisms, such as temperature regulation; neuroendocrine control of catecholamines, thyroid-stimulating hormone, adrenocorticotropic hormone, follicle-stimulating and luteinizing hormones, prolactin, and growth hormones; thirst; appetite; water balance; and sexual behavior.
The brain stem consists of the midbrain, pons, and medulla. Figure 18-4 shows the external anatomy of the brain stem. The brain stem is responsible for relaying all messages between the upper and lower levels of the central nervous system. Cranial nerves III to XII also arise from the brain stem. The brain stem contains the reticular formation, a network that provides for constant muscle stimulation to counteract the force of gravity. In addition to its antigravity effects, this area of the brain is essential for the control of consciousness. The neurons in the reticular activating system are capable of waking and arousing the entire brain.
Figure 18–4 Anatomy of the brain stem.
The midbrain contains the superior and inferior colliculi, the cerebral peduncles, and the motor nuclei of the trochlear (cranial nerve IV) and oculomotor (cranial nerve III) nerves. The superior colliculi are associated with the visual system, and the inferior colliculi are associated with the auditory system. The cerebral peduncles converge from the inferior aspect of the cerebral hemispheres and enter the pons. A destructive lesion of the superior colliculi causes paralysis of upward gaze. Destructive lesions of the cranial nerve nuclei produce paralysis of the affected nerve. A destructive lesion of the cerebral peduncle gives rise to spastic paralysis on the other side of the body. Destruction of other tracts in the midbrain results in rigidity and involuntary movements.
The pons lies ventral to the cerebellum and rostral to the medulla. The abducens, facial, and acoustic (and vestibular) nuclei are found in the pons, and their nerves exit through a groove that divides the pons from the medulla. The motor and sensory nuclei of the trigeminal nerve are also located in the pons. At this level, the corticospinal tracts (also known as the pyramidal tracts) have not yet crossed, and a lesion at this level produces loss of voluntary movement on the opposite side. Destructive lesions of the pons may produce a variety of clinical syndromes, such as the following:
• Contralateral hemiplegia with ipsilateral facial palsy (Bell’s palsy)
The medulla is the portion of the brain stem between the pons and the spinal cord. The nuclei of the hypoglossal, vagus, glossopharyngeal, and spinal accessory nerves are located in the medulla. It is within the medulla that the majority of fibers in the corticospinal tracts cross to the opposite side. Destructive lesions in the medulla produce symptoms that are referable to the tracts interrupted by the lesion. Some clinical syndromes are as follows:
• Contralateral hemiplegia with ipsilateral hypoglossal palsy1
• Ipsilateral vagal palsy2 with contralateral loss of pain and temperature sense
• Ipsilateral vagal palsy with ipsilateral spinal accessory palsy3
• Ipsilateral vagal palsy with ipsilateral hypoglossal palsy
• Ipsilateral vagal palsy, ipsilateral spinal accessory palsy, and ipsilateral hypoglossal palsy
The cerebellum is located in the posterior fossa of the skull and is composed of a small midline vermis and two large lateral hemispheres. The cerebellum acts to keep the individual oriented in space and to halt or check motions. The cerebellum is also responsible for the fine movements of the hands. Essentially, the cerebellum coordinates and refines the action of muscle groups to produce steady and precise movements. Destructive lesions of the cerebellum cause swaying, staggering, intention tremors,4 and inability to change movements rapidly.
Of the blood supply to the brain, 80% is through the internal carotid arteries and 20% is through the vertebral basilar arteries. Each internal carotid artery terminates at the anterior cerebral and middle cerebral arteries. The posterior cerebral artery arises from the basilar artery, which joins with the posterior communicating artery, a branch of the internal carotid artery. The two anterior cerebral arteries are joined by the anterior communicating artery. This vascular network forms the circle of Willis, located at the base of the brain. This is illustrated in Figure 18-5.
Figure 18–5 Circle of Willis.
Continuous with the medulla is the spinal cord, a cylindric mass of neuronal tissue measuring 40 to 50 cm in length in adults. Its distal end attaches to the first segment of the coccyx. The spinal cord is divided into two symmetric halves by the anterior median fissure and the posterior median sulcus. Each half contains white and gray matter, which can be further subdivided. This is illustrated in Figure 18-6.
