CHAPTER 52 The Biomechanics of the Cervical Spine during Whiplash Injury
INTRODUCTION
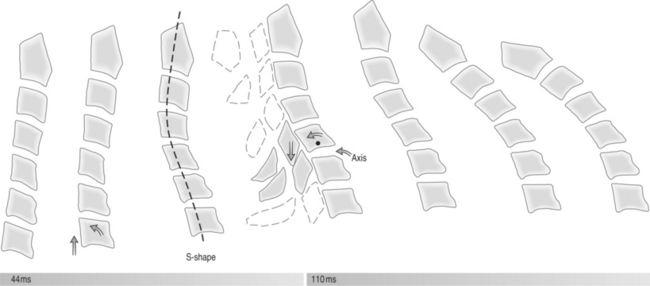
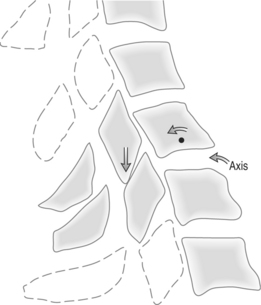
The injury mechanism associated with ‘whiplash-associated disorder’1 has been studied for over 40 years. Cervical spine injury associated with rear-end collision was first described in 1867 with railroad workers, the so-called ‘railroad spine.’ In 1928, Crowe described the cervical spine injury associated with rear-end automobile collisions.2 The theories hypothesizing the biomechanical injuries have evolved from early years when the mechanism of injury was thought to be simple cervical hyperextension.3–6 Cadaveric, anthropomorphic, and animal (including human) studies as well as mathematical models have all been used to further investigate the biomechanical events that occur during whiplash injuries. The majority of these studies focus on the association between motion and injury to the cervical spine that occurs during rear-end impact, simulating motor vehicle collisions. Factors that affect energy transfer are the basis for injury to the cervical spine in these collisions. It has become more apparent through these studies that the mechanism of injury to the cervical spine is not, in fact, simply cervical hyperextension or hyperflexion as was once thought.3–6 Investigators have shown through studies of segmental cervical spine motion that an ‘S-shaped’ cervical spine deformation occurs in the sagittal plane at approximately 50–75 ms after impact (Fig. 52.1), which includes abnormal lower cervical spine extension coupled with upper cervical spine flexion, as well as axial cervical spine compression.7–11 It is now felt that this abnormal curvature and compression of the cervical spine is the etiology of the injuries that occur during rear-end collision.
The Quebec Task Force defines whiplash as an ‘acceleration–deceleration mechanism of energy transfer to the neck. It may result from rear-end or side-impact motor vehicle collisions, but can occur during diving or other mishaps.’6 As the majority of published studies that investigate whiplash simulate rear-end collision motor vehicle accidents, this chapter focuses on the biomechanical forces and energy transfer that is associated with rear-end collision.
ANATOMIC CERVICAL SPINE
First, it is important to define the anatomic cervical spine. The cervical spine is the most mobile of any spinal section with the most physiologic lordosis.12 It is generally considered as two functional regions, the upper cervical spine, C0–2, and the lower cervical spine, C3–7 (Fig. 52.2).
