The descending tracts
Basic anatomy and function of the main descending tracts
The descending tracts originate from various regions of the brain stem and cerebral cortex and in the main synapse upon the alpha motor neurons (AMN) in the ventral horn of the spinal cord (S2.13). Ultimately, the AMN innervates various muscles to produce a motor contraction and achieve a motor goal. However, the descending tracts are not just a relay system as their influence via interneuron connections also gives precise control of motor output.
The descending tracts can functionally be divided into:
Basic structure of a descending tract
Most descending tracts show typical features within their anatomical structure:
A 1st order neuron with its cell body in the cerebral cortex or brain stem decussates (i.e. the neuron crosses to the opposite side of the body) and descends in the spinal cord. These neurons synapse on a 2nd order neuron
A 2nd order neuron which has its cell body in the spinal cord at the level at which it terminates/leaves the spinal cord. These neurons synapse on a 3rd order neuron
A 3rd order neuron is the AMN, with its cell body in the ventral horn of the spinal cord and which innervates a skeletal muscle.
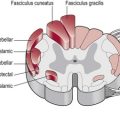
The precise detail of each individual descending tract is beyond the scope of this book, however the function of each tract is shown in Table 14.1. Knowledge of the basic structure and anatomical orientation (Fig. 14.1) of the descending tracts, especially where each tract decussates, is important in understanding the clinical presentation of a patient with a lesion involving the spinal cord.
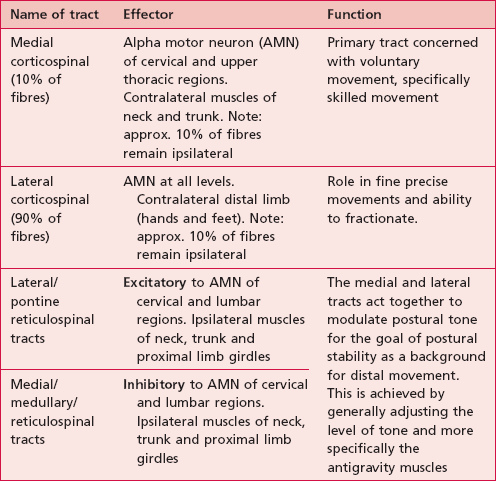
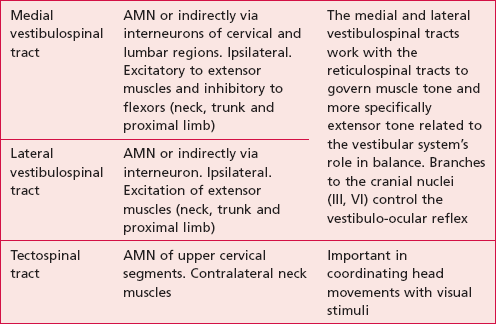
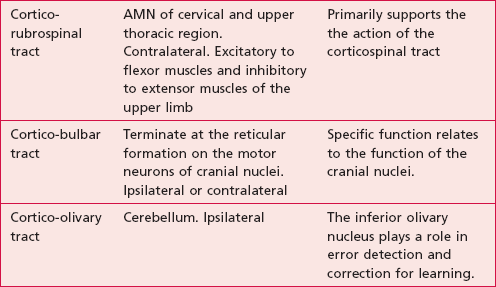
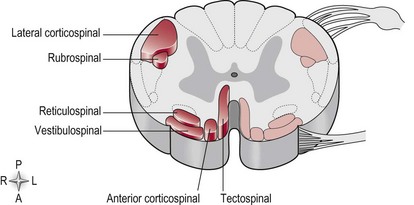
Figure 14.1 A cross-section of the spinal cord showing the orientation of the main descending tracts.
For example, a situation may arise whereby an incomplete spinal cord injury such as a spinal tumour may result in damage to a specific region. The consequent motor loss will be related to the particular descending tract or tracts infiltrated by the tumour (Fig. 14.1) and their specific function (Table 14.1). Depending on the level of decussation, the motor loss may be contralateral or ipsilateral to the lesion.