Figure 18–6 Cross-sectional view through the spinal cord.
The white matter of the spinal cord consists of tracts that link segments of the spinal cord and connect it to the brain. There are three main columns (funiculi). Between the anterior median fissure and the anterolateral sulcus is the anterior white column, which contains the descending fibers of the ventral corticospinal tract and the ascending fibers of the ventral spinothalamic tract. The ventral corticospinal tract is involved with voluntary motion, and the ventral spinothalamic tract carries impulses related to light touch.
The lateral white column is located between the anterolateral and posterolateral sulci and contains the descending fibers of the lateral corticospinal tract and the ascending spinocerebellar and lateral spinothalamic tracts. The lateral corticospinal tract is responsible for voluntary movement; the spinocerebellar tracts, for reflex proprioception; and the lateral spinothalamic tract, for pain and temperature sensation.
The posterior white column is located between the posterolateral and posterior median sulci. The most important fibers in this column are the ascending fibers of the fasciculus gracilis and fasciculus cuneatus. These tracts are involved with vibration sense, passive motion, joint position, and two-point discrimination.
There are 31 pairs of spinal nerves, each with a ventral (motor) and dorsal (sensory) root. The ventral root consists of efferent nerve fibers, which originate in the anterior and lateral gray matter (T1 to T2 only) and travel to the peripheral nerve and muscle, which constitute the motor root. The dorsal root consists of afferent nerve fibers whose cell bodies are in the dorsal root ganglion, which is the sensory root.
The spinal nerves are grouped into 8 cervical (C1 to C8), 12 thoracic (T1 to T12), 5 lumbar (L1 to L5), 5 sacral (S1 to S5), and 1 coccygeal nerve. These nerves are illustrated in Figure 18-7.
Figure 18–7 Spinal nerves.
A spinal reflex involves an afferent neuron and an efferent neuron at the same level in the spinal cord. The basis for this reflex arc is an intact sensory limb, functional synapses in the spinal cord, an intact motor limb, and a muscle capable of responding. The afferent and efferent limbs travel together in the same spinal nerve. When a stretched muscle is suddenly stretched further, the afferent sensory limb sends impulses through its spinal nerve that travel to the dorsal root of that nerve. After reaching a synapse in the gray matter of the spinal cord, the impulse is transmitted to the ventral nerve root. These impulses are then conducted through the ventral root to the neuromuscular junction, where a brisk contraction of the muscle completes the reflex arc. Figure 18-8 illustrates a reflex spinal arc.
Figure 18–8 Reflex spinal arc.
The afferent sensory limb is important not only in the reflex arc but also in the conscious appreciation of sensation. Nerve fibers carrying pain and temperature sensation enter the spinal cord and cross to the other side within one or two spinal segments. They ascend in the contralateral lateral spinothalamic tract, travel through the brain stem and the thalamus, and end in the postcentral gyrus of the parietal lobe, as illustrated in Figure 18-9A. Fibers carrying proprioceptive sensation from muscles, joints, and tendons enter the dorsal root and participate in the reflex arc. Other fibers carrying proprioceptive sensation pass directly into the posterior columns and ascend in the fasciculi gracilis and cuneatus to their ipsilateral nuclei, cross in the medial lemniscus, reach a synapse in the thalamus, and end in the postcentral gyrus of the parietal lobe. Still other proprioceptive fibers ascend crossed and uncrossed in the spinocerebellar tracts to the cerebellum. These additional pathways are illustrated in Figure 18-9B.
Review of Specific Symptoms
The most common symptoms of neurologic disease are as follows:
Headache
Headache is the most common neurologic symptom. It has been estimated that more than 35 million individuals in the United States suffer from recurrent headaches. Most of these patients have headaches that are related to migraine, muscle contraction, or tension. A headache pattern that is unchanged and has been present for several years is unlikely to be related to present illness of the patient. Several points must be clarified for any patient complaining of a recent change in the frequency or severity of headaches. Ask the following questions:
“How long have you been having headaches?”