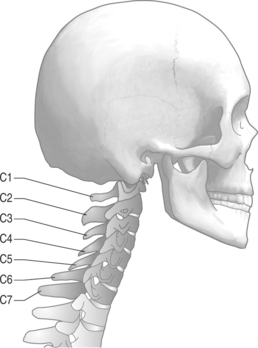
As a functional unit, the upper cervical region can be broken down into two adjacent segments of motion: C0–1 and C1–2. Physiologic motion at the C0–1 level generally accommodates 25° of flexion–extension and 5° of lateral flexion. There are 3–8° of rotation that occurs about the instantaneous axis of rotation.12 Paradoxical extension at C0–1 is observed at end-range cervical spine flexion.13 The C1–2 level accommodates 20° of flexion–extension and 5° of lateral flexion. There is significantly more rotation about the instantaneous axis of rotation, approximately 40° to each side, which accounts for approximately half of the total rotation of the cervical spine.12
The middle and lower cervical spine encompasses the cervical levels C3–7. Physiologic anterior–posterior translation can be up to 2–2.7 mm from the anterior-inferior corner of the moving vertebral body.14 On flexion and extension plain films of the cervical spine, a maximum of 3.5 mm of anterior–posterior translation is accepted as normal (Fig. 52.3). This takes into account approximately 25% magnification due to radiographic technique.9 There is also physiologic coupling in the lower cervical spine between lateral flexion and rotation. Coupling occurs when motion about one axis is accompanied by simultaneous motion around another axis. In the cervical spine, lateral flexion of a vertebra is accompanied by rotation so that the spinous process moves toward the convexity of the developing curve. This coupling pattern changes from the C2 to C7 level, with the more cephalad segments having a higher ratio of rotation to lateral flexion and the more caudal segments having a lower ratio of rotation to lateral flexion.14
BIOMECHANICS OF THE REAR-END COLLISION
Researchers debated for many years as to the pathologic mechanism that leads to whiplash-associated disorder. The prevalent theories revolved around early stage hyperextension and late stage hyperflexion.3–6 These earlier studies investigated cervical spine motion as a whole during rear-end collision. As researchers began to look at individual segmental motion in the cervical spine, the abnormal posturing that occurs throughout the event was found. Grauer first described the abnormal S-shaped cervical spine curvature that occurs during rear-end collisions, with lower cervical spine flexion and upper cervical spine extension.15 The abnormal posture that occurs during this S-shaped curve is now implicated as the most likely etiology of injury in whiplash-associated disorder.9–12,16,17
The sequence of events that occur in rear-end collisions begins with the impact of the bullet vehicle, and ends with complete cervical spine flexion (Table 52.1). The energy transfer that occurs through this process causes the abnormal cervical spine curvature and compression which leads to the cervical spine injury.
Table 52.1 Typical sequence of events in rear-end collisions
Immediately following the collision of the vehicles the first contact with the individual is the seat-back against the lumbar spine and pelvis. The base of the car seat forces the lumbar spine forward inducing lumbar straightening and cephalad axial compression of the spine (Fig.52.4A). Contact between the individual and the seat-back induces a counterforce from the individual’s lumbar spine to the seat-back, causing a ramping effect of the seat. The forward movement of the caudal spine induces relative cervical flexion as inertia of the head resists motion initially and maintains its position in space. There is vertical displacement of the torso from this cephalad compression, as well as downward displacement of the seat-back from this ramping effect. The ramping effect of the seat-back will bring the head restraint down in relation to the cervical spine and head. Thoracic contact with the seat at this point has also been considered as a mechanism for spinal compression, as the kyphotic thoracic spine is forced forward into a flattened posture.8 The clinician should be aware that much of this information comes from crash dummies which are rigid and do not replicate the normal flexible curves of the spine in human beings. In humans, these curves are able to absorb energy, which is not the case in these more rigid hybrid dummies. Matsushita et al.18 were the first to observe thoracic spine straightening during rear-end impact. It is reasonable that the thoracic spine would suffer the greatest kinematic change initially that would transfer compressive forces to the cervical and lumbar spines. The cervical spine would receive compressive forces from both the thoracic spine below and the cranium above. The normal thoracic kyphosis is lost as the seat back transmits forces to the thoracic spine. This results in thoracic straightening and longitudinal transmission of force to both the cervical and thoracic spines. This can result in injury of various structures including the intervertebral discs and the zygapophyseal joints of the cervical, thoracic, and lumbar spines.
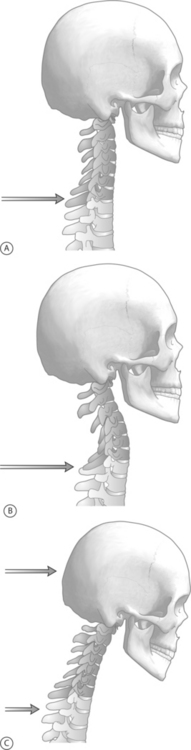
As energy is initially transmitted to the cervical spine, the sequence most often implicated in whiplash-associated disorder is initiated. At this point, the upper cervical spine is in relative flexion due to the forward displacement of the thoracic spine. Studies differ on which levels experience peak rotations, but all agree that forward acceleration and compression from the ascending energy transfer cause lower cervical extension and compression. As the head remains stationary, this induces upper cervical spine flexion. There is significant posterior element stress at the C5–7 region during this phase.7,8,11,12 There is no evidence demonstrating that the upper cervical spine flexion during the S-shaped curve exceeds physiologic flexion (Fig. 52.4B).11
As the torso continues in a forward direction and the relatively large head lags behind, the so called C-shaped curve of complete cervical extension occurs. This phase has been implicated in injury, as the amount of lower cervical hyperextension that occurs exceeds physiologic measures.11 Upper cervical spine extension does not exceed physiologic extension during either the C-shaped curve or the previous S-shaped curve.11 Contact with the head restraint will occur at this point if the head restraint system is positioned properly. Peak horizontal backward acceleration of the head occurs just prior to contact with the head restraint. This peak acceleration may cause the shearing forces associated with any axonal damage that is implicated in rear-end collisions. In addition, following these injuries there is an alteration of the instantaneous axis of rotation (Fig. 52.4C).
