The ascending tracts
Basic anatomy and function of the main ascending tracts
The main ascending tracts include:
Basic structure of an ascending tract
Sensory receptor
A 1st order neuron which is an afferent/sensory neuron in the peripheral nervous system. Its cell body is found in the dorsal root ganglion and it enters the spinal cord via the dorsal root. These neurons synapse on the 2nd order neuron
A 2nd order neuron which decussates and ascends the spinal cord in white matter to higher levels of the nervous system. These neurons synapse on the third order neuron
A 3rd order neuron usually arises from the thalamus and terminates in the somatosensory region of the parietal lobe of the cerebral cortex (S2.7). Of course those tracts that do not reach the cerebral cortex will terminate in other regions.
Knowledge of the basic structure and especially where each tract decussates is important in understanding the clinical presentation of a patient with a lesion involving the spinal cord. The precise detail of the individual ascending tracts is beyond the scope of this book, however the function of each tract is shown in Table 15.1.
Table 15.1
Basic function of the main ascending tracts
| Name of tract | Function |
| Lateral spinothalamic | Free nerve endings provide pain and temperature information. At the level of the thalamus crude pain is perceived, however it cannot be localized (i.e. its location identified) accurately. This is only possible upon reaching the primary sensory area of the cerebral cortex (parietal lobe). The slow pain travelling in C fibres is also harder to localize than fast pain in A delta fibres. |
| Anterior spinothalamic | Free nerve endings provide information related to touch and pressure. At the level of the thalamus only a crude sensation is perceived. Conscious awareness is possible upon reaching the primary sensory area of the cerebral cortex (parietal lobe), however localization remains crude and discrimination of intensity is poor. |
| Posterior/dorsal columns | This tract carries information related to touch, two-point discrimination and proprioception to the cerebral cortex (parietal lobe). Conscious awareness is possible upon reaching the cerebral cortex and in this case localization is more precise. Information ascending in fasciculus gracilis represents the lower limb and in fasciculus cuneatus, the upper limb. |
| Posterior spino- cerebellar tract | Muscle spindles and stretch receptors in the skin provide information related to position and movement of the ipsilateral lower limbs and trunk to the cerebellum to achieve smooth coordinated movement. As this information does not reach the cerebral cortex, it is non-conscious. |
| Anterior spino- cerebellar tract | Muscle spindles and stretch receptors in the skin provide information related to position and movement of the ipsilateral upper limbs and trunk to the cerebellum to achieve smooth coordinated movement. As this information does not reach the cerebral cortex, it is non-conscious. |
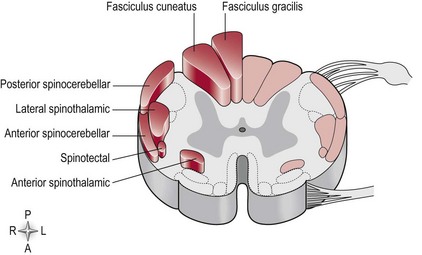
Figure 15.1 represents the anatomical orientation of the ascending tracts within the white matter of the spinal cord. This is highly relevant in terms of a patient’s clinical presentation in conditions affecting the spinal cord. For example, a situation may arise whereby an incomplete spinal cord injury due to a spinal tumour may result in damage to a specific region. The consequent sensory loss will be related to the particular ascending tract or tracts infiltrated by the tumour (Fig. 15.1) and the specific function of the tract (Table 15.1). Depending on the level of decussation the sensory loss may be contralateral or ipsilateral to the lesion.