“When did you notice a change in the pattern or severity of your headaches?”
“How has the pattern of your headaches changed?”
“How often do your headaches occur?”
“How long does each headache last?”
“Which part of your head aches?”
“What does the headache feel like?”
“How quickly does the headache reach its maximum?”
“When you get headaches, do you have any other symptoms?”
“Are you aware of anything that produces the headaches?”
“Are there any warning signs?”
Patients complaining of a sudden onset of headache usually have more serious illnesses than patients with headaches of chronic duration. A continuous headache can be related to muscle spasm, whereas a recurrent headache may be a migraine or cluster headache. A throbbing headache often has a vascular cause. Certain headaches are associated with visual phenomena, nausea, or vomiting. In patients with increased intracranial pressure, any maneuver that increases the pressure, such as coughing or bending, may worsen the headache. In any patient who experiences a severe, sudden headache, stroke should be suspected.
Migraine is a biphasic type of headache associated with a prodromal phase, called the aura, followed by the headache phase. During the aura, one or more physiologic events may occur. These include transient experiences of autonomic, visual, motor, or sensory phenomena. Common visual symptoms are photophobia, blurred vision, and scotomata. As the aura fades, the headache begins. It is usually unilateral and is often described as pulsating; it can last for hours to days. Migraine headaches are often triggered by stress, anxiety, the use of birth control pills, and hormonal changes. Many patients experience migraine headaches after a period of excitement. Other important triggers are hunger and the ingestion of certain foods such as chocolate, cheese, cured meats, and highly spiced foods. There is often a family history of migraine.
Cluster headaches are associated with oculosympathetic disturbances. The typical patient is a middle-aged man complaining of recurrent episodes of pain around the eye that last for up to 1 hour. Classically, cluster headaches awaken the patient from sleep on successive nights for 2 to 4 weeks. There is ipsilateral miosis, ptosis, conjunctival edema, tearing, and nasal stuffiness during the headache. It is thought that alcohol may precipitate such attacks.
Headache may be the result of referred pain from sinus infections, ocular disease, or dental disease. Systemic conditions such as viral infections, chronic obstructive pulmonary disease, and poisoning may produce headaches. Determine whether the patient is taking any medications that may be producing the head pain. (See Table 18-2, which provides an approach to patients with the symptom of headache.)
Loss of Consciousness
Loss of consciousness—syncope—may result from cardiovascular or neurologic causes. The cardiovascular causes are discussed in Chapter 11, The Heart, and Chapter 12, The Peripheral Vascular System. The term blackout is commonly used, but it may mean different conditions to the patient and the interviewer. Any patient who uses this term should be asked to clarify its meaning. The patient may be referring to an actual loss of consciousness, a dimming of vision, or a decreased awareness of the environment without an actual loss of consciousness.
A useful way to clarify the symptom of loss of consciousness is to ask the patient, “Have you ever lost consciousness, fainted, or felt that you were not aware of your surroundings?” If the patient answers in the affirmative, identify the cause of the loss of consciousness. Ask the following questions:
“Can you describe the attack to me—every event as it occurred until you lost consciousness?”
“Did anyone witness the attack?”5
“Were there any symptoms that preceded the attack?”
“Were you told that there were body movements?”
“Can you describe everything you remember after the attack until you felt completely normal?”
“Was there a period of sleepiness that followed?” If yes, “For how long did this period last?”
“How did you feel after the attack? Were you confused?”
“Did you notice afterward that you had urinated or had a bowel movement during the attack?”
Epileptic seizures may produce a loss of consciousness and are caused by the sudden, excessive, disorderly discharge of neurons. The first step in approaching the symptom of seizure is to identify its type. If the discharge is focal, the clinical seizure reflects the effect of the excessive discharge in that area of the body. For example, if the discharge is located in the inferior precentral gyrus, involved with hand and arm motion, the seizure is characterized by involuntary motion of the hand and arm. A generalized seizure results from a discharge in the subcortical structures, such as the thalamocortical radiations. These have widespread bilateral cortical connections. There are three main types of generalized seizures:
A petit mal seizure is characterized by a sudden attack of unconsciousness lasting only about 10 seconds, usually without any warning. During the petit mal seizure, the patient appears to be staring or daydreaming. There is no associated falling or involuntary limb motion. The patient rapidly returns to normal activity without being aware of the attack. These seizures are most common in children 5 to 15 years of age. On occasion, they may persist into adulthood.