The final event that occurs in the sequence follows as the head accelerates forward. Both the upper and lower cervical spine go into complete flexion (Fig. 52.5). Studies investigating segmental motion of the cervical spine have not demonstrated the cervical spine to reach levels of flexion that exceed physiologic cervical flexion.11 Depending on the individual’s restraint system, this stage may end with contact of the head against the steering wheel or windshield.
EFFECT OF MUSCULAR TENSION
Unfortunately, most rear-end impact collisions do not occur under the setting of preparation. Electrodiagnostic studies investigating the reaction time of the cervical spine musculature demonstrate that full contraction occurs at approximately 115–200 milliseconds. The S-shaped cervical spine as well as full hyperextension occur at up to 75 milliseconds.2,18 This suggests that muscular tension in unexpected rear-end collisions will not occur in time to stabilize the cervical spine, and therefore minimize whiplash-associated injuries. Dynamic stabilization via cervical muscular contraction may minimize the abnormal curvature of the cervical spine in rear-end collisions when the individual in the target vehicle is prepared for the impending collision.
COLLISION FACTORS ASSOCIATED WITH WHIPLASH
Vehicle factors
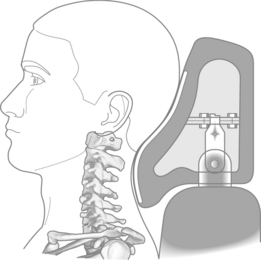
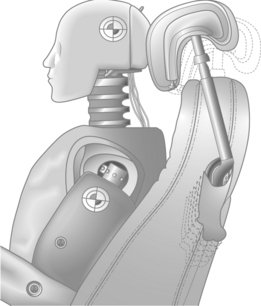
There has been significant debate regarding the standards of the head restraint systems currently being used. Maximum protection for the cervical spine includes a head and neck restraint system that maintains the physiologic lordotic posture of the cervical spine following rear-end impact. Current head restraint systems tend not to protect the lordosis of the cervical spine on rear-end impact, as these restraints are often flat and not positioned correctly (Fig. 52.6). Newer head and neck bolstering systems may minimize injuries to the cervical spine following rear-end impact by maintaining the neck’s physiologic contour (Fig. 52.7).19
Human factors
An individual’s mass and posture potentially change the injury suffered in a rear-end collision. Heavier individuals will have less acceleration for the same amount of force applied, as the energy of a collision is transferred from the seat-back to the lumbar spine. Pre-impact kyphotic postures of the cervical spine will exaggerate the S-shaped curve. Chronic kyphotic posturing may be associated with anterior contractures, which are particularly vulnerable to high-velocity movements. In addition, if the individual head is turned to one direction or another, there are questions regarding how this may influence injury of the underlying soft tissues. It is clear that the loss of cervical lordosis with the development of an S-shaped cervical spine will occur; however, with the cervical spine rotated, this may lead to greater injuries of the intervertebral discs due to torsion and to cervical nerve roots damage due to foraminal narrowing. In addition, cadaveric studies have shown that pre-torque of the capsular ligaments by rotation increases capsular strain when loaded, which may result in increased injury risk of the zygapophyseal joint.12
Females seem to have a predisposition for whiplash-associated disorder. The exact mechanism of this gender-based discrepancy is unclear.20 This may be due primarily to the size of most females compared to males and their body position in the car seat and head position relative to the headrest during driving. A smaller driver would tend to have relatively exaggerated thoracic kyphosis and a head positioned lower down on the headrest, which may actually predispose the driver to cervical spine injuries rather than preventing them. This would suggest that head and neck restraints that can conform to the individual driver would be an important development in the prevention of cervical spine injuries.
1 Seletz E. Trauma and the cervical portion of the spine. J Int Coll Surg. 1963;40:47-62.
2 Crowe HE. Injuries to the cervical spine. Presented at the Meeting of the Western Orthopedic Association, San Francisco, 1928.
3 Brault JR, Wheeler JB, Gunter P, et al. Clinical response of human subjects to rear-end automobile collisions. Arch Phys Med Rehab. 1998;79:72-80.
4 Luan F, Yang KH, Deng B, et al. Qualitative analysis of neck kinematics during low-speed rear-end impact. Clin Biomech. 2000;15(9):649-657.
5 Scifert J, Totoribe K, Goel V, et al. Spinal cord mechanics during flexion and extension of the cervical spine: a finite element study. Pain Phys. 2002;5(4):394-400.
6 Spitzer WO, Skovron MI, Salmi LR, et al. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: Redefining ‘whiplash’ and its management. Spine. 1995;10(Suppl 8):1S-73S.
7 Geigl BC, Steffan H, Leinzinger P, et al. The movement of head and cervical spine during rearend impact. Proceedings of the 1994 International Ircobi Conference on the Biomechanics of Impacts, pp 127–137. Lyons, 1994.
8 Kumar S, Narayan Y, Amell T. Analysis of low velocity frontal impacts. Clin Biomech. 2003;18(8):694-703.
9 Macnab I. Acceleration injuries of the cervical spine. J Bone Joint Surg. 1964;46A:1797-1799.
10 Gay R, Levine R. Biomechanics of whiplash. In: Malanga GA, Nadler SF, editors. Whiplash. Philadellphia: Hanley & Belfus, 2002.
11 Panjabi MM, Cholewicki J, Nibu K, et al. Simulation of whiplash trauma using whole cervical spine specimens. Spine. 1998;23(1):17-24.
12 White AA, Johnson RM, Panjabi MM, et al. Biomechanical analysis of clinical stability in the cervical spine. Clin Orthop. 1975;109:85-96.
13 Panjabi MM, Pearson AM, Ito S, et al. Cervical spine curvature during simulated whiplash. Clin Biomech. 2004;19(1):1-9.
14 Versteegen GJ, Kingma J, Meijler WJ, et al. Neck sprain after motor vehicle accidents in drivers and passengers. Eur Spine J. 2000;9:547-552.
15 Grauer JN, Panjabi MM, Cholewicki J, et al. Whiplash produces an S-shaped curvature of the neck with hyperextension at lower levels. Spine. 1997;22(21):2489-2494.
16 Harrison DD, Janik TJ, Troyanovich SJ, et al. Comparisons of lordotic cervical spine curvatures to a theoretical ideal model of the static sagittal cervical spine. Spine. 1996;21(6):667-675.
17 Kaneoka K, Ono K, Inami S, et al. Motion analysis of cervical vertebrae during whiplash loading. Spine. 1999;24(8):763-769.
18 Matsushita T, Sato TB, Hirabayashi K, et al. X-ray study of the human neck motion due to head inertia loading.
19 Foust DR, Chaffin DB, Snyder RG, et al. Cervical range of motion and dynamic response and strength of cervical muscles. In: Backaiatis SH, editor. Biomechanics of impact injury tolerances of the head-neck complex. Warrendale, PA: Society of Automotive Engineers; 1993:1023-1035.
20 Barnsley L, Lord S, Bogduk N. Pathophysiology of whiplash. In: Malanga G, Nadler S, editors. Whiplash. Philadelphia: Hanley and Belfus, 2002.
1 Clemens HJ, Burow K. Experimental investigation on injury mechanisms of the cervical spine at frontal and rear-frontal vehicle impacts. Proceedings of the 16th STAPP Car Crash Conference. Warrendale, PA: Society of Automotive Engineers, 1972;76-104.
2 Penning L. Normal kinematics of the cervical spine. Clinical anatomy and management of cervical spine pain, Vol 3 . Butterworth-Heinemann, Oxford, 1998;51-55.
3 States JD, Korn MW, Maengill JB. The enigma of whiplash injuries. AAAM. 1969;84:12.
4 White AA, Panjabi MM. Clinical biomechanics of the spine, 2nd edn. Philadelphia: JB Lippincott, 1990.
5 Winkelstein BA, Nightingale RW, Richardson WJ, et al. The cervical facet capsule and its role in whiplash injury. Spine. 2000;25:1238-1246.
6 Yoganandan N, Pintar FA, Stemper BD, et al. Single rear impact produces lower cervical spine soft tissue injuries.