A grand mal seizure is a generalized major motor convulsion. Affected patients lose consciousness, and many fall down rigidly. In 50% of patients with grand mal seizures, there is an aura of giddiness, involuntary twitching, change in mood, confusion, or epigastric discomfort as the seizure begins. Some patients may cry out initially. During this tonic phase, there is an increase in muscle tone, resulting in a rigid, flexed posture and then a rigid, extended posture. The patient may become apneic and cyanotic. The eyes may open and stare or may be deviated to one side. The clonic phase follows, with involuntary movements of the body. These are often associated with salivation, eye rolling, and incontinence. Biting the tongue is common. After the clonic phase, the individual passes into a phase resembling sleep from which she or he cannot be easily awakened. Postictally, or after the seizure, the patient may be confused and often falls into a deep sleep that lasts for hours. Accompanying muscle pain and headache are common.
A myoclonic seizure is a minor motor seizure characterized by sudden muscle contractions of the face and upper extremities. The eyelids and forearms are commonly affected. There is no detectable loss of consciousness.
Febrile convulsions are common in children from 6 months to 6 years of age and are similar to grand mal seizures. When a child has a high fever, a seizure lasting less than 10 minutes may occur. The younger the child is at the time of the first febrile seizure, the greater is the likelihood that seizures will recur.
“Dizziness”
Dizziness is a term used frequently by patients and should be avoided by the interviewer. “Dizziness” may be the patient’s description of vertigo, ataxia, or lightheadedness. Any time the patient uses this term, it must be clarified by additional questioning, because different pathophysiologic mechanisms may be responsible. The interviewer needs to differentiate vertigo from ataxia. If the patient complains of “dizziness,” it is important to ask these questions:
“Would you describe the dizziness as a strange spinning sensation in your head?”
“Did the room spin, or did it feel as if you were spinning?”
Vertigo is partially discussed in Chapter 8, The Ear and Nose. Vertigo is the hallucination of movement. Acute vertigo may be associated with nausea, vomiting, perspiration, and a sense of anxiety. Ask patients whether they have the sensation that objects are moving around them or that they are spinning or moving. In addition to the questions in Chapter 8, ask the following:
“During the attack, did you experience any nausea or vomiting?”
“Have you noticed any problem with your hearing or ringing in your ears?”
Ménière‘s disease can result in protracted attacks of severe vertigo associated with vomiting. Many patients with Ménière’s disease also have the symptoms of tinnitus and hearing loss. During the attack, the patient is unsteady, with horizontal nystagmus directed away from the affected ear. Certain drugs (such as gentamicin) are associated with changes in the labyrinth of the ear and can cause vertigo and deafness.
Dizziness and stumbling are commonly associated with a stroke.
Ataxia
Disruption of the vestibular-ocular-cerebellar control mechanism produces ataxia. Ataxia is persistent unsteadiness in the upright position. Any patient complaining of dizziness must be evaluated for abnormal function of the vestibular, visual, proprioceptive, and cerebellar systems. Equilibrium requires the integration of sensory input and motor output, acting primarily at a reflex level for the maintenance of balance. The ears and eyes and their central connections in the brain stem and the cerebellum are intimately involved in balance. Any patient with ataxia should be asked the following questions:
“Are you unsteady when you walk?”
“Have you noticed that the dizziness is worse when your eyes are open or closed?”
“What does your diet consist of? What did you eat yesterday?”
Abnormal proprioceptive input from the lower extremities can cause ataxia. Severe posterior column damage from syphilis, vitamin B12 deficiency, or multiple sclerosis may produce a “sensory” ataxia, resulting in a wide-based, high-stepping gait. The gait is worsened by having the patient close the eyes and is improved by having the patient observe the feet. Vitamin B12 deficiency may result from pernicious anemia or from inadequate intake, although poor nutrition is a rare cause. “Motor” ataxia results from an abnormality in the cerebellum and central vestibular pathways. It is characterized by wide-based, irregular placement of the feet and poor placement of the center of gravity, with a lurching to either side.
Changes in Consciousness
Changes in consciousness may be related to changes in attention span, perception, arousal, or a combination. In confusional states, the patient has the ability to receive information normally, but the processing is disturbed. In delirium, the individual perceives the information abnormally. Any patient, or member of the patient’s family, who indicates that a change in consciousness has occurred should be asked the following:
“Did the change occur suddenly?”
“Have there been other symptoms associated with the change in consciousness?”
“Do you use any medications? Depressants? Insulin? Alcohol? Recreational drugs?”
“Is there a history of psychiatric illness?”
“Is there a history of kidney disease? Liver disease? Thyroid disease?”
Many factors can produce changes in consciousness. The acuteness of the change in consciousness is often helpful in making a diagnosis. Hemiparesis, paresthesia, hemianopsia, garbled speech, and arm and leg weakness are common associated symptoms of supratentorial lesions. Brainstem lesions are often associated with changes in consciousness and with nystagmus, vomiting, double vision, nausea, and excessive yawning. Drugs of any type can produce acute changes in consciousness. A history of earlier psychiatric illness is important. Toxic and metabolic changes are frequently associated with changes in consciousness. Liver or kidney failure, myxedema, and diabetic ketoacidosis are common causes of metabolic abnormalities. A history of head trauma may result in a subdural hematoma and produce a gradual change in consciousness.
Visual Disturbance
Visual disturbances are common neurologic presenting symptoms. The most important symptoms are acute visual loss, chronic visual loss, and double vision. Ask any patient complaining of visual disturbances the following questions:
“How long have you noticed these visual changes?”
“Is the visual loss associated with pain?”
“Do you have a history of glaucoma?”
Acute painless visual loss is caused by either a vascular accident or a retinal detachment. Painless loss of vision over a longer period occurs with compression of the optic nerve or tract or radiation. Glaucoma is often the cause of chronic, insidious, painless loss of vision. Acute narrow-angle glaucoma, however, may be responsible for transient loss of vision in association with intense ocular pain. Episodes of migraine may produce transient episodes of visual loss before the development of the headache. Amaurosis fugax is transient visual loss lasting up to 3 minutes and is a feature of internal carotid artery disease.
Double vision, or diplopia, is discussed in Chapter 7, The Eye. Ocular motor palsies, thyroid abnormalities, myasthenia gravis, and brainstem lesions are well-known causes of diplopia. Ocular motor palsies can occur in trauma, multiple sclerosis, myasthenia gravis, aneurysms of the circle of Willis, diabetes, and tumors. Ask the following questions of any patient complaining of diplopia:
“In which field of gaze do you have double vision?”
“Did the double vision occur suddenly?”
“Was there any pain associated with the double vision?”
“Has there been any injury to your head or eye?”
“Have you ever been told that your blood pressure was elevated?”
“Does the double vision get worse when you are tired?”
“Have you been exposed to the AIDS [acquired immune deficiency syndrome] virus?”
When a cranial nerve is affected, resulting in an extraocular muscle palsy, the patient may complain of diplopia in one field of gaze when the affected eye is unable to move conjugately with the other. Ocular palsies involve the third, fourth, and sixth cranial nerves. A complete third (oculomotor) nerve palsy causes ptosis, mydriasis, and loss of all extraocular movements except abduction. Trauma, multiple sclerosis, tumors, and aneurysms are the most frequent causes. Aneurysms of the posterior communicating artery can involve the third nerve, which passes near the artery on its way to the cavernous sinus. Cavernous sinus thrombosis, not infrequently seen in patients with AIDS, may also produce a complete third nerve palsy. Pupil-sparing third nerve, fourth (trochlear) nerve, and sixth (abducens) nerve palsies are seen in diabetic patients and in patients with long-standing hypertension. Patients with myasthenia gravis often have diplopia in the later part of the day as the muscles tire and weaken.
Visual disturbances, including blocked vision or loss of vision in one eye, blurry vision, or “graying out” are seen frequently in patients suffering a stroke.
Dysphasia
Speech abnormalities, or dysphasia, may be either nonfluent (expressive) or fluent (receptive). In expressive aphasia, the speech pattern is hesitant and labored, with poor articulation. The patient has no problem with comprehension. When asked to say, “no ifs, ands, or buts,” the patient has great difficulty. In receptive aphasia, the speech is rapid and appears fluent but is full of syntax errors, with the omission of many words. Handwriting changes are nonspecific but indicate an impairment of neuromuscular control. Ask the following questions:
“Have you noticed any recent change in your speech pattern, such as slurring of your words?”
“Do you have trouble understanding things that are said to you?”
“Have you had any difficulty finding the right word in conversation?”
Language problems, as well as slurred speech, are found commonly in patients suffering a stroke.
Dementia
An important symptom of neurologic disease is failing memory. Dementia can be defined as the progressive impairment of orientation, memory, judgment, and other aspects of intellectual function. Dementia is a symptom rather than a specific disease entity. The most common cause of dementia is Alzheimer‘s disease. Other causes include Parkinson’s disease, vascular disorders, metabolic disorders, drugs, tumors, vitamin B12 deficiency, tertiary syphilis, and normal-pressure hydrocephalus. It is common for patients with early dementia to recognize an increasing inability to comprehend written material. They are aware also of their cognitive impairment but fail to acknowledge it with friends and family. It is often so insidious that individuals with dementia may live with their family for years without the family recognizing the problem. In addition, family members and friends may not wish to acknowledge the failing mental capacities.
Ask the patient and his or her friends and family the following:
“Have you noticed any change in your memory lately?”
“Do you have difficulty reading or understanding what you have read?”
“What was the patient’s personality like a few years ago?”
“When was the last time the patient seemed normal?”
“What does the patient’s diet consist of? Does he or she eat well?”
Cerebrovascular Accident
Strokes, or cerebrovascular accidents, are common. Most are thromboembolic (80%), but some are hemorrhagic (20%). Thirty percent of patients who sustain a stroke die within the first month. Most patients with strokes have paresis of at least one limb. Transient ischemic attacks (TIAs) are short episodes manifested by focal neurologic dysfunction. They usually last only a few minutes, after which complete recovery occurs. The importance of TIAs is that, in 30% of affected patients, a stroke occurs within 4 to 5 years.
Gait Disturbance
Gait disturbances may occur for a variety of reasons. Gait may be changed by local pain in the foot, pain in a joint, claudication of the hip or leg, bone disease, vestibular problems, and extrapyramidal disorders. Interruption of the corticospinal tracts in the cerebrum after a stroke produces a spastic weakness in the contralateral leg. The foot is dragged, and the whole leg appears stiff and extended. Lesions in the spinal cord may produce a spastic paralysis affecting both legs. The gait is slow and stiff, with small steps. Patients with Parkinson’s disease walk stooped over, with short, quick, shuffling steps. Any patient with a gait disturbance should be asked the following:
Patients with vascular occlusive disease of the hip or leg may experience pain while walking and may alter their gait. Diabetes, syphilis, and pernicious anemia may produce a sensory loss, and each condition can result in gait abnormalities.
Tremor
A tremor is a rhythmic motion of the distal parts of the limbs or head. A physiologic tremor has an oscillation of 10 to 12 cycles per second and is more obvious after exercise. A pathologic tremor is slower. Parkinson‘s disease is the most frequently encountered extrapyramidal movement disorder. In this condition, the tremor is present at rest and is decreased with action. It has a frequency of three to six cycles per second and is worsened by anxiety. An intention, or ataxic, tremor is slow (two to four cycles per second) and worsens on attempted movement. Multiple sclerosis is one of the many causes of intention tremor. Metabolic problems from liver or kidney failure are frequently responsible. Withdrawal from alcohol or caffeine is often a precipitating factor. Any patient with the symptom of tremor should be asked these questions:
“Does the tremor worsen when you try to do something?”
“Is there a history of thyroid disease?”
“Have you ever been told about any problems with your liver or kidneys?”
“What is your daily consumption of alcoholic beverages?”
Chorea is involuntary jerky motions of the face and limbs. A common cause is Huntington‘s disease, in which chorea is accompanied by personality changes and progressive mental deterioration terminating in dementia.
“Numbness”
Numbness is another term used by patients to indicate a variety of problems. “Numbness” can be used by patients to describe a “pins-and-needles” sensation, coolness, pain, or clumsiness. The interviewer should be sure to clarify the meaning. The examiner must be careful during the physical examination to palpate the distal pulses in any patient complaining of numbness, because arterial insufficiency is a possible cause. Diabetes mellitus is a common cause of lower extremity numbness. Multiple sclerosis may cause numbness in any extremity.
“Weakness”
Weakness may be a symptom of the motor system. A patient with a proximal arm motor weakness complains of difficulty brushing hair, shaving, or reaching up to shelves. A patient with distal arm motor weakness complains of difficulty putting a button through a buttonhole, using keys, or writing with a pen or pencil. Proximal leg motor weakness is characterized by difficulty climbing stairs or getting into bed or the bathtub. Footdrop is a classic sign of distal leg motor weakness. Chapter 17, The Musculoskeletal System, reviews some of the important questions related to weakness.
Face droop and weakness are common signs of a stroke, as is the presence of numbness or clumsiness in one arm or hand.
Pain
Pain is an infrequent symptom of neurologic disease, but it merits mention. Trigeminal neuralgia, also known as tic douloureux, is the occurrence of severe, jabbing pain lasting only seconds in the distribution of the maxillary or mandibular divisions of the trigeminal nerve (Fig. 18-10). It is frequently provoked by motion, touch, eating, or exposure to cold temperatures. Another cause of facial pain is the cluster headache, already discussed. Herpes zoster infection of a sensory nerve root, also known as shingles, manifests with intense pain along the distribution of that nerve root. The classic linear, vesicular skin eruption develops 3 to 4 days later along the distribution of the nerve. Figure 5-70 shows the classic dermatologic manifestations of herpes zoster infection of spinal nerve T3.
Sciatica is intense pain shooting down the leg in the distribution of the sciatic nerve. In this condition, there is impingement of portions of the sciatic nerve by the vertebrae. Arthritis of the lumbosacral spine is frequently the cause.
Sometimes the paresthesias associated with demyelinating diseases are so intense that the patient may describe them as pain.
Patients with inflammation of the meninges often complain of pain in the neck and a resistance to flexion of the neck. If meningitis is suspected, have the patient lie on his or her back. Place your hand behind the patient’s neck and flex it until the chin touches the sternum. In patients with meningitis, there is neck pain and resistance to motion. This is called Brudzinski‘s sign. There may also be flexion of the patient’s hips and knees. Jósef Brudzinski described at least five different physical signs indicative of meningeal irritation. This sign is the best known and most reliable sign. Another sign of meningeal irritation can be elicited while the patient lies on the back and you flex one of the patient’s legs at the hip and knee. If pain or resistance is elicited as the knee is extended, a positive Kernig‘s sign is present.
Effect of Chronic Neurologic Disease on the Patient
The ramifications of chronic neurologic disease on the patient and his or her family are enormous. All family members experience emotional pain while observing the progressive clinical changes. The family bears an immense personal burden in assisting the patient to cope with disability.
One example of a progressive neurologic condition is Alzheimer’s disease. A devastating chronic disorder of unknown cause, Alzheimer’s disease is the most common diffuse brain degeneration causing brain failure. This condition is characterized by progressive and widespread brain degeneration with a hopeless prognosis.
Memory problems and impairment of intellectual function are the main symptoms of Alzheimer’s disease. Depression is common. Patients may have significant cognitive impairment, which ruins their ability to negotiate their environment. They may forget where they live. They may forget to turn off a gas burner on the stove or to put out a cigarette. They may wander aimlessly outdoors.
Manifestations of Alzheimer’s disease span a clinical spectrum from awareness of the disability to a vegetative state. Many patients lose touch with reality. During an interview with such a patient, it may become clear that even the ability to describe the patient’s own medical history has been lost.
[/not-level-membership-for-internal-medicine-category